Review Article Title Title should be no more than 16 words
advertisement

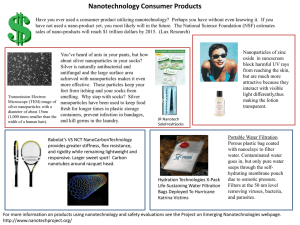
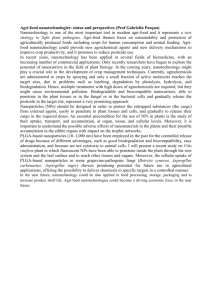
Review Article Title Title should be no more than 16 words. Authorship Authorship criteria should be based only on substantial contributions to each of the three components mentioned below: (1) concept and design of study or acquisition of data or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; (3) final approval of the version to be published. Participation solely in the acquisition of funding or the collection of data does not justify authorship. General supervision of the research group is not sufficient for authorship. Each author should have participated sufficiently in the work to take public responsibility for appropriate portions of the content of the manuscript. The order of the authors should be based on the relative contribution of the author towards the study and writing the manuscript. Authors’ full name should be given (First name + Middle name + Last name). Once submitted, authors cannot be added or deleted and the order cannot be changed also without written consent of all authors. Author institutions The complete name of department, institution, city, province/state, postcode and country should be given. For example, “Department of Burn and Plastic Surgery, Affiliated Hospital of Qingdao University, Qingdao 266003, Shandong, China”, “Division of Plastic, Reconstructive, and Hand Surgery, Baptist Memorial Healthcare Corporation, Memphis, TN 38120, USA”. Correspondence The corresponding author is responsible for communicating with the other authors about revisions and final approval of the proofs. The name, title, institution, address, e-mail and contact number of the corresponding author should be given. For example, “Dr. Zhen-Yu Chen, Department of Burn and Plastic Surgery, Affiliated Hospital of Qingdao University, Qingdao 266003, Shandong, China. E-mail: wzg_qd@126.com. Contact number: +86-29-68686779”. Abstract Review article (200 words) should have unstructured abstracts. First person should not be used in Abstract. Review Article Key words Please list 3-8 key words, which reflect the content of the study. Text The word amount of main text of review article should be 5000 words. Review article has unfixed section titles. Ethics When report studies on human beings, indicate whether the procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional or regional) and with the Helsinki Declaration (available at http://www.wma.net/en/30publications/10policies/b3/). For prospective studies involving human participants, authors are expected to mention about approval of (regional/national/institutional or independent Ethics Committee or Review Board, obtaining informed consent from adult research participants and obtaining assent for children aged over 7 years participating in the trial. The age beyond which assent would be required could vary as per regional and/or national guidelines. Ensure confidentiality of subjects by desisting from mentioning participants’ names, initials or hospital numbers, especially in illustrative material. When reporting experiments on animals, indicate whether the institution’s or a national research council’s guide, or any national law on the care and use of laboratory animals was followed. Evidence for approval by a local Ethics Committee (for both human as well as animal studies) must be supplied by the authors on demand. Animal experimental procedures should be as humane as possible and the details of anesthetics and analgesics used should be clearly stated. The ethical standards of experiments must be in accordance with the guidelines provided by the CPCSEA and World Medical Association Declaration of Helsinki on Ethical Principles for Medical Research Involving Humans for studies involving experimental animals and human beings, respectively). A statement on ethics committee permission and ethical practices must be included in all research articles under the “Methods” section. The journal will not consider any paper which is ethically unacceptable. Selection and description of participants Describe your selection of the observational or experimental participants (patients or laboratory animals, including controls) clearly, including eligibility and exclusion criteria and a description of the source population. Review Article Technical information Identify the methods, apparatus (give the manufacturer’s name and address in parentheses), and procedures in sufficient detail to allow other workers to reproduce the results. Give references to established methods, including statistical methods (see below); provide references and brief descriptions for methods that have been published but are not well known; describe new or substantially modified methods, give reasons for using them, and evaluate their limitations. Identify precisely all drugs and