Open Access version via Utrecht University Repository
advertisement

PTEN as a regulator of
the PI3K/AKT pathway
Involvement of a growth- and survival pathway in the development
of autism spectrum disorders
I.N. de Bruin
July 2011
Supervisor: Prof. Dr. J.P.H. Burbach
Cover picture: The knowledge that PTEN is involved in some cases of autism brought us one small
step closer to solving the puzzle of autism spectrum disorders. Further research will probably learn us
more about the causes and underlying mechanisms of ASD.
July 4, 2011
Ilse N. de Bruin
Supervisor: Prof. Dr. J.P.H. Burbach
Bacherlor thesis Biomedical Sciences
2
Contents
Abstract
4
Introduction
5
Literature Study
6
Autism Spectrum Disorders
ASD and PTEN
PTEN
The Pathway regulated by PTEN
Consequences of aberrant PTEN expression
Treatment of patients with PTEN mutations
Other mutations in the PI3K/AKT Pathway
Practical Part
Introduction
Material and Methodes
Results
Discussion
6
7
8
10
13
17
17
19
19
19
20
Conclusion
23
Acknowledgements
25
References
26
Supplementary Material
29
Supplement 1
Supplement 2
Supplement 3
29
31
32
3
Abstract
Autism spectrum disorders (ASD) are a complex group of neurodevelopmental disorders,
characterized by difficulties in social relationships and abnormal behaviors. Although ASD is known to
be highly heritable, the underlying genetic factors remain to be unknown for most of the cases. The
tumor-suppressor gene PTEN is one of the few genes for which an association with ASD is proven. It
is known that disturbance of its function as a regulator of the growth-stimulating PI3K/AKT pathway
can result in ASD. However, much has to be learned about the precise mechanism by which PTEN
mutations can lead to the disorder. In this thesis, an overview of the current information about
PTENs involvement in the development of ASD is provided. Besides, a database search is performed
to explore if mutations in other players in the PI3K/AKT pathway are involved in the development of
ASD. The results of this study suggest that besides PTEN, no other players in the PI3K/AKT pathway
have a significant role in the cause of ASD.
4
Introduction
Autism Spectrum Disorders (ASD) are a complex group of neurodevelopmental disorders
characterized by impaired social skills and abnormal behaviors. In most of the individuals with ASD,
the cause of their condition is still unknown. Research has indicated that genetic factors are involved
in the development of the disorder in most of the cases. However, it is generally accepted that ASD is
no monogenetic disorder but can be caused by a variety of mutations in many different genes.
Phosphatase and tensin homologue deleted on chromosome 10 (PTEN), originally known as a tumor
suppressor, is expected to be one of these genes. By regulating the PI3K/AKT pathway, PTEN is
involved in important processes in brain development, including regulation of growth and neuronal
migration. The aim of this thesis is to find out what the role of PTEN in development of the normal
developed and autistic brain is, by answering the following question:
What is the influence of mutations in PTEN on the PI3K/AKT pathway and how are these mutations
associated with autism spectrum disorders?
To make this question more specific, the following sub-questions will be answered:
o What does the PI3K/AKT signaling pathway look like in brain tissue and what is the role of
PTEN in it?
o Which processes are regulated by the PI3K/AKT signaling pathway?
o How do the alterations in the PI3K/AKT pathway play a role in the development of ASD?
o Are there, besides in PTEN itself, mutations in other genes involved in the PTEN signaling
pathway seen in ASD patients?
First, a literature study was performed to consider the information about PTEN available in the
literature. The results of this study are reviewed in the first part of this thesis.
The second part of this research consists of a report of a little practical work. To get a better view at
the heterogeneity of ASD in real live, I saw five of the patients of a child psychiatrist. The reports of
my observations can be found in the supplementary material of this thesis. The other part of my
practical work consists of a database search in the Autism Genome Resource Exchange (AGRE)
database. This database contains the micro-array data of about 4000 people, consisting of 1000
patients and their relatives. To answer the last sub-question, for four important genes in the
PI3K/AKT pathway was checked whether copy number variations (CNVs) were present in ASD
patients.
5
Literature Study
Autism Spectrum Disorders
In 1943, the child psychologist Leo Kanner and psychiatrist Hans Asperger were the first to describe
children affected by a neurodevelopmental disorder they called autism(Kelleher and Bear 2008;
Schaaf and Zoghbi 2011). Since then, it has become clear that autism is a heterogeneous group of
disorders that can collectively be termed autism spectrum disorders (ASDs). The most common forms
of ASD are classical autism, Asperger syndrome and pervasive developmental disorder-not otherwise
specified (PDD-NOS)(Baltussen, Clijsen, Leenders 2003). Individuals with an ASD can be characterized
by impairment in social relationships, atypical verbal and non-verbal communication, difficulties with
imaginary thoughts and stereotypic behaviors (Baltussen, Clijsen, Leenders 2003; Bourgeron 2009;
Kelleher and Bear 2008; Levitt and Campbell 2009; O'Hare 2009; Toro and others 2010). The degree
of severity of symptoms can vary between the different forms of ASD, but also differs extremely
between individuals with the same disorder(Levitt and Campbell 2009).
Besides the characteristic ASD symptoms, a broad range of other features are seen in individuals with
the disorder. Most of the children with ASD are cognitively impaired as well, about 70% of them has
an IQ score below 70(Baltussen, Clijsen, Leenders 2003; Kelleher and Bear 2008). Macrocephaly is
seen in 10-30% of the individuals with ASD. At birth, the head circumference usually appears normal,
the overgrowth of brain tissue develops during the first four years of life(Bourgeron 2009). The
pathogenesis of this overgrowth is still not unraveled(Buxbaum and others 2007). About 10-30% of
the patients with ASD suffers from epilepsy(Bourgeron 2009), 10% of the individuals exhibits socalled “savant abilities”(Kelleher and Bear 2008). Savant abilities are defined as normal or superior
skills in individuals with cognitive disability. These skills can involve a broad range of cognitive and
artistic skills, but superior skills in declarative memory are most seen(Kelleher and Bear 2008).
Besides these features, co-occurrence of medical conditions like sleeping disorders and
gastrointestinal problems, or psychiatric problems such as anxiety, aggression and obsessivecompulsive disorder are common in ASD(Levitt and Campbell 2009).
Autism spectrum disorders are diagnosed in about one in hundred children, which means that worldwide about 1% of the children is affected(Toro and others 2010). Although there are some
discrepancies between different studies after the prevalence of ASD, it is clear that ASD are among
the most common neuropsychiatric disorders. ASD are more common in males than in females, with
a ratio of 4:1(Toro and others 2010) It is not yet known what causes this compelling
difference(Schaaf and Zoghbi 2011), but the hypothesis is that the perturbations to trigger autism in
females have to be stronger compared to males(Gilman and others 2011). This hypothesis is
supported by the recent observations that copy number variations (CNVs) in females are significantly
larger, contain more genes and that the genes involved are more functionally important(Gilman and
others 2011). ASD is usually diagnosed before the age of 3 years, especially when it co-occurs with
mental retardation(Pardo and Eberhart 2007). The disorder is seldom curable, but interventions van
be very helpful for the patients as well as their families(O'Hare 2009).
Although the causes of ASD have been an important topic of research for a while, the underlying
cause of the disorder remains unknown in the majority of patients (Fig.1). What we do know, is that
ASD has a strong and complex genetic component and that it is highly heritable, with heritability
indices estimated at 85-92%(Buxbaum and others 2007; Schaaf and Zoghbi 2011). The first steps in
6
identifying the genetic causes of ASD came from studies about syndromic autism, a term used for
disorders caused by single-gene mutations that are associated with autism. Although just about 10%
of the individuals with an ASD are diagnosed with syndromic autism, these disorders may learn us
much about the possible genetic basis of other forms of autism(Pinto and others 2010; Schaaf and
Zoghbi 2011). About the causes of non-syndromic or idiopathic autism, significantly less is known.
Recent studies identified that in about 7-20% of the individuals with idiopathic autism, the disorder is
caused by copy number variations (CNVs)(Schaaf and Zoghbi 2011). These CNVs were found in a
variety of genes, which supports the suggestion that autism is mostly caused by rare
mutations(Schaaf and Zoghbi 2011). Another recent association is that of ASD with several metabolic
conditions. Besides genetic causes for autism, the involvement of environmental factors in the
pathogenesis of ASD is also considered(Pardo and Eberhart 2007).
Figure 1. Causes of autism spectrum disorders{{39 Schaaf,C.P. 2011}}
This diagram represents the causes of ASD that are known nowadays. Although there are some
disagreements about the exact percentages, all authors agree that in most of the patients, the cause
of autism is still unknown.
ASD and PTEN
One of the genes that is associated with autism spectrum disorders is PTEN. PTEN mutations were
first found in patients with Cowden syndrome, an inherited form of cancer predisposition(Butler and
others 2005). In addition to the increased risk of cancer, mental retardation was reported in 12% of
the individuals with Cowden syndrome (CS). Furthermore, PTEN germ line mutations have been
found in patients with hamartoma syndromes. The benign tumors seen in these syndromes are often
accompanied by hallmark signs like macrocephaly, mental retardation and delayed motor
development. In several patients with PTEN mutations, autistic behaviors were observed by separate
researchers as well. These observations in combination with the data that macrocephaly is seen in
20% of the ASD patients, led to the hypothesis that there might be an association between
macrocephaly, autistic behavior and PTEN mutations.(Butler and others 2005)
Inspired by this hypotheses, different studies about the role of PTEN in the development of ASD were
performed. Among the first of these studies was the study of Butler et al., in which they undertook
PTEN mutation analysis in 18 subjects with ASD and macrocephaly(Butler and others 2005). The
three subjects with the largest head circumference turned out to have mutation is the PTEN gene,
which indicates that PTEN mutations might not only be involved in the development of ASD, but are
7
also associated with macrocephaly. Other studies started to mention the link between PTEN an ASD
as well(Kwon and others 2006; van Diepen and Eickholt 2008), while researchers were working on
more adequate prove for this hypothesis. Indeed, later studies showed that mutations in PTEN are
found in about 5% of the patients with ASD and macrocephaly(Buxbaum and others 2007; Kelleher
and Bear 2008). Nowadays, the appearance of macrocephaly as a cause of PTEN mutations has been
termed the PTEN macrocephaly syndrome. This syndrome is estimated to be the cause of ASD in
approximately 1% of the cases(Schaaf and Zoghbi 2011). The link between PTEN, macrocephaly and
ASD is nowadays generally accepted, but the exact mechanisms via which they influence each other
remain a secret. In this essay, the recent knowledge about the pathway regulated by PTEN and the
mechanisms via which PTEN deficiency can cause autism are discussed.
PTEN
In 1997, phosphatase and tensin homologue deleted on chromosome 10 (PTEN) was discovered by
three different groups as being a tumor-suppressor gene located on chromosome 10q23(Stiles
2009).PTEN and its network regulate the signaling cascade from stimulation of a tyrosin kinase
receptor until the activation of transcription factors in the nucleus, thereby interacting with other
pathways(Keniry and Parsons 2008). One of these pathways is the p53 pathway, which regulated
apoptosis and is known to be deregulated most tumors. The most important pathway regulated by
PTEN is the phosphatidylinositol-3-kinase (PI3K)/AKT pathway(Stiles 2009).The PI3K/AKT pathway is
involved in many cellular processes, including cell growth, metabolism and survival.(Carracedo and
Pandolfi 2008) In this pathway, the function of PTEN is to dephosphorylate the phospholipid
phosphatidylinositol (3,4,5)-trisphosphate (PIP3)(Tamguney and Stokoe 2007). Since PIP3 is the
product of PI3K, PTEN is an important PI3K antagonist(Tamguney and Stokoe 2007). Besides its most
well known function as a PIP3 phosphatase, PTEN has some other functions. PTEN is also able to
dephosphorylate other phospholipids, as well as some protein substrates and itself(Tamguney and
Stokoe 2007). Although PTEN is mainly known for its function as a tumor suppressor, more recent
studies have revealed an important role for PTEN in brain development. Studies in neural stem cells
demonstrate that PTEN negatively regulates the size and proliferation of these stem cells (Rodgers
and Theibert 2002). According to other studies, PTEN also influences neuronal growth and survival,
neurite outgrowth, protein synthesis in dendrites, synaptic plasticity, learning and memory(Buxbaum
and others 2007; Jaworski and others 2005). In addition to its function in neural development, PTEN
also regulates neural stem cells in adult brains, where it has an important function in the self-renewal
of stem cells and neurogenesis(Qu and Shi 2009). Although PTEN is still best known for its function as
a tumor-suppressor, it also has an important role in the development and maintenance of the
nervous system.
The PTEN protein consists 403 amino acids and is composed of three different domains: a N-terminal
catalytic phosphatase domain, a C2 domain and the C-terminal tail region (Fig. 2)(Das, Dixon, Cho
2003; Tamguney and Stokoe 2007). The function of the C2 domain is to dephosphorylate PIP3(Stiles
2009). Together with the N-terminal phosphatase domain, the C2 domain forms a catalytical unit,
involved in the binding of PTEN to the membrane. The tail region of PTEN is a region that contains
several phosphorylation sites. The role of the C-terminal tail region is not completely clear. It is
proposed that it might modulate the stability of PTEN, but it might also have a function in membrane
localization of PTEN (Das, Dixon, Cho 2003).
(Lee and others 1999)
8
Figure 2. The PTEN structure
Overall view of the PTEN structure. PTEN is a protein consisting of three domains: the N-Terminal
Phosphatase domain, the C2 Domain and a small C-terminal tail-region. The dotted line indicates
the region deleted in the crystal structure of the protein.{{25 Lee,J.O. 1999}}
When the PTEN protein was discovered, it was reported to be a protein exclusively located in the
cytoplasm. More recent evidence showed that PTEN can be both a cytoplasmic and nuclear(Stiles
2009). Nuclear located PTEN functions in chromosome stability, DNA repair, cell cycle arrest and
cellular s(Planchon, Waite, Eng 2008)tability(Planchon, Waite, Eng 2008) and seems to be
independent of its lipid phosphatase activity. This lipid phosphatase activity seems to be a feature
limited to the cytoplasmic form of PTEN. Switching between the two locations can occur and is based
on ubiquitination(Stiles 2009). For its function as PIP3 phosphatase, PTEN has to be recruited in the
plasma membrane. This is because phosphatidylinositides, among which PIP3, are located in the
plasma membrane. (Tamguney and Stokoe 2007). Because the function of PTEN in the PI3K/AKT
pathway is performed by cytoplamic PTEN, the nuclear function will no further be evaluated.
The PTEN protein typically has a relatively long half-life of 48-72 hours(Wu and others 2000). The life
span and activity of PTEN are further regulated by several events. This complex combination of
regulatory events ensures that PTEN influences the important PI3K/AKT pathway in the exact right
way.
First of all, transcription of the PTEN gene is regulated by several transcription factors. These
transcription factors take care of positive as well as negative regulation of PTEN(Tamguney and
Stokoe 2007). The transcriptional control together with translational control mechanisms ensure that
sufficient PTEN protein is available.
Besides regulation of the amount of PTEN protein present, there are mechanisms that regulate the
activity and stability of the present amount of protein. Posttranslational modifications
(phosphorylation, acetylation, ubiquitination, oxidation and caspase activity) play an important role
in regulating protein activity (Keniry and Parsons 2008; Stiles 2009). But besides protein activity,
these posttranslational modifications also affect the incorporation of PTEN in protein complexes, the
subcellular localization and protein stability(Keniry and Parsons 2008). As mentioned before, the
subcellular localization of PTEN is another important factor in the regulation of its phosphatase
activity. The localization of PTEN is controlled by posttranslational modifications like ubiquitination
and phosphorylation and by interaction with other proteins(Tamguney and Stokoe 2007). The
interaction with other proteins may also influence PTEN stability and thereby modulate PTEN levels.
For example, the interaction between PTEN and tumor suppressor protein p53 promotes PTEN
degradation(Tamguney and Stokoe 2007).
9
PTEN expression can be detected early during the blastocyst stage of embryonic development, which
commences on embryonic day 3,5(Stiles and others 2004). The observation of PTEN expression this
early in development suggests a major role for this gene in development. Therefore, a broad range of
effects would be suspected the expression is altered. Indeed, mutations and deletions in PTEN result
in a large amount of possible alterations in development, including macrocephaly, hamartomas
(benign malformations), cancer predisposition and different neurological abnormalities(Kwon and
others 2001). These findings indicate that correct PTEN expression is important for development to
occur correctly. The consequences of aberrant PTEN expression will be discussed more detailed later
in this thesis.
The pathway regulated by PTEN
Fourteen years after the discovery of PTEN, regulating the PI3K/AKT pathway is still seen as its most
important function(Planchon, Waite, Eng 2008; Stiles and others 2004). This explains why, when the
PTEN pathway is mentioned, this usually refers to the PI3K/AKT pathway regulated by PTEN. The
pathway described here will be the PI3K/AKT pathway as it is regulated by PTEN.
After it became clear that there was a possible relationship between the PI3K/AKT pathway and
cancer, the pathway was extensively studied in tumor tissue. The exact function of this pathway in
brain tissue is studies less extensive and must still be unraveled. What we do know yet, is that the
essentials of this pathway are quite similar in different kinds of tissue. Therefore, only the pathway as
it occurs in neurons will be discussed here. The pathway will be extensively discussed below and is
summarized in figure 3.
First, it is important to know a little more about the protein PI3K. PI3K is not one single protein, but
forms a family of eight heterodimeric phosphatidylinositol kinases. Each kinase is compsed of a
regulatory and a catalytic subunit that are encoded by different genes. The eight members are
divided into three different classes: class I, II and III PI3Ks. Class I PI3Ks are the kinases that catalyses
the phosphorylation of the phospholipid PIP2, thereby converting PIP2 into PIP3. The class I PI3Ks
consist of two subgroups, the IA and the IB PI3Ks. Members of class IA transmit signals from the
receptor tyrosin kinase, members of IB from the G-protein coupled receptor. The regulatory subunits
of PI3K class 1A are encoded by three different genes(Vivanco and Sawyers 2002). Taken this
information together, PI3K is a group of proteins that is encoded by a broad range of genes.
The PI3Ks involved in the PI3K/AKT pathway, are members of the class IA PI3Ks (Vivanco and Sawyers
2002).
The PI3K/AKT pathway starts with the stimulation of the receptor tyrosin kinase (RTK) on the cell
membrane by the binding of a growth factor, trophic factors, neuregulin (members of the EGF
family), cytokine or neurotransmitter(Rodgers and Theibert 2002). Inactive PI3K binds to the
stimulated RTK and is activated. For this activation, many RTKs need to recruit adaptor proteins such
as insulin receptor substrate (IRS) 1/2(Rodgers and Theibert 2002). Multiple adaptor proteins van
form an adaptor complex, which can activate PI3K in two ways. First, the adaptor complex can recruit
PI3K to the plasma membrane, which is the place where PI3K has to be to fulfill its function as a PIP2
kinase. Second, adaptor complexes can activate Ras, which binds to PI3K and stimulates its catalytic
activity. Activation of PI3K by Ras and adaptor proteins appears to be critical in the nervous
system(Rodgers and Theibert 2002). PTEN can antagonize PI3K by dephosphorylating PIP3 into PIP2,
hereby lowering the intracellular PIP3 levels. By this action, PTEN blocks the RTK signaling pathway
from propagating downstream(Stiles 2009).
10
The activated PI3K starts converting PIP2 into PIP3 by phosphorylating PIP2(Stiles 2009). In resting
cells, the PIP3 levels normally are low but increase upon growth factor signaling via RTKs (Keniry and
Parsons 2008). PIP3 serves as a second messenger which can bind to a subset of kinases that contain
a pleckstrin homology (PH) domain(Keniry and Parsons 2008; Vivanco and Sawyers 2002). Among
these kinases, phosphoinositide-dependent protein kinase 1 (PDK1) and AKT are quite important.
The binding of PIP3 to the PH domain of AKT allows exposure of the residues that are critical for its
activation. Phosphorylation of these residues by PIP3-bound PDK1 leads to full kinase activity of AKT
(Keniry and Parsons 2008; Stiles 2009)
When the serine/threonine kinase AKT is activated, it can fulfill a broad range of functions. A
summary of these functions can be found in figure 3. The AKT protein can therefore be seen as an
important intersection in the cell, which is crucial in many processes. The processes AKT functions in,
differ from metabolism to cell growth to apoptosis. To accomplish this range of effects, AKT mediates
the activation and inhibition of a large amount of targets by phosphorylating them(Keniry and
Parsons 2008; Stiles 2009). Here, the focus will be on the functions of AKT in brain development and
adult neurons. Some of the important proteins downstream of AKT in the PI3K/AKT pathway will be
discussed.
Figure 3. The PI3K/AKT pathway
Intracellular signaling after activation of the RTK. When the RTK is stimulated, it activates PI3K. PI3K
converts PIP2 into PIP3, a second messenger that together with PDK-1 can activate AKT kinase. AKT had
several targets that play roles in various important cellular processes. PTEN antagonizes the function of
PI3K by converting PIP3 back into PIP2. RTK, receptor tyrosine kinase; PI3K, phosphatidylinositol-3kinase; PDK-1 Pyruvate dehydrogenase kinase 1; GSK3β, glycogen synthase kinase-3β; TSC2, tuberous
sclerosis protein 2; CREB, cAMP response element-binding; BAD, Bcl-2 associated death protein; FOXO,
forkhead transcription factor; MDM2, murine double minute. Adapted from (Stiles 2009)
11
One of the most important functions of PI3K/AKT pathway in nerve tissue is the regulation of
apoptosis. Because neurons do not divide, it is very important that cells do not die unnecessary. On
the other hand, cells with irreparable damage must not be allowed to survive with regard to the risk
of developing a tumor. AKT is one of the proteins that regulates the complex process of apoptosis. If
high amounts of AKT are present, apoptosis will be inhibited. To arrange this anti-apoptotic situation,
AKT activates and inhibits a range of targets by phosphorylating them(Rodgers and Theibert 2002).
To prevent cells from going into apoptosis, AKT inhibits different pro-apoptotic factors(Stiles 2009).