chemicals used, including generic name (s), dose(s), and route(s) of administration. Reports of randomized clinical trials should present information on all major study elements, including the protocol, assignment of interventions (methods of randomization, concealment of allocation to treatment groups), and the method of masking (blinding), based on the CONSORT Statement (http://www.consort-statement.org). Statistics Whenever possible quantify findings and present them with appropriate indicators of measurement error or uncertainty (such as confidence intervals). Authors should report losses to observation (such as, dropouts from a clinical trial). When data are summarized in the “Results” section, specify the statistical methods used to analyze them. Avoid non-technical uses of technical terms in statistics, such as “random” (which implies a randomizing device), “normal”, “significant”, “correlations”, and “sample”. Define statistical terms, abbreviations, and most symbols. Specify the computer software used. Use upper italics (P < 0.048). For all P values include the exact value and not less than 0.05 or 0.001. Mean differences in continuous variables, proportions in categorical variables and relative risks including odds ratios and hazard ratios should be accompanied by their confidence intervals. Results Present your results in a logical sequence in the text, tables, and illustrations, giving the main or most important findings first. Do not repeat in the text all the data in the tables or illustrations; emphasize or summarize only important observations. Extra- or supplementary materials and technical detail can be placed in an appendix where it will be accessible but will not interrupt the flow of the text; alternatively, it can be published only in the electronic version of the journal. When data are summarized, give numeric results not only as derivatives (for example, percentages) but also as the absolute numbers from which the derivatives were calculated, and specify the statistical methods used to analyze them. Restrict tables and figures to those needed to explain the Review Article argument of the paper and to assess its support. Use graphs as an alternative to tables with many entries; do not duplicate data in graphs and tables. Where scientifically appropriate, analysis of the data by variables such as age and sex should be included. Discussion Include summary of key findings (primary outcome measures, secondary outcome measures, results as they relate to a prior hypothesis); strengths and limitations of the study (study question, study design, data collection, analysis and interpretation); interpretation and implications in the context of the totality of evidence (is there a systematic review to refer to, if not, could one be reasonably done here and now? what this study adds to the available evidence, effects on patient care and health policy, possible mechanisms); controversies raised by this study; and future research directions (for this particular research collaboration, underlying mechanisms, clinical research). Do not repeat in detail data or other material given in the Introduction or the Results section. In particular, contributors should avoid making statements on economic benefits and costs unless their manuscript includes economic data and analysis. Avoid claiming priority and alluding to work that has not been completed. New hypotheses may be stated if needed, however they should be clearly labeled as such. Acknowledgments One or more statements should specify: (1) contributions that need acknowledging but do not justify authorship, such as general support by a departmental chair; (2) acknowledgments of technical help; and (3) acknowledgments of financial and material support, which should specify the nature of the support. References References should be created by using Endnote. They should be numbered consecutively in the order in which they are first mentioned in the text (not in alphabetic order). Identify references in text, tables, and legends by Arabic numerals in superscript with square bracket after the punctuation marks. References cited only in tables or figure legends should be numbered in accordance with the sequence established by the first identification in the text of the particular table or figure. All authors’ names should be listed in the references. The names of journals should be abbreviated according to the style used in Index Medicus. Avoid using abstracts as references. Information Review Article from manuscripts submitted but not accepted should be cited in the text as “unpublished observations” with written permission from the source. Avoid citing a “personal communication” unless it provides essential information not available from a public source, in which case the name of the person and date of communication should be cited in parentheses in the text. The commonly cited types of references are shown here, for other types of references please refer to ICMJE Guidelines (http://www.nlm.nih.gov/bsd/uniform_requirements.html). Standard journal articles (list all authors) Parija SC, Ravinder PT, Shariff M. Detection of hydatid antigen in the fluid samples from hydatid cysts by co-agglutination. Trans R Soc Trop Med Hyg 1996;90:255-6. Both personal authors and organization as author Vallancien G, Emberton M, Harving N, van Moorselaar RJ; Alf-One Study Group. Sexual dysfunction in 1,274 European men suffering from lower urinary tract symptoms. J Urol 2003;169:2257-61. Books Sherlock S, Dooley J. Diseases of the liver and billiary system. 