One of these factors is the Bcl-2 associated death protein (BAD) (Fukunaga and Kawano 2003). Apart
from its regulation by AKT, BAD is also regulated by the proto-oncogen Ras (Keniry and Parsons
2008). The forkhead transcription factor family FOXO is inhibited by AKT too(Keniry and Parsons
2008). FOXO can activate apoptosis by moving to the nucleus, where it can transcribe pro-apoptotic
genes. AKT phosphorylates FOXO, after which it can no longer enter the nucleus(Fukunaga and
Kawano 2003).Besides blocking its ability to transcribe pro-apoptotic genes, the phosphorylation of
FOXO also has an effect on cell proliferation(Stiles 2009). The third target inhibited by AKT are the
pro-apoptotic caspases, that form the fatal pores in the mitochondrium of an apoptotic cell (Stiles
2009). Glycogen synthase kinase-3β (GSK3β) is a negative regulator of the cell cyclus with proapoptotic features (Keniry and Parsons 2008; Rodgers and Theibert 2002). AKT inactivates GSK3β,
which leads to the activation of glycogen synthase and β-catenin(Stiles 2009). Glycogen synthase is
one of the targets in the PI3K/AKT pathway that functions in cell metabolism.
A target that is inactivated rather that inhibited by AKT is tuberous sclerosis complex 1/2 (TSC1/2). To
fulfill their function as a Ras homolog enriched in brain - GTPase-activating protein (RHEB-GAP), TSC1
and TSC 2 have to bind to each other(Keniry and Parsons 2008). When TSC2 is phosphorylated by
AKT, the subunits cannot bind anymore. This inactivation of TSC2 can also be performed by Ras. Both
the inactivation of TSC2 by AKT and by Ras result in inhibition of RHEB-GAP activity. Active RHEB-GAP
prevents the presence of active mTOR in the complex called MTORC1(Keniry and Parsons 2008). This
means that by the inactivation TSC2, AKT makes mTORC1 activity possible. mTOR is, just as AKT, an
important player in multiple pathways. In the PI3K/AKT pathway, mTOR phosphorylates some
important regulators of protein translation(Jaworski and others 2005). A specialty of mTOR is that it
can also enhance AKT(Keniry and Parsons 2008), thereby creating a positive feedback loop.
Other proteins that are activated by AKT expression are cAMP response element-binding (CREB) and
NFκB. CREB is a transcription factor for proteins that promote neuronal survival, among which brainderived neurotrophic factor (BDNF) and the cytokines(Fukunaga and Kawano 2003; Rodgers and
Theibert 2002)(Fukunaga and Kawano 2003). NFκB is a nuclear factor that promotes neuronal
survival by inactivating the pro-apoptotic caspases (Fukunaga and Kawano 2003; Rodgers and
Theibert 2002).
The last two proteins regulated by AKT that will be discussed here, are p53 and MDM2. PTEN and
p53 participate in the same pathways and can interact and regulate each other directly and
indirectly(Stiles 2009). This regulation can occur via quite a broad range of mechanisms, of which a
few will be described here. First of all, PTEN can directly regulate p53 transcription and protein levels
via phosphatase-dependent as well as phosphatase-independent mechanisms. PTEN can also
modulate p53s DNA binding activity, which influences p53s transcriptional activity. The other way
round, p53 seems to influence PTEN transcription levels by binding its promoter region. Besides,
these two proteins can influence each other by physical interaction(Freeman and others 2003). The
indirect regulation of p53 by PTEN can occur via AKT. When AKT is activated, it has a stimulating
effect on p53 degradation. The key player in this degradation is the protein MDM2. Activated AKT
12
can phosphorylate MDM2, which induces its activity. The function of MDM2 is to ubiquitinate p53,
which leads to p53 proteolysis. If AKT activaty increases as a consequence of PTEN deletion, MDM2
will be more active and p53 degradation increases(Freeman and others 2003). In summary, it is
obvious that PTEN and p53 influence each other, but our knowledge about the exact mechanisms
involved is not yet complete.
As mentioned in the description of PTEN, the pathway regulated by PTEN interacts with pathways
influenced by p53. As all processes in the cell, the PI3K/AKT pathway is not a static process but is
subject to interactions with other pathways and proteins. For example, AKT is a protein that is
involved in many processes. Alterations in its expression will therefore not only influence the
PI3K/AKT pathway, but have also effect on a lot of other cellular processes and pathways. An
example of a substrate of AKT that is also involved in another pathway is the protein GSK3β. This
protein is a player in the PI3K/AKT pathway as well as in the WNT signaling pathway, which is
involved in diverse processes associated with the formation of neuronal circuits and in regulation of
dendrite morphogenesis(Gilman and others 2011; Stiles 2009). Besides the WNT signaling pathway,
interactions between the PI3K/AKT pathway and the reelin pathway and the MAPK3/ERK pathway
are shown(Gilman and others 2011; Schaaf and Zoghbi 2011). The reelin pathway regulates dendritic
spine morphogenesis, the MAPK3/ERK pathway functions in proliferation, differentiation, and cell
cycle progression. There also are several pathways, including WNT and reelin, that play roles in
neuron motility(Gilman and others 2011). Another type of interaction with other pathways is the
relationship between serotonin and the PI3K/AKT pathway. Serotonine may be, just as PTEN, a
modulator of the PI3K/AKT pathway. This suggestion is based on the fact that serotonin mutations
can also cause macrocephaly and abnormal behavior(Bourgeron 2009). These are some examples of
interactions between the PI3K/AKT pathway and other cellular processes. In the complex machinery
of the cell, there are hardly any proteins that have just one function. Therefore, the PI3K/AKT
pathway cannot be seen as an isolated process. It always has to be taken in account that if the
expression of one protein in the pathway is affected, this almost certainly has effect on other cellular
processes. This is why it is will be complicated to cure a genetic defect like ASD by the inhibition of
certain proteins or genes without causing unwished side-effects. (Stiles and others 2004; Stiles 2009)
Consequences of aberrant PTEN expression
The PI3K/AKT pathway is crucial for the development of neuronal circuits and the maintenance of
individual neuronal architecture in the adult brain.(van Diepen and Eickholt 2008) Based on this
information, it is not hard to imagine that incorrect control of this pathway could have disastrous
consequences. Indeed, mutations and deletions in PTEN result in a large amount of possible
alternations in development. Mice heterozygous for PTEN or with germ line PTEN mutations show a
broad range of phenotypic features, including macrocephaly, hamartomas (benign malformations),
cancer predisposition and different neurological abnormalities(Kwon and others 2001). Since PTEN is
one of the main regulators of the PI3K/AKT pathway, it is interesting to further observe the
consequences of aberrant PTEN expression on the developing and the adult brain.
To define aberrant expression, it first has to be known where PTEN is expressed during and after
development in a healthy brain. The highest levels of PTEN expression are seen during development
of the brain. PTEN expression is seen as early as in the embryonic stem cell stage, which commences
13
on embryonic day 3,5 (Stiles and others 2004). PTEN expression is detected in both embryonic and
extraembryonic tissue. Until embryonic day 11, PTEN is expressed ubiquitously. But from day 15, the
expression becomes restricted to the central nervous system (CNS), liver, heart, skin and
gastrointestinal tract(Stiles and others 2004).
In the adult brain, PTEN expression is mainly seen in the neuronal stem cells and in the granule
neurons of the cerebellum and the dentate gyrus (Kwon and others 2001). Granule cells are small
neurons that vary a lot in both function and anatomy between different brain structures. The granule
cells in the cerebellum are the most numerous neurons in the brain. They receive and integrate
information from the brain stem via the mossy fibers. In response, the granule cells send an
excitatory signal to the Purkinje cells, which eventually arrange the fine coordination of motor
activity. In the dentate gyrus, the granule cells receive information from the ethorinal cortex. They
integrate this information and signal to the CA3 pyramidal cells in the hippocampus. The
hippocampus, as a part of the limbic system, is involved in emotions, behavioral control and memory
storage(Purves and others 2008). Expression of PTEN in glial cells, in Purkinje cells and in astrocytes
in brainstem, thalamus and striatum has been observed only in very small amounts, which indicates
that it is not of great importance(Kwon and others 2001).
During embryonic development, PTEN expression is thus mainly seen in the central nervous system.
In the adult brain, expressed is most important in neurons that function in control of motor activity,
behavioral control, emotions and memory storage. If PTEN expression during development is altered,
severe impairment in these functions would be expected. Different studies about PTEN mutations
are preformed, the results of these studies will be discussed here.
As mentioned before, the first studies involving PTEN were about its function as a tumor suppressor.
These studies showed that patients carrying an inactivating PTEN mutation have a prevalence to
develop different kinds of benign and malign tumors (Kwon and others 2001; van Diepen and
Eickholt 2008). Nevertheless, these studies also showed that the cancer prevalence can be coincided
by neurological defects such as macrocephaly, mental retardation, ataxia and seizures(Kwon and
others 2001; van Diepen and Eickholt 2008){{}}. The consequences of aberrant PTEN expression
depend on a couple of factors. In the case of an inactivating or a non-sense mutation, the
consequences differ between hetero- and homozygous mutations and between germ line and
conditional mutations. About activating PTEN mutations and neurological defects, little to no
information is available. The most sever condition is a homozygous Pten germ line knockout, which
leads to embryonic lethality(van Diepen and Eickholt 2008). Besides mutations, it is possible that
PTEN aberrations can be caused by copy number variations (CNV). In case of a CNV in PTEN, the
genome would contain an abnormal number of copies of the part of chromosome 10 where PTEN is
located. This means that there are less or extra copies of the PTEN gene in the genome, which will
lead to an abnormal amount of PTEN protein. About CNVs as a cause of PTEN aberrations, no
applicable literature is available. Therefore, only the different mutations that result in diminished
PTEN expression are discussed here.
In mice with a germ line Pten+/- mutation, moderate to severe seizures were seen during and after
development. One of the most obvious abnormalities in these animals is the pronounced
enlargement of the cerebellum, sometimes combined with hydrocephalus. Hydrocephalus can be
caused by the swelling of the cerebellum, which constricts the brainstem and the circulation of
cerebrospinal fluid(Kwon and others 2001). These mice were followed during development. At two
weeks of age, the neurons seemed to have a normal soma size and the mice seemed unaffected.
14
Four weeks after birth, an enormous cell-autonomous enlargement of the neuronal soma had
occurred. At the age of eight weeks, progressive atrophy in the Purkinje cells was first observed. The
atrophy of the Purkinje cells seems to be a secondary response to impaired Pten signaling in the
granule cells, which were earlier mentioned as being the neurons with the most extensive Pten
expression. (Kwon and others 2001)
Besides the studies about the consequences of heterozygous Pten germ line deletion, studies after
the effect of hetero- and homozygous conditional Pten knockouts were performed. Conditional
deletion conform the cre-lox method was performed, to achieve Pten deletion only at the desired
time and place(van Diepen and Eickholt 2008). This is necessary to prevent embryonic lethality and
to obtain more information about the role of Pten in certain processes in neuronal development. The
results of these studies are described below.
The heterozygous conditional Pten knockout mice appeared normal and exhibited no anatomical
abnormalities. However, protein homogenates and crude synaptosomal fractions of heterozygous
Pten knockouts showed that the levels of the NMDA receptor subunit NR2A were significantly
decreased. This indicates that heterozygous conditional Pten knockouts are not completely
asymptomatic, but that the knockout affects the expression of synaptic proteins. Further studies are
required to identify if this interaction is direct or indirect, which domains are involved in this
interaction and if this heterozygous Pten knockout influences other synaptic proteins(Ventruti and
others 2011).
Homozygous conditional Pten knockouts are far more extensively studied. The influence of
conditional homozygous Pten knockouts in different areas and at different stages of development
have been studied. Some important findings are discussed below.
In one of the conditional knockout studies, Pten has been deleted in neuronal stem cells on
embryonic day 9 or 10. The consequence was that these mice showed a lot of neurological defects,
among which macrocephaly, increased neuron size and number and defects in different regions of
the brain. The defects turned out to be that severe that the mice died soon after birth.(Groszer and
others 2001)
Four other knockout studies in mice embryos had less severe effects, but still caused premature
dead. In all studies, the mice showed macrocephaly and increased neuronal soma size(van Diepen
and Eickholt 2008).
In their study, Marino and colleages performed an additional experiment in which they knocked out
Pten in the neurons of the mid-hindbrain junction only. The mice showed defects in the cerebellum,
an increase in the number of neurons and loss of Purkinje cells. Before they died prematurely, these
mice suffered from ataxia and seizures and had impairments in their balance(Marino and others
2002). The group of Kwon knocked out Pten in the cerebellum and dentate gyrus. Since these brain
areas are among the areas that normally show the highest Pten expression, a clearly visible effect
would be expected. Indeed, defects in both areas, loss of Purkinje cells and degeneration of the
dentate gyrus were observed. During their life, these mice suffered from seizures and ataxia(Kwon
and others 2001). A third research performed by Fraser created a Pten knock-out in neurons and
astrocytes throughout the brain. Defects in the cerebellum and dentate gyrus were observed, as well
as increased size and proliferation of astrocytes. These mice also suffered from seizures and
ataxia(Fraser and others 2004). The aim of the fourth experiment, performed by Yue and colleagues,
is to investigate the influence of Pten loss in granule cells and Bergman glia in the cerebellum. The
consequences of this loss are impairment of the laminar organization in the cerebellum, defect is
15
formation and patterning of Bergman fibers and increased soma size of both Bergman glia and
neurons. These mice do not seem to have functional impairments during their live, nevertheless they
die prematurely(Yue and others 2005).
In the last study mentioned here, a homozygous Pten germ line knockout was induced in mice pups
four weeks after birth. Pten expression was blocked in the neurons of the cerebral cortex and the
hippocampus. The mice involved in this experiment exhibit macrocephaly, defects in the cerebral
cortex and hippocampus, hypertrophy of the neurons and an abnormal dendritic arbor (Kwon and
others 2006). Besides these anatomical abnormalities, the mice also displayed abnormal social
interactions and higher responses to sensory stimuli(Buxbaum and others 2007), features that are
typical for ASD.
These studies together pointed out a number of abnormities that occur in most types of neurons
when Pten expression is disturbed. Among these abnormalities are neuronal hypertrophy, impaired
neuronal migration with defect brain areas as a consequence, abnormal dendritic branching and
changes in behavior. What also can be concluded from the studies is that the seizure phenotype is
influenced by the timing of Pten loss and the brain areas affected(van Diepen and Eickholt 2008).
The defects caused by Pten deletion can be explained by its function in the PI3K/AKT pathway.
Normally, Pten has an inhibitory effect on the PI3K/AKT pathway by antagonizing PI3K. Pten
dephosphorylates PIP3 into PIP2, which results in less AKT phosphorylation. When little AKT activity
is present, growth, division and survival processes will be inhibited(Kwon and others 2001). In resting
cells, PIP3 levels normally are low and only increase upon growth factor activation(Stiles and others
2004),(Keniry and Parsons 2008). But when Pten is deleted, the growth pathway is no longer
inhibited and unrestrained cell growth and division can take place. This explains why neurons lacking
Pten have enlarged somas and are often present in higher numbers. (Kwon and others 2001) The
enlargement of the cerebellum relatively to other brain areas can also be explained by this account.
Since Pten expression is clearly more abundant in the cerebellum then in most of the other brain
areas, the impact of Pten loss will be relatively large. The inhibition on the PI3K/AKT pathway is lost,
which causes an enormous increase of growth stimulation, causing the swelling of the cerebellum.
Probably the observed macrocephaly is caused by a similar mechanism, although the exact nature of
macrocephaly remains difficult to establish(Bourgeron 2009).
The exact mechanism by which Pten knockout causes impaired neuronal migration has yet to be
unraveled. Nevertheless, a recent study found some clues that might help to better understand the
mechanism by which neuronal migration is regulated(Ventruti and others 2011). The aim of this
study was to better understand the function of Reelin, a growth factor that induces the PI3K/AKT
pathway by activating the RTK. Reelin has an important function in migration and dendrite
outgrowth. It was already known that insufficient Reelin expression could result in a reduced number
of dendritic spines. In the heterozygous Reelin knockout mice, altered expression of different
proteins was observed, among which Pten. If Reelin was absent, the amount of Pten in the
postsynaptic density decreased, which suggests that Reelin can in some way influence Pten
expression(Ventruti and others 2011). The other way round, it is possible that Pten influences Reelin
activity as well. In that case, a Pten knockout probably will result in down regulation of Reelin. Since
neuronal migration as well as dendritic outgrowth are impaired when Reelin is absent, this could
explain why this phenotype is seen in Pten knockout mice. But before this speculation can be
accepted as a prove for these symptoms, a large amount of research has to be performed.
16
It is hard to explain the observed changes in behavior just by mutations or changed molecular and
cellular mechanisms. Behavior is influenced by many different factors, the genetic basis is just one of
them. In the case of PTEN, this mutation can cause changes in certain brain areas, which can in part
explain the observed abnormal behavior. As mentioned before, a brain structure that is often
changed in animals with a Pten mutation is the dentate gyrus(Kwon and others 2001; van Diepen and
Eickholt 2008). The dentate gyrus is a part of the hippocampus, which belongs to the limbic system.
The limbic system has a role in emotion, behavior and memory. It is thus likely that people with PTEN
mutations have difficulties with these functions. Indeed, PTEN mutations are associated with ASD, a
disorder characterized by having difficulties with social situations, emotions and behavior.
Treatment of patients with PTEN mutations
The consequences of PTEN mutations are quite severe, besides cancer prevalence some of the
patients also have neurological problems like ASD. This raises the question if it is possible to treat
these patients. At this moment, ASD is a disorder that is only in very seldom cases curable(O'Hare
2009). Instead, therapy can be a very good option to help children with disorders in the autism
spectrum. The aim of the therapy can be to learn the children social skills, to reduce their anxiety or
to help them with other problems they experience. This therapy is aimed to reduce the symptoms
rather than cure the cause of the problem: the PTEN mutation.
PTEN mutations are a problem, because they deregulates the PI3K/AKT pathway. To create a better
regulation of the pathway and to reduce the risk to develop cancer, it would be desirable to
administer a PI3K/AKT pathway inhibitor. A candidate inhibitor would be the protein rapamycin.
Rapamycin was originally developed as an antifungal agent. However, the drug turned out to have
immunosuppressive properties. Since then, it is used as an immunosuppressant to prevent rejection
after organ transplantations(Hu and others 2011). Some of the same studies showed that Rapamycin
can as well inhibit proliferation by the inhibition of the rapamycine-sensitive mTOR-raptor complex
(mTORC1)(Hu and others 2011; Zhou and others 2009). As mentioned before, mTORC1 is activated
by the PI3K/AKT pathway and functions as a major regulator of cell growth. A inactivating PTEN
mutation thus would enhance mTORC1, which is suggested to lead to abnormal synaptic
function(Bourgeron 2009). It has already been demonstrated that rapamycin is able to reduce the
number of dendritic branches and to block the effect of different PI3K/AKT pathway
intermediates(Jaworski and others 2005). Murine studies showed that rapamycin could control
seizures, prolong survival, reverse learning and memory deficits and improve social interaction
behavior(Zhou and others 2009). Rapamycin thus can be a promising agent to normalize the
PI3K/AKT pathway in patients with PTEN mutations. One of the advantages of using Rapamycin as a
mTOR inhibitor in cancer patients and people with ASD, is that it is already used as an
immunosuppressant medicine. This means that all the medical security tests are already performed,
which will considerably accelerate the process preceding the approval of Rapamycin as a possible
treatment for people with ASD.
Other mutations in PI3K/AKT pathway
It is proven that mutations in the PTEN gene can have the development of ASD as a consequence. If
PTEN is mutated, the PI3K/AKT pathway is no longer inhibited, which can lead to ASD. Since a whole
amount of other proteins are involved in the pathway, the question arose if the mutation of one of
these proteins can also have ASD as a consequence. First, a literature study was performed to draw
up an inventory of the studies that might already be performed to answer this question.
17
Of one of the proteins in the PI3K/AKT pathway, TSC2, is known that its mutation is associated with a
high prevalence of autism. Mutations in TSC, which stands for tuberous sclerosis complex, lead to the
equally named disorder tuberous sclerosis (TS). Patients with TS develop non-malignant tumors,
additional symptoms are ASD (in 25%-60% of the cases), cognitive impairment an epilepsy(Kelleher
and Bear 2008). In unaffected people, TSC1/2 inhibits the growth-stimulating mTORC1. When
TSC1/2 does not function correctly, mTOR is no longer inhibited and translation in neurons will be
enhanced(Kelleher and Bear 2008). The effect on the neurons lacking TSC1/2 will thus be similar to
that of neurons lacking PTEN expression, there in both situations mTOR inhibition is no longer
present.
A recent study showed the involvement of EIF4E mutations in the development of autism. EIF4E is
the component that limits the rate of eukaryotic translation initiation. Being a target downstream of
mTOR, EIF4E activity is very important in learning and memory through its role in controlling the
translation in the synaps. Increased levels of EIF4E can increase the activity in the systems that
regulate these processes, which leads to repetitive, preservative behavior. Chromosomal
translocations implicating the region containing EIF4E and heterozygous insertions in the EIF4E
promoter have been identified in patients with autism. This finding implicates that the EIF4E
mutations could be one of the many causes of autism(Neves-Pereira and others 2009).
Other studies found that in patients with ASD, levels of certain proteins differed from the levels in
matched controls. The main conclusions of one of these studies, were that levels of Bcl2, AKT and
BDNF were significantly reduced, while p53 expression increased. All these proteins are involved in
the PI3K/AKT pathway and thus have a function in maintaining the balance between growth and
apoptosis(Sheikh and others 2010). What this study did not show, is what the cause of these changes
expression levels could be. It is possible that these changes are caused by mutations in these genes,
but also a deregulation of the pathway caused by mutations in (other) regulations of the pathway
could be the underlying cause. To get more insight in this cause, further research has to be
performed.
What can be concluded from this information, is that a lot of research has to be done before the
mutations that can cause autism spectrum disorders are all discovered.