9th ed. Oxford: Blackwell Sci Pub; 1993. p. 258-96. Chapter in a book Meltzer PS, Kallioniemi A, Trent JM. Chromosome alterations in human solid tumors. In: Vogelstein B, Kinzler KW, editors. The genetic basis of human cancer. New York: McGraw-Hill; 2002. p. 93-113. Article not in English (The title should be translated into English, and clarify the original language in the bracket.) Zhang X, Xiong H, Ji TY, Zhang YH, Wang Y. Case report of anti-N-methyl-D-aspartate receptor encephalitis in child. J Appl Clin Pediatr 2012;27:1903-7. (in Chinese). Tables Tables should be self-explanatory and should not duplicate textual material. Review Article Number tables, in Arabic numerals, consecutively in the order of their first citation in the text and supply a brief title for each. Place explanatory matter in footnotes, not in the heading. Explain in footnotes all abbreviations that are used in each table. Obtain permission for all fully borrowed, adapted, and modified tables and provide a credit line in the footnote. For footnotes use the following symbols, in this sequence: *, †, ‡, §, ||,¶ , **, ††, ‡‡ Tables with their legends should be provided at the end of the text after the references. The tables along with their numbers should be cited at the relevant places in the text. Figures Upload the images in JPEG format. The file size should be within 2 MB in size while uploading. Figures should be numbered consecutively according to the order in which they have been first cited in the text. Labels, numbers, and symbols should be clear and of uniform size. The lettering for figures should be large enough to be legible after reduction to fit the width of a printed column. Symbols, arrows, or letters used in photomicrographs should contrast with the background and should be marked neatly with transfer type or by tissue overlay and not by pen. Titles and detailed explanations belong in the legends for illustrations not on the illustrations themselves. When graphs, scatter-grams or histograms are submitted the numerical data on which they are based should also be supplied. The photographs and figures should be trimmed to remove all the unwanted areas. If photographs of individuals are used, their pictures must be accompanied by written permission to use the photograph. If a figure has been published elsewhere, acknowledge the original source and submit written permission from the copyright holder to reproduce the material. A credit line should appear in the legend for such figures. Legends for illustrations: type or print out legends (maximum 40 words, excluding the credit line) for illustrations using double spacing, with Arabic numerals corresponding to the illustrations. When symbols, arrows, numbers, or letters are used to identify parts of the illustrations, identify and explain each one in the legend. Explain the internal scale (magnification) and identify the method of staining in photomicrographs. Review Article Final figures for print production: send sharp, glossy, un-mounted, color photographic prints, with height of 4 inches and width of 6 inches at the time of submitting the revised manuscript. Print outs of digital photographs are not acceptable. If digital images are the only source of images, ensure that the image has minimum resolution of 300 dpi or 1800 × 1600 pixels in TIFF format. Send the images on a CD. Each figure should have a label pasted (avoid use of liquid gum for pasting) on its back indicating the number of the figure, the running title, top of the figure and the legends of the figure. Do not write the author/s’ name/s. Do not write on the back of figures, scratch, or mark them by using paper clips. The journal reserves the right to crop, rotate, reduce, or enlarge the photographs to an acceptable size. Abbreviations In general, terms should not be abbreviated unless they are used repeatedly and the abbreviation is helpful to the reader. Standard abbreviations should be defined in the abstract and in the text on first mention. Permissible abbreviations are listed in Units, Symbols and Abbreviations: A Guide for Biological and Medical Editors and Authors (Ed. Baron DN, 1988) published by The Royal Society of Medicine, London. Certain commonly used abbreviations, such as DNA, RNA, ATP, etc., can be used directly without further explanation. Abbreviations are not preferred in the title and key words. Abbreviations used in the tables and figures should be defined in the legends. Units Use SI units. There should be space between number and unit (i.e., 23 mL). Units can be omitted sometimes (i.e., 2 - 3 mL, 2 + 3 mL) while sometimes not (i.e., 2 cm × 3 cm). Hour, minute, second should be written as h, min, s. However, day, month and year cannot be abbreviated. Numbers Numbers appearing at beginning of sentences should be expressed in English. When there are two or more numbers in a paragraph, they should be expressed as Arabic numerals; when there is only one number in a paragraph, number < 10 should be expressed in English and number > 10 should be expressed as Arabic numerals. 23243641 should be written as 23,243,641. Italics Review Article General italic words like vs., et al., etc., in vivo, in vitro; t test, F test, U test; related coefficient as r, sample number as n, and probability as P; names of genes; names of bacteria and biology species in Latin. MANUSCRIPTS SUBMISSION All manuscripts must be submitted on-line through the website http://www.journalonweb.com/par/. First time users will have to register at this site. Registration is free but mandatory. Registered authors can keep track of their articles after logging into the site using their user name and password. Authors do not have to pay for submission, processing or publication of articles. If you experience any problems, please contact the editorial office by e-mail at par_editor001@parjournal.net or pareditor002@gmail.com. Generally, the manuscript should be submitted in the form of several separate files: First page This file should provide: 1. The type of manuscript, title of the manuscript, names of all authors, and their institutions. All information which can reveal your identity should be here. 2. The name, title, address, e-mail, and telephone number of the corresponding author, who is responsible for communicating with the other authors about revisions and final approval of the proofs. 3. The total number of photographs and word counts separately for abstract and for the text (excluding the references, tables and abstract), word counts for introduction + discussion in case of an original article. 4. Acknowledgements, if any. 5. Source(s) of support, if any. 6. If the manuscript was presented as part at a meeting, the organization, place, and exact date on which it was read. 7. Registration number in case of a clinical trial and where it is registered (name of the registry and its URL). 8. Conflicts of interest of each author/ contributor. A statement of financial or other relationships that might lead to a conflict of interest, if that information is not included in the manuscript itself or in an authors’ form. Blinded article file Review Article The main text of the article, beginning from Abstract till References (including tables) should be in this file. The file must not contain any mention of the authors' names or initials or the institution at which the study was done or acknowledgements. Manuscripts not in compliance with the journal’s blinding policy will be returned to the corresponding author. Limit the file size to 1 MB. Do not incorporate figures in the file. The pages should be numbered consecutively, beginning with the first page of the blinded article file. Images Submit good quality color images. Each image should be less than 2 MB in size. Size of the image can be reduced by decreasing the actual height and width of the images (keep up to 1600 × 1200 pixels or 5-6 inches). Images can be submitted as JPEG files. Do not zip the files. Legends for the figures/images should be included at the end of the article file. Presentation and format All articles should be written in American English, submitted using word-processing software, and typed in 1.5 line spacing. The font should be Times New Roman, and the size should be 10.5. Review Article First Page Review Article Article Title: Current and future applications of nanotechnology in plastic and reconstructive surgery Author Information: Dana K. Petersen1, Tate M. Naylor2, Jon P. Ver Halen3,4,5 1 Department of Otolaryngology - Head and Neck Surgery, University of Tennessee Health Science Center, Memphis, TN 38163, USA. 2 Department of Surgical Oncology, School of Medicine, University of Tennessee Health Sciences Center, Memphis, TN 38163, USA. 3 Department of Surgical Oncology, Division of Plastic, Reconstructive and Hand Surgery, Baptist Memorial Healthcare Corporation, Memphis, TN 38120, USA. 4 Department of Surgical Oncology, Vanderbilt Ingram Cancer Center, Nashville, TN 37232, USA. 5 Department of Surgical Oncology, St Jude Children’s Research Hospital, Memphis, TN 38105, USA. Address for correspondence: Dr. Jon P. Ver Halen, Department of Surgical Oncology, Division of Plastic, Reconstructive