18
Practical Part
Introduction
As mentioned in the introduction of this thesis, relatively little is known about the causes of ASD. The
involvement of the PI3K/AKT pathway is established, but which of the genes in this pathway are
mutated is not yet known. It is known that some of the people with ASD have mutations in PTEN, but
for most of the other genes in the pathway, no data are available. To answer the question if, besides
PTEN, mutations in other important genes involved in the PI3K/AKT pathway are seen in people with
ASD, a database search is performed. The database used for this aim is the Autism Genome Resource
Exchange database (AGRE). The aim of this search was to observe if mutations in PTEN, AKT, PDK1
and the gene encoding phosphatidylinositol-3-kinase (PI3K) are present in individuals with ASD. Since
PI3K is not encoded by only one gene, the PIK3CA gene, which encodes the catalytic subunit of PI3K,
was observed. Besides these four genes, the gene PKD1 was examined as well, for reasons that will
be evaluated in the discussion. On average, about 15 CNVs can be found in the entire human
genome, which makes the change to find a CNV in a arbitrary gene very small. If CNVs in the genes
examined here are causal for ASD, CNVs would be present in multiple patients. CNVs in PTEN would
be expected, since it is already demonstrated that deletions in that gene can cause ASD. CNVs in the
other genes can have similar effects, since the four genes function in the same pathway. In PI3K, AKT
and PDK1, duplications have similar effects as deletions in PTEN and would therefore be expected.
Material and methods
The Autism Genome Resource Exchange database (AGRE) is consulted to obtain genetic information
from ASD patients. The database consists of the micro-array data of about 4000 people, obtained
from about 1000 patients and their families. To obtain data about the prevalence of CNVs in the four
genes of interest, first the USCS genome browser was used to detect the position of these genes in
the genome. Because PI3K protein is encoded by multiple genes, only the catalytic subunit encoded
by the PIK3CA gene was observed. The decision to look at this gene is based on the program String
9.0, which indicated that this subunit was the most important for the PI3K/AKT pathway. Based on
the position found in the genome browser, the AGRE database was searched for CNVs in and around
this area. The database of genomic variants (DGV) was used to control whether the CNVs found in
the database are structural variations that are also present in healthy people. For the patients with
CNVs that turned out not to be structural variants, the program AGRE Pedigree was used to consider
if the subject has family members with ASD. If so, the genome of these family members was checked
in AGRE to see if the same CNV is present in these relatives. The last step in obtaining reliable
information about the eventual involvement of the four genes in ASD, is to eliminate falls positive
and negative results. The AGRE database is based on an algorithm that entails a relatively large
amount of falls positive results, but very little falls negatives. The falls positives are eliminated with
Beadstudio, a program used to analyze the gene expression levels, and ,in this case, to define
whether or not the result is likely to be falls positive.
A similar database search was performed in the Autism Genome Project (AGP) database. The AGP
database is the world’s largest gene bank for autism, containing about 6000 genetic profiles of both
multiplex (at least two affected individuals) and simplex (one affected individual plus both parents)
autism families. This advantage of this database is its size, for the reason that it is more likely to find
causal connections and extend our knowledge about the complex genetic basis of ASD if more
19
profiles are available. After the gene name was entered in this database, a list of both subjects with
ASD and parent people carrying mutations in this gene appeared.
Results
PTEN
The PTEN gene is located on chromosome 10, between 89,613,175 and 89,716,382 base pairs. In the
AGRE database, initially only one CNV was found PTEN. This CNV was a deletion between 89.596.169
and 89.747.929, which indicates that the CNV is located in the promoter area of PTEN. The Database
of Genomic Variation (DGV) was used to consider if this mutation could be a structural variant. In the
PTEN gene, three duplications in this gene are known to be structural variants. Since the CNV in our
subject is deletion, this CNV is not a structural variant. The family history of this subject was traced
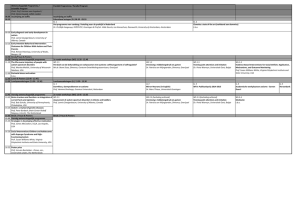
with the program AGRE Pedigree. As you can see in figure 4, the family of the subject with the
mutation did not carry the mutation. When this CNV was entered in Beadstudio, it turned out to be a
false positive call. Indications that led to this conclusion are the great distribution seen in this region
and the lack of clear deflection towards below zero. The AGRE database thus showed no CNVs in the
PTEN gene.
Legend
= affected male
= unaffected male
= affected female
= unaffected female
Figure 4. Pedigree of subject PTEN CNV
In the AGRE database, only one subject with a CNV in PTEN was found. The subject is indicated with a
red box around the subject number. Since this subject has two autistic siblings without the same CNV, it
is very unlikely that this CNV is the cause of ASD in this family. After the data were controlled with
Beadstudio, this CNV turned out to be a falls positive call.
In the AGP database, in four subjects with ASD CNVs in PTEN were found. Among these subjects were
two males and two females. In all four patients, the CNV observed was a deletion that included the
PTEN gene, none of the CNVs was located in the promoter area only. Since the AGP database
contains data of autism families, the parents with CNVs in PTEN were shown as well. The parents of
autistic children turned out to have CNVs in PTEN in a relatively high amount of cases. As many as
twelve parents have deletions in the PTEN gene.
AKT1
AKT1 can be found on chromosome 14, between 104,306,734 and 104,330,983 base pairs. The AGRE
database contains sixty-five individuals with CNVs that started in the 100kB before the beginning of
the AKT1 gene. Except for one deletion, all the CNVs were duplications. For AKT1, the DGV contains
six structural variants, among which five duplications and one deletion. Since there are so many CNVs
found in healthy controls, it is very unlikely that these CNVs in AKT1 are clinically relevant for ASD.
This region of chromosome 14 will probably be a polymorphic region, which could be an explanation
for the large amount of CNVs in this region is healthy people as well as subjects with ASD. Since
20
CNVs in AKT1 are concluded to be structural variants without clinical relevance, it was no longer
useful to further investigate the CNVs in this gene.
The AGP database contains no autistic people with CNVs in the AKT1 gene. In the populations of
parents, in contrast, three CNVs were found. Among these, two duplications and one deletion were
present.
PDK1
The location of PDK1 is chromosome 2, between base pair 173,129,025 and 173,172,108. For this
gene, one subject with a CNV was found in the AGRE database. This deletion was located the 100kB
before the start of the gene and thus might influence the transcriptional regulation. The DGV showed
that no structural variants for PDK1 are known. Information about the family of the subject was
obtained from AGRE Pedigree and can be found in figure 5. The subject that carries the CNV turned
out not to have a ASD and was the only family member with this CNV.
Legend
= affected male
= unaffected male
= affected female
= unaffected female
Figure 5. Pedigree of subject with PDK1 CNVs
One subject with a CNV in the PKD1 was present in the AGRE database, this is a non-syndromic male
that has a deletion in or nearby the promoter area of PDK1. The family member with the mutation is
indicated with a red box around the subject number. The subject is the non-syndromic father of two
autistic daughters. The fact that the daughters do not carry this deletion, makes it unlikely that this
deletion is the cause of ASD in this family.
In the AGP database, CNVs were present for neither subjects with ASD nor their parents.
PIK3CA
PIK3CA is the gene that encodes the catalytic subunit of phosphoinositide-3-kinase (PI3K). Mutations
in this gene result in dysfunction of PI3K. The gene is located on chromosome 3, between base pair
180,348,005 and 180,453,191. When the AGRE database was consulted to check if CNVs were
present in patients with ASD, the result turned out be negative. Neither the autistic individuals nor
their parents in this database show CNVs.
In the AGP database, no CNVs were found in cases with ASD either. However, one of the parents of
an autistic child showed a deletion in the PIK3CA gene and one other parent has a mutation in the
region just after PIK3CA. The database of genomic variants shows that five structural variants are
known for PIK3CA.
21
PKD1
PKD1 is located on chromosome 16, in the region between base pair 2.078.712 and 2.125.900.
When the location of PKD1 was checked in the AGRE database, 10 CNV were found in its promoter
area and in the gene itself. When these data were observed with Beadstudio, three of the CNVs came
true to be falls positive. For the other seven patients, the pedigree is displayed in figure 6. All seven
CNVs found here were located in the 100kB before the start of the gene, which indicates these CNVs
might influence the transcription regulation of PKD1. For all seven cases, the CNV is present in only
one family member. Only three of the subjects with the CNV were diagnosed with ASD. All three of
them have an autistic sibling that does not carry the same CNV.
B.
.
A.
Legend
= affected male
= unaffected male
= affected female
= unaffected female
C.
D.
E.
F.
C.
C.
.
G.
.
Figure 6. Pedigrees of subjects with PKD1 CNVs
In the AGRE database, seven subjects with a CNV in the PKD1 gene remained after falls positive results were
excluded. Subjects are indicated with a red box around the subject number. Subject A was the only subject with a
deletion in PDK1, B t/m G turned out to have duplications A The red asterisk indicates a sibling with a deletion close
to the deletion in the subject. The distance between the two CNVs however was 10kB, which is too much to
presume the two CNVs to be similar. A-C In these families, of the two autistic siblings carries the CNV in PKD1. If
this CNV would be the cause of ASD in these families, all autistic siblings would be likely to have that CNV.
Therefore it can be concluded that it is very unlikely that there is a causal relation between these CNVs and the
development of ASD. D-G In these families, the only affected individuals are non-autistic. Because the people that
carry the CNV are not affected with ASD, there is no causal relationship between these CNVs in PKD1 and ASD.
For PKD1, no search was performed in the AGP database.
22
Discussion
The probability that a CNV attributes in the development of ASD is the highest if all relatives with
ASD carry the same CNV, while this CNV is not present in the genome of unaffected family members.
Although this situation did not occur in our autism families, the following conclusions can be drawn
from the results from this search.
PTEN
The data from the AGP search indicate that deletions are seen in patients with ASD. However,
deletions in PTEN do occur as well in the non-autistic parents, which suggests that not all individuals
with deletions in PTEN have ASD. This finding can be interpreted in a few ways. First, this could mean
that PTEN deletion is not involved in the development of ASD, or that PTEN deletion can only cause
ASD in combination with other factors. Another explanation could be that the parents with PTEN
deletions are never diagnosed with ASD, but do show the symptoms. Based on the results of this
search, it is not possible to obtain a decisive explanation for this observation, nor to unequivocally
state that CNVs in PTEN are involved in the development of autism. An additional study in which the
prevalence of ASD will be observed in a larger cohort of patients with PTEN mutations, could learn us
more about the connection between PTEN mutations and ASD.
AKT1
For AKT, the CNVs found in the AGRE database were very likely to be structural variants. In the AGP
database, no copy number variations were found at all. If in a study population of this size of AGP no
CNVs are found at all, it is not very likely that CNVs in AKT1 are a common cause for autism spectrum
disorders. To make this statement more definite, additional studies could be performed in a study
population containing even more people with ASD.
PDK1
In the AGP database, no subjects with ASD nor their parents had CNVs in PDK1. In the AGRE
database, only one unaffected person has a deletion in PDK1. Together, these two databases indicate
that mutations in PDK1 are not commonly seen in people with ASD and thus unlikely to be a frequent
cause of the disorder.
PIK3CA
In both databases, no CNVs were found in individuals with ASD. In the AGP database, two parents of
autistic children did have CNVs. The CNVs found in the parents might either be structural variants, or
CNVs that are not involved in the development of ASD. These data indicate that CNVs in PIK3CA are
not likely to be a common cause of ASD.
PKD1
Only three of the seven subjects with CNVs in PKD1 are affected with ASD, in all three cases the
autistic siblings of these subjects do not show the same CNV. These findings suggest that CNVs in
PKD1 are not likely to be the cause of ASD in these families. Besides, when the database of genomic
variants was consulted for the right gene, it turned out that as many as nineteen structural variants,
both deletions and duplications, were known for PKD1. The gene PDK1 is thus very unlikely to be
involved in the development of ASD.
23
The four genes PTEN, AKT, PDK1 and PIK3CA are involved in PI3K/AKT pathway and are therefore
chosen for this database search. But what is the function of PKD1 and why is it involved in this
search? PKD1 is a gene that can be transcribed in different ways and has multiple biological functions
in health and disease. It is especially known for its crucial function in kidney development(Rozengurt
2011). This gene is included in the database search by accident. A typing error in the USCS genome
browser during the search for the position of PDK1, resulted in the position of PKD1. With the
position of PKD1, the search in AGRE was performed and the results section for AGRE was written. I
did not notice this mistake, until the results of the AGP database were obtained. When I compared
the data from the two databases, thirteen CNVs were present for PDK1 in AGRE, but none in AGP.
This difference was very illogical, therefore I started looking thoroughly for the cause of this
difference. The reason why these data are still included in this thesis, is because it did deliver
relevant information. Thanks to this search, we now know that PKD1 CNVs seem not to be involved
in the development of ASD. Besides, this gene was the one that was most extensively studied. That is
because in this gene seven CNVs were present, while (when PDK was inserted) no structural variant
of the gene seemed to be known. Because these seven people and their families were all controlled,
the results showed best the techniques and methods applied in this search.
When the typing error was discovered, the correct position for PDK was searched in AGRE for
mutations. Because the only CNV that resulted from the database was not relevant, since it was only
seen in one unaffected individual, Beadstudio was not consulted in this case.
Of the genes encoding for PI3K, only PIK3CA was observed. This is because the program String 9.0
indicated that this gene was the most important in the pathway. Another gene that is involved in the
PI3K pathway is PIK3CG. To create a more complete knowledge about the genetic basis of autism
spectrum disorders, further research with the aim to indentify if this gene is mutated in people with
ASD would be useful.
In the first paragraphs of the discussion, the conclusion sometimes is that studies in a larger
population can be performed. For now, AGP is known to be the most extensive autism database,
which might make this reference seem useless. The reason why this reference is made, is because
the AGP project consists of different phases, in each phase the database is extended. The filename of
the results used in this thesis indicate that the phase 1 database is used. This database contains only
1500 families, while the phase 2 version created in 2010 contains as many as 7500 families. The third
phase of the project just started and will even further extend the amount of data
(www.autismgenome.org).
In some of the pedigrees, it occurs that two unaffected parents do have affected children. Since ASD
is known to be highly inheritable, this is a quite remarkable observation. Nevertheless, there are
some things that can explain this notable event. First, it is possible that one of the parents does have
a mild form of ASD, but is never diagnosed. A second declaration could be a de novo mutation in the
child, which has ASD as a consequence. This statement can only be true if the CNV is seen in just one
child, because the change is very small the same mutation occurs twice. Since the genetic cause of
ASD is not unraveled, another possibility is that the combination of the genes of both parents led to
autism. In this case, more than one gene is necessary to cause ASD in one individual. After all, it is
suggested that besides genetic factors, ASD can be caused by environmental factors.
24
Conclusion
The aim of this thesis is to examine the PTEN regulated pathway in brain tissue and its role in the
development of autism spectrum disorders. The pathway that PTEN regulates turned out to be the
PI3K/AKT pathway, involved in cell division, growth and migration. The literature about the exact
composition of this pathway is adversary at some points. Besides, the fact that pathways in the cell
interact with a range of other pathways, means that the writer has to decide where to stop
describing the pathway. Nevertheless, according to the literature available at this moment, an
overview of the principles of the PI3K/AKT pathway is composed.
It is now generally accepted that aberrant expression of PTEN can play a role in the development of
ASD. Since the genes AKT, PDK1 and PIK3CA function in the same pathway as PTEN, the question
arose if impairments in the expression of these genes could lead to ASD as well. A database study
demonstrated that for all three genes, no CNVs were present in the genome of patients with ASD.
For PTEN, CNVs were observed in some cases with ASD. Since this search was performed in a
relatively large population, it is unlikely that CNVs in AKT, PDK1 or PIK3CA are common causes of
ASD. The observation that other important players in the PI3K/AKT pathway are not involved in the
development ASD, suggests that PTEN is the only gene in that pathway for which this causal
connection is present. Nevertheless, to test this hypothesis, a more extensive study, in which all
genes involved in the pathway are included, has to be performed.
The exact mechanism by which CNVs in PTEN can lead to the development of ASD are not clear, but
observations in Pten knockout mice supplied some cues. Knockout of Pten leads to changes in the
size of neurons and in their connections with other neurons. These changes are most severe in the
cerebellum and the dentate gyrus, part of the hippocampus. The most obvious feature of patients
with ASD is their deviating behavior. The dentate gyrus plays a major role in the limbic system, which
is involved in emotion, empathy, behavior and memory. This are just the areas that autistic people
have problems with. Nevertheless, these observations are just the onset of the process of unraveling
the mechanisms by which ASD is caused. Further research is necessary to better understand the
cellular and molecular mechanisms behind ASD.
The main question of this thesis is how PTEN mutations can influence the PI3K/AKT pathway and
what the association between these mutations and ASD is. In the normal situation, PTEN antagonizes
PI3K,thereby inhibiting the growth-stimulation PI3K/AKT pathway. Deletions in PTEN impair this
inhibition, which causes problems like extensive growth and division. When this happens during
brain development, overgrowth of certain brain areas and incorrect connections between neurons
can arise, which can cause a spectrum of developmental disorders known as ASD. To further enrich
our knowledge about the precise impairments in brain development due to PTEN aberration, further
research has to be performed.
Acknowledgements
I would like to thank Peter Burbach for being my supervisor and supporting me by writing this thesis.
Besides, I would like to thank Emma van Daalen, Bert van der Zwaag, Jacob Vorstman and Robert van
Jaarsveld for showing me what their jobs contain and helping me with the practical part of this
thesis.
25
References
Baltussen M, Clijsen A, Leenders Y. 2003. Leerlingen met autisme in de klas. een praktische gids voor
leerkrachten en intern begeleiders. 1st ed. Meppel: Drukkerij Giethoorn ten Brink.
Bourgeron T. 2009. A synaptic trek to autism. Curr Opin Neurobiol 19(2):231-4.
Butler MG, Dasouki MJ, Zhou XP, Talebizadeh Z, Brown M, Takahashi TN, Miles JH, Wang CH, Stratton
R, Pilarski R, et al. 2005. Subset of individuals with autism spectrum disorders and extreme
macrocephaly associated with germline PTEN tumour suppressor gene mutations. J Med Genet
42(4):318-21.
Buxbaum JD, Cai G, Chaste P, Nygren G, Goldsmith J, Reichert J, Anckarsater H, Rastam M, Smith CJ,
Silverman JM, et al. 2007. Mutation screening of the PTEN gene in patients with autism spectrum
disorders and macrocephaly. Am J Med Genet B Neuropsychiatr Genet 144B(4):484-91.
Carracedo A and Pandolfi PP. 2008. The PTEN-PI3K pathway: Of feedbacks and cross-talks. Oncogene
27(41):5527-41.
Das S, Dixon JE, Cho W. 2003. Membrane-binding and activation mechanism of PTEN. Proc Natl Acad
Sci U S A 100(13):7491-6.
Fraser MM, Zhu X, Kwon CH, Uhlmann EJ, Gutmann DH, Baker SJ. 2004. Pten loss causes hypertrophy
and increased proliferation of astrocytes in vivo. Cancer Res 64(21):7773-9.
Freeman DJ, Li AG, Wei G, Li HH, Kertesz N, Lesche R, Whale AD, Martinez-Diaz H, Rozengurt N,
Cardiff RD, et al. 2003. PTEN tumor suppressor regulates p53 protein levels and activity through
phosphatase-dependent and -independent mechanisms. Cancer Cell 3(2):117-30.
Fukunaga K and Kawano T. 2003. Akt is a molecular target for signal transduction therapy in brain
ischemic insult. J Pharmacol Sci 92(4):317-27.
Gilman SR, Iossifov I, Levy D, Ronemus M, Wigler M, Vitkup D. 2011. Rare de novo variants associated
with autism implicate a large functional network of genes involved in formation and function of
synapses. Neuron 70(5):898-907.
Groszer M, Erickson R, Scripture-Adams DD, Lesche R, Trumpp A, Zack JA, Kornblum HI, Liu X, Wu H.
2001. Negative regulation of neural stem/progenitor cell proliferation by the pten tumor
suppressor gene in vivo. Science 294(5549):2186-9.
Hu M, Ekshyyan O, Herman Ferdinandez L, Rong X, Caldito G, Nathan CO. 2011. Efficacy and
comparative effectiveness of sirolimus as an anticancer drug. Laryngoscope 121(5):978-82.
Jaworski J, Spangler S, Seeburg DP, Hoogenraad CC, Sheng M. 2005. Control of dendritic arborization
by the phosphoinositide-3'-kinase-akt-mammalian target of rapamycin pathway. J Neurosci
25(49):11300-12.
26
Kelleher RJ,3rd and Bear MF. 2008. The autistic neuron: Troubled translation? Cell 135(3):401-6.
Keniry M and Parsons R. 2008. The role of PTEN signaling perturbations in cancer and in targeted
therapy. Oncogene 27(41):5477-85.
Kwon CH, Luikart BW, Powell CM, Zhou J, Matheny SA, Zhang W, Li Y, Baker SJ, Parada LF. 2006. Pten
regulates neuronal arborization and social interaction in mice. Neuron 50(3):377-88.
Kwon CH, Zhu X, Zhang J, Knoop LL, Tharp R, Smeyne RJ, Eberhart CG, Burger PC, Baker SJ. 2001. Pten
regulates neuronal soma size: A mouse model of lhermitte-duclos disease. Nat Genet 29(4):40411.
Lee JO, Yang H, Georgescu MM, Di Cristofano A, Maehama T, Shi Y, Dixon JE, Pandolfi P, Pavletich NP.
1999. Crystal structure of the PTEN tumor suppressor: Implications for its phosphoinositide
phosphatase activity and membrane association. Cell 99(3):323-34.
Levitt P and Campbell DB. 2009. The genetic and neurobiologic compass points toward common
signaling dysfunctions in autism spectrum disorders. J Clin Invest 119(4):747-54.
Marino S, Krimpenfort P, Leung C, van der Korput HA, Trapman J, Camenisch I, Berns A, Brandner S.
2002. PTEN is essential for cell migration but not for fate determination and tumourigenesis in
the cerebellum. Development 129(14):3513-22.
Neves-Pereira M, Muller B, Massie D, Williams JH, O'Brien PC, Hughes A, Shen SB, Clair DS,
Miedzybrodzka Z. 2009. Deregulation of EIF4E: A novel mechanism for autism. J Med Genet
46(11):759-65.
O'Hare A. 2009. Autism spectrum disorder: Diagnosis and management. Arch Dis Child Educ Pract Ed
94(6):161-8.
Pardo CA and Eberhart CG. 2007. The neurobiology of autism. Brain Pathol 17(4):434-47.
Pinto D, Pagnamenta AT, Klei L, Anney R, Merico D, Regan R, Conroy J, Magalhaes TR, Correia C,
Abrahams BS, et al. 2010. Functional impact of global rare copy number variation in autism
spectrum disorders. Nature 466(7304):368-72.
Planchon SM, Waite KA, Eng C. 2008. The nuclear affairs of PTEN. J Cell Sci 121(Pt 3):249-53.
Purves D, Augustine GJ, Fitzpatrick D, Hall WC, LaMantia A, McNamara JO, White LE. 2008.
Neuroscience. 4th ed. Sunderland, Massachusetts U.S.A.: Sinauer.
Qu Q and Shi Y. 2009. Neural stem cells in the developing and adult brains. J Cell Physiol 221(1):5-9.
Rodgers EE and Theibert AB. 2002. Functions of PI 3-kinase in development of the nervous system.
Int J Dev Neurosci 20(3-5):187-97.
27
Rozengurt E. 2011. Protein kinase D signaling: Multiple biological functions in health and disease.
Physiology (Bethesda) 26(1):23-33.
Schaaf CP and Zoghbi HY. 2011. Solving the autism puzzle a few pieces at a time. Neuron 70(5):806-8.
Sheikh AM, Malik M, Wen G, Chauhan A, Chauhan V, Gong CX, Liu F, Brown WT, Li X. 2010. BDNF-aktBcl2 antiapoptotic signaling pathway is compromised in the brain of autistic subjects. J Neurosci
Res 88(12):2641-7.
Stiles B, Groszer M, Wang S, Jiao J, Wu H. 2004. PTENless means more. Dev Biol 273(2):175-84.
Stiles BL. 2009. Phosphatase and tensin homologue deleted on chromosome 10: Extending its
PTENtacles. Int J Biochem Cell Biol 41(4):757-61.
Tamguney T and Stokoe D. 2007. New insights into PTEN. J Cell Sci 120(Pt 23):4071-9.
Toro R, Konyukh M, Delorme R, Leblond C, Chaste P, Fauchereau F, Coleman M, Leboyer M, Gillberg
C, Bourgeron T. 2010. Key role for gene dosage and synaptic homeostasis in autism spectrum
disorders. Trends Genet 26(8):363-72.
van Diepen MT and Eickholt BJ. 2008. Function of PTEN during the formation and maintenance of
neuronal circuits in the brain. Dev Neurosci 30(1-3):59-64.
Ventruti A, Kazdoba TM, Niu S, D'Arcangelo G. 2011. Reelin deficiency causes specific defects in the
molecular composition of the synapses in the adult brain. Neuroscience .
Vivanco I and Sawyers CL. 2002. The phosphatidylinositol 3-kinase AKT pathway in human cancer.
Nat Rev Cancer 2(7):489-501.
Wu X, Hepner K, Castelino-Prabhu S, Do D, Kaye MB, Yuan XJ, Wood J, Ross C, Sawyers CL, Whang YE.
2000. Evidence for regulation of the PTEN tumor suppressor by a membrane-localized multi-PDZ
domain containing scaffold protein MAGI-2. Proc Natl Acad Sci U S A 97(8):4233-8.
Yue Q, Groszer M, Gil JS, Berk AJ, Messing A, Wu H, Liu X. 2005. PTEN deletion in bergmann glia leads
to premature differentiation and affects laminar organization. Development 132(14):3281-91.
Zhou J, Blundell J, Ogawa S, Kwon CH, Zhang W, Sinton C, Powell CM, Parada LF. 2009.
Pharmacological inhibition of mTORC1 suppresses anatomical, cellular, and behavioral
abnormalities in neural-specific pten knock-out mice. J Neurosci 29(6):1773-83.
28
Supplementary material
Supplement 1: Onderzoek spelgedrag bij een jongentje van 3;9 jaar
Het eerste onderzoek dat werd uitgevoerd was een onderzoek naar het speelgedrag van het kind.
Aan het spelgedrag van een kind kunnen een aantal dingen worden afgeleid over zijn (sociale)
ontwikkeling. Tijdens dit onderzoek werden er een aantal spelletjes gedaan, waarbij onder andere
vaardigheden als het maken van oogcontact, sociaal spelen, vragen stellen, een gesprek voeren,
fantasie en eventueel stereotype gedrag worden getest. Wat zegt speelgedrag precies? Is dit een
goede manier om verschillende vaardigheden te meten?
Dit onderzoek werd uitgevoerd in een spiegelkamer, waardoor twee andere psychiaters en ik mee
konden kijken zonder het kind te beïnvloeden. Toen de ouders met het kind binnenkwamen, begon
het jongentje direct met een speelgoedtelefoon te spelen. Emma van Daalen, de kinderpsychiater,
nam samen met een psychiater in opleiding eerst een gesprekje met de ouders af over de
voorgeschiedenis van het kind.
Vervolgens mochten de ouders aan de rand van de kamer gaan zitten en zich zo normaal mogelijk
gedragen zonder het kind actief te beïnvloeden. Emma begon met het speelonderzoek. Nadat ze de
speeltjes waarmee het jongentje bezig was had weggelegd, probeerde ze verschillende spelletjes te
doen om zijn verschillende vaardigheden te testen.
Op het eerste gezicht zag dit jongentje er normaal uit. Toen hij alleen aan het spelen was terwijl
Emma met de ouders praatte, zag zijn spelgedrag er ook uit als dat van een normaal ontwikkeld kind.
Tijdens de spelletjes die Emma met hem probeerde te doen vielen er wel een aantal dingen op.
Een van de spelletjes bestond eruit dat het jongentje een beperkt aantal blokjes kreeg die hij op een
bordje met pinnetjes moest bevestigen. Emma zei van tevoren dat hij om meer blokjes mocht vragen
als het er niet genoeg waren. Dit deed zij om te kijken in hoeverre het kind vragen stelt aan anderen.
Bij dit spel leek het gedrag van het jongentje vrij normaal, hoewel hij repetitief het zinnetje ‘Die moet
daar’ gebruikte. Toen de blokjes op waren vroeg hij niet om nieuwe blokjes. Toen Emma aan hem
vroeg of hij meer blokjes nodig had gaf hij wel goed antwoord, hoewel hij Emma daarbij niet
aankeek.
Een ander spelletje om te kijken of het jongentje een vraag kon stellen is het bellen blazen. Dit
jongentje vond de bellen heel leuk, hij probeerde ze te vangen en kapot te maken. Toen de bellen op
waren, was het de bedoeling dat hij vroeg of Emma er meer wilde blazen. Dit deed hij niet, hij ging
wel naar Emma toe en maakte een ‘bellen-pak-gebaar’. Toen Emma aan hem vroeg of ze meer bellen
moest blazen, zei hij wel ja. Uit zichzelf vragen stellen doet hij dus niet.
Bij een ander spelletje kreeg het jongentje een aantal meubeltjes en poppetjes waarmee hij mocht
gaan spelen. Het doel van dit spelletje is om te kijken in hoeverre het kind sociaal spelgedrag
vertoont. In eerste instantie leek hij dit op een normale manier te doen. Hij liet het poppetje tegen
een bal schoppen en riep ‘Goal’. Wel was toen al duidelijk dat zijn taalgebruik vrij minimaal en
onduidelijk was voor een kind van zijn leeftijd. In eerste instantie liet hij Emma met een van de
poppetjes spelen, hij reageerde echter niet op haar spel. Verderop in het spel viel op dat het
jongentje niet reageerde op Emma’s vragen en Emma negeerde, de speeltjes steeds wat meer zijn
eigen kant op verplaatste en de poppetjes voorzichtig van Emma afpakte en ergens anders neerzette.
Hij speelde zijn eigen spel, waarbij hij niet praatte maar alleen geluidjes maakte. Dit spelgedrag wijkt
sterk af van wat je zou verwachten bij een kind van zijn leeftijd.
29
Bij de eerste spelletjes was het jongentje relatief geconcentreerd en bleef hij goed op zijn stoeltje
zitten. Later tijdens het onderzoek begon hij meer weg te lopen. Als er iets nieuws werd neergezet
(waarbij geluid werd gemaakt) kwam hij echter wel weer kijken wat er gebeurde. Daarbij zei hij
verbaasd ‘Oohh’, hoewel dit eerder aangeleerd dan oprecht klonk.
Om te kijken in hoeverre het jongetje zijn fantasie kan gebruiken heeft Emma een paar spelletjes
geprobeerd. Bij het eerste spelletje was het de bedoeling dat het jongentje zijn tanden zou poetsen
met een denkbeeldige tandenborstel, tandpasta en kraan. Toen dit niet lukte probeerde Emma hem
denkbeeldig zijn handen te laten wassen. Om hem op weg te helpen zette ze een zeeppompje en
handdoekje neer, toch kreeg ze het jongentje niet zo ver om dit te gaan doen.
Een alternatief spel was het vieren van de verjaardag van de baby (pop). Eerst liet ze het jongentje
een taartje van klei versieren met kaarsjes. Ze stak denkbeeldig de kaarsjes aan. Toen Emma met
hem wilde zingen voor de pop, liep het jongetje weg naar een hoek van de kamer en ging daar een
ineengedoken liggen. Dit gedrag was erg opvallend. Na het zingen kreeg Emma hem wel weer op zijn
plaats om de taart te snijden. Toen Emma vroeg of er nog iemand taart zou willen, voerde hij uit
zichzelf de pop (maar niet Emma). De opdracht om het zogenaamd geknoeide drinken op te ruimen
met een servetje begreep hij echter niet goed, hij ruimde het servet op. Vervolgens vroeg Emma hem
de baby naar bed te brengen. Hieraan vooraf haalde hij eerst de restjes ‘taart’ uit de mond van de
pop en zocht toen een goed plekje om haar neer te leggen, wat erg zorgzaam was.
Toen het jongentje niet direct naar de tafel kwam nadat hij daarvan weg was gelopen, blies Emma
een ballon op. Hiermee wilde ze testen of hij kon aangeven hoe groot de ballon moest worden. Dit
kon het jongentje niet, hij zei alleen ‘groot’.
Samen een boekje lezen was een opdracht die niet zo goed ging. Emma begon en het jongentje
moest het verhaal afmaken. Zijn aandacht dwaalde heel snel af en hij liep weg. Als Emma
nadrukkelijk iets vroeg, gaf hij soms antwoord met één woord (als Emma bijvoorbeeld vroeg wat hij
zag, antwoordde hij ‘Leeuw’). De moeder van het jongentje gaf aan dat hij boekjes lezen nooit
interessant vindt.
Aan het einde van het onderzoek had Emma een hondje dat ze met een afstandsbediening kon laten
bewegen. Het jongentje had niet echt veel interesse in het hondje. Toen Emma probeerde zijn
aandacht te trekken door hem in zijn zij te prikken, wilde het jongetje pakkertje doen. Dit was de
enige keer dat hij echt oprecht leek te lachen en dat ze zogenaamd gedeeld plezier hadden.
Tussen de verschillende spelletjes door probeerde Emma een paar keer een gesprekje met het
jongentje te beginnen. De eerste poging was een gesprekje over een fiets (heb jij een fiets? Welke
kleur is die?). Hierop kreeg ze geen reactie. Een tweede poging was een gesprekje over huisdieren.
Emma vroeg of het jongentje een poes had thuis. Daarop zei hij uiteindelijk ja. Toen Emma zei dat ze
ook een poes had thuis, reageerde het jongentje daar niet op. Op Emma’s vraag of hij thuis ook een
hond had (naar aanleiding van het knuffelhondje waarmee ze probeerde te spelen) gaf het jongentje
geen duidelijk antwoord. De moeder zei dat ze thuis geen poes en geen hond hadden (alleen een
poezenknuffel). Het jongentje leek helemaal geen interesse in Emma te tonen.
Wat verder opviel was dat het jongentje een duidelijke achterstand in de taalontwikkeling had. Hij
sprak weinig en articuleerde niet goed. Zijn niveau lag duidelijk onder het verwachtte niveau van een
kind dat bijna naar school zal gaan. Het jongentje is al begonnen met logopedie. Uit de tot nu toe
uitgevoerde tests kwam nog niet veel informatie, behalve dat zijn woordbegrip net onder gemiddeld
lag. Aan de andere test had hij niet goed meegedaan. Logopedie wordt voortgezet.
Nadat Emma aan de ouders gevraagd had of het jongentje zich gedroeg zoals voor hem normaal is en
verteld had hoe het traject verder gaat verlopen, werd het onderzoek nabesproken. Emma en de
30
mensen achter de spiegel (de andere psychiaters en ik) bespraken of ze hetzelfde gezien hadden en
wat dit betekent voor de diagnose.
Vervolgens vulde Emma een classificatieformulier in dat aan de criteria van de DSM voldoet. Op dit
formulier worden alle verschillende type gedrag die getest zijn genoemd. Daarbij staan verschillende
stellingen over dit gedrag genoemd. Het is de bedoeling dat de stelling die het meest overeenkomt
met de gedragingen van het kind wordt aangevinkt. Bij elke stelling hoort tevens een puntenaantal.
Uiteindelijk zal het totale puntenaantal een diagnose opleveren. Deze dient dan te worden
vergeleken met de klinische diagnose (de diagnose van de observatoren). In dit geval kwamen beide
diagnoses overeen en heeft dit kind de diagnose autisme gekregen.
Supplement 2: Verslag klinisch interview van een 6 jarig jongentje (Rida)
Uiterlijk
Op het eerste gezicht ziet het jongentje er normaal uit, zijn lichaamsbouw en gelaat zijn niet
afwijkend. Er zijn geen duidelijke dysmorfieën zichtbaar. De leeftijdsschatting komt ongeveer
overeen met zijn daadwerkelijke leeftijd. Hij wil geen spijkerbroek en schoenen meer aan en draagt
daarom een joggingbroek en sandalen. Aan zijn handen heeft hij handschoentjes tegen het bijten. De
verzorging lijkt goed te zijn.
Sociale functies, contact en communicatie
Contact met de onderzoeker
Af en toe maakt hij oogcontact met de onderzoeker. Hij kijkt dan nadrukkelijk in de ogen. Gebaren
zijn niet of nauwelijks te zien. De mimiek is duidelijk minder dan je van een kind van deze leeftijd zou
verwachten. Hij lacht soms en als hij bang is, is dit duidelijk zichtbaar. Verder is het lastig emoties van
zijn gezicht af te lezen. Van gedeeld plezier was tijdens het interview geen sprake. Omdat hij niet kan
praten, was er geen over- en weer gesprek. Wederkerigheid is niet waargenomen.
Vermogen tot inschatten van gevoelens van anderen (empathie)
Het feit dat dit jongentje niet praat, maakt het lastiger in te schatten of hij empathie vertoont. Zijn
taalbegrip is niet zodanig dat hij emoties kan opmaken uit gesproken taal. Het lijkt er niet op dat hij
veel inzicht heeft in de gevoelens van anderen.
Cognitieve functies
Het bewustzijnsniveau is verlaagd ten opzichte van leeftijdsgenootjes. Het jongentje lijkt zich
verminderd bewust van zichzelf en zijn omgeving. De oriëntatie is verminderd. Aandacht en
concentratie zijn beperkt. Hij kan zich kort op een spelletje concentreren, maar gaat als snel weer
rondjes lopen. Tot uitvoerende functies als planning en cognitieve flexibiliteit is hij niet in staat.
Spraak is niet aanwezig, simpele, korte opdrachten begrijpt hij wel. Door het gebrek aan taal is het
geheugen lastig te beoordelen. Wel reageert hij anders op nieuwe personen dan op al bekende
personen. Zijn waarneming lijkt intact, hij observeert objecten en personen. Zijn intelligentie is
beneden gemiddeld, complexe zinnen begrijpt hij niet, hij moet korte en duidelijke opdrachten
krijgen.
Affectieve functies/gevoelsleven
Zijn stemming is op dit moment vrolijk. Hij is nieuwsgierig en rustig en maakt af en toe een tevreden
31
klinkend geluid. Hij lijkt niet depressief of euforisch te zijn. Van angst en vermijdingsgedrag was
sprake hij aangeraakt werd en stil moest liggen om zijn bloeddruk te meten. Op de aanraking bij het
vasthouden van zijn hand reageerde hij rustig. Dwanghandelingen zijn duidelijk aanwezig. Hij krabt
zichzelf en bijt op zijn handen. Ook loopt hij veel rondjes en blijft hij rondjes draaien op de
bureaustoel.
Motoriek
In zijn grove motoriek lijkt hij achter te lopen. Wel kan hij zelfstandig lopen. Zijn fijne motoriek is
onderontwikkeld. Hij slaagt er niet in de blokjes in de passende gaatjes te stoppen. Dit kan ook deels
desinteresse zijn, omdat hij al na twee keer proberen zijn aandacht op iets anders richt. Tics zijn
aanwezig. Hij bijt, vooral als hij angstig is, veel op zijn handen. Het rondjeslopen is mogelijk een
motorische stereotypie. Psychomotorische ontwikkeling is wel aanwezig, maar ook hierin loopt hij
achter.
Spel
Spel lijkt in zijn algemeen niet of nauwelijks aanwezig te zijn. Hij heeft even met het spelletjes
gespeeld waarbij hij blokjes in het juiste gaatje moest stoppen. Dit was echter maar erg kort. Het
grootste deel van de tijd liep hij rond, of zat hij op een stoel rondjes te draaien. Ook keek hij soms
een tijdje naar objecten of personen in de kamer.
Gedragsregulatie
Op het moment dat hij in de kamer was heeft hij geen agressief gedrag vertoont. Toen zijn bloeddruk
werd gemeten probeerde hij los te komen door zich vrij te worstelen. Dit was echter een
paniekreactie.
Supplement 3: Verslag intake/spelonderzoek van een 4 jarig jongentje (Philip)
Uiterlijk
In eerste instantie leek dit jongentje geen opvallende uiterlijke kenmerken te hebben. Na beter
kijken viel op dat hij wat vreemd uit zijn ogen keek, zijn ogen staan relatief dicht bij elkaar. Ook had
hij wat trekjes met zijn mond. Het kind leek groot voor zijn leeftijd, hij zou ongeveer een jaar ouder
geschat kunnen worden dan zijn daadwerkelijke leeftijd. Zijn lichaamsbouw was normaal en hij
maakte een verzorgde indruk.
Sociale functies, contact en communicatie
Contact met de onderzoeker
Hij keek de onderzoeker een aantal keer in de ogen. Het was niet helemaal duidelijk of hij haar
daadwerkelijk elke keer bewust aankeek of dat hij een deel van de tijd toevallig die kant op keek.
Oogcontact werd niet actief vermeden. Gebaren maakte hij minimaal, maar hij wees wel één keer
spontaan iets aan. Zijn mimiek was niet erg goed. Als hij blij was of lachte was dit af te lezen. Het
grootste deel van de tijd was zijn gezicht echter uitdrukkingloos. Hij probeerde wel plezier te delen
door richting zijn ouders te kijken, maar slaagde hier niet echt in. Een gesprek voeren deed hij niet,
hij zei enkel af en toe een los woord. Er was geen sprake van wederkerigheid.
Vermogen tot inschatten van gevoelens van anderen (empathie)
32
Tijdens dit onderzoek heeft hij geen empathie getoond.
Cognitieve functies
Het bewustzijnsniveau is lager dan te verwachten bij een kind van vier. Hij lijkt zich weinig bewust te
zijn van wat er zich precies in zijn omgeving afspeelt, hij reageert niet adequaat op dingen in zijn
omgeving. Zijn oriëntatie lijkt daardoor ook minder te zijn. Het is goed mogelijk zijn aandacht te
trekken met iets wat hij leuk vindt. Zijn concentratie is laag, hij maakt snel een afwezige indruk. Tot
uitvoerende functies als plannen en cognitieve flexibiliteit is hij niet in staat. Taal en spraak is
minimaal. Als hij met zijn naam wordt aangesproken en concrete opdrachten krijgt, is hij in staat die
uit te voeren. Hij spreekt enkele woorden, zoals ja, nee en hoera. Dit is echter aanzienlijk minder dan
bij een kind van vier verwacht wordt. Zijn geheugen is zodanig dat hij in elk geval bepaalde zaken kan
onthouden. Zo wist hij na 20 minuten nog dat de bellenblaas op de kast lag, wat op te maken uit het
feit dat hij daarnaar wees. Zijn waarneming is waarschijnlijk intact. Hij kan onderscheid maken tussen
verschillende personen en objecten. In hoeverre hij kan denken is lastig te beoordelen. Wel is
duidelijk dat zijn intelligentie ver beneden gemiddeld ligt.
Affectieve functies/gevoelsleven
Zijn stemming leek vrolijk te zijn. Het is een heel rustig jongentje. Soms was hij duidelijk vrolijk,
bijvoorbeeld als het kiekeboe-spelletje met hem werd gespeeld of als hij probeerde zijn vaders bril af
te pakken. Op het moment dat hij gewogen moest worden en zijn hoofdomtrek werd gemeten, was
hij erg angstig. Hij protesteerde en probeerde zich los te krijgen. Waarschijnlijk heeft hij geen last van
dwanghandelingen, dit was echter niet helemaal goed te bepalen.
Motoriek
In zijn grove motoriek loopt dit jongentje duidelijk achter. Hij kan staan, maar staat niet erg stabiel.
Lopen kan hij alleen aan de hand, nog niet zelfstandig. Het ziet er wat ongecontroleerd uit. De fijne
motoriek was ook onderontwikkeld. Hij probeerde een kaarsje in de taart van klei te steken, maar dit
lukte hem niet. Een kind van vier zou dit wel moeten kunnen. Er is heel duidelijk sprake van
stereotype motoriek of tics. Als er niets van hem gevraagd wordt, gaat hij over in stereotype
bewegingen. Hij beweegt zijn hoofd heen en weer en schudt met een speeltje en maakt
knijpbewegingen met zijn handen. Dit heeft ook iets weg van fladderen met de armen. Hiermee
houdt hij niet op, totdat hij actief wordt gestopt. De psychomotoriek is onderontwikkeld, hij kan niet
gecontroleerd geplande bewegingen maken.
Spel
Spontaal spel kwam niet voor, als hij zelfstandig mocht spelen was hij alleen bezig met stereotype
bewegingen. Het spel tijdens het onderzoek was vrij minimaal. Fantasiespel kwam niet voor en ook
functioneel spel was niet aanwezig. Wel vond hij een simpel spelletje als kiekeboe erg leuk. Het
spelen met de onderzoeker en de aandacht die hij daarbij kreeg vond hij leuk. Hij probeerde nonverbaal voor elkaar te krijgen dat de onderzoeker weer met hem ging spelen toen zij met de ouders
praatte.
Gedragsregulatie
Van agressief gedrag was geen sprake.
33