and Hand Surgery, Baptist Memorial Healthcare Corporation, Memphis, TN 38120, USA. E-mail: jpverhalen@gmail.com Phone: +86-29-68686779 Total number of photographs: Word counts For abstract: For the text: Acknowledgements: Source(s) of support: Presentation at a meeting Organization: Place: Date: Conflicting Interest (If present, give more details): Review Article Article File Current and future applications of nanotechnology in plastic and reconstructive surgery ABSTRACT Although nanotechnology is a relatively young field, there are countless biomedical applications in use or under investigation. Many specialties have benefitted from nanoscale refinements of diagnostic and therapeutic techniques. Plastic and reconstructive surgery is an incredibly diverse specialty, encompassing craniofacial and hand surgery; trauma, oncologic and congenital reconstruction; burn care, and aesthetic surgery. Advances in nanotechnology have significantly impacted wound management, topical skin care, implant and prosthetic design, tissue engineering, and drug delivery systems. Currently, plastic surgeons are researching the utility of nanoscale tools for bone regeneration, bone prosthetics, and drug delivery. Nanotechnology will continue to build upon preceding discoveries, and its biomedical applications in the field of plastic and reconstructive surgery will expand significantly. Key words: Bone graft, burns, drug delivery, implants, nanotechnology, tissue engineering, wound care INTRODUCTION Nanotechnology can be defined as the science of design, synthesis, characterization and application of materials and extremely small devices. The smallest functional unit of this technology, in at least one dimension, is on the nanometer scale, which is one billionth of a meter.[1-3]Nanotechnology is the design and engineering of novel products that interact with biological, electrical and chemical systems on the atomic level, thus yielding a level of specificity and specialization that was not feasible in the past. In the 1950’s, European researchers discovered formation of an active biological field from the oxidation of titanium when exposed to air. They identified that this promotes living tissue ingrowth.[4] This phenomenon was used to take a tremendous leap in medical technology, specifically in bone implant applications. Nanomedicine Review Article is a subdivision of nanotechnology that employs highly specific molecular interventions for both the diagnosis and treatment of disease processes. Currently, nanomedicine has allowed advancement in the fields of drug delivery systems, gene therapies, body and organ imaging, surgical tools, and diagnostic procedures. SOFT TISSUE REPAIR AND HEALING Wound and burn care are two areas of clinical care that are already benefitting from developments in nanotechnology.[5] Wound dressings constructed using nanoscale fabrication techniques can greatly improve wound healing. Nanofibers may be created from various materials using manufacturing techniques on a nanoscale. The nanofibers provide a three-dimensional structure that mimics the native extracellular matrix (ECM) while the host tissue regeneration replaces the scaffold. Nanofiber scaffolds provide several properties that are essential for tissue repair: mechanical integrity, temperature control, fluid absorption, and gas exchange. In rat models, scaffolds made of collagen nanofibers accelerate acute wound healing by enhancing capillary and fibroblast proliferation.[6] In a study by Choi et al.,[6] recombinant human epidermal growth factor (EGF) was immobilized on electrospun biodegradable nanofibers to treat diabetic ulcers in a rat model. Human primary keratinocytes were cultivated on the nanofiber matrix to investigate the effect of EGF nanofibers on their differentiation. Wound healing effect of the EGF nanofibers was confirmed in diabetic animals with dorsal wounds. In in-vivo wound healing studies, the EGF-nanofibers group was superior to control groups (conventional dressing, nanofibers alone, or EGF solutions). This study showed that EGF-conjugated nanofibers could potentially be employed as a novel wound healing material by increasing proliferation and phenotypic expression of keratinocytes in diabetic wounds. Chitin and chitosan nanofibrils are nanocrystals of natural polysaccharides derived from the exoskeletons of crustaceans. These fibrils have been used in a variety of formulations to aid wound healing. Muzzarelli et al.[7] showed in murine models that different formulations of chitin nanofibrils almost lead to normal physiologic repair of wounds. They subjected various formulations of dibutyryl chitin (DBC), a modified chitin carrying butyryl group at the 3 and 6 Review Article positions, to a battery of in vitro and in vivo tests. The DBC’s were then incorporated into a 5-methylpyrrolidinone chitosan solution and submitted to freeze-drying to produce a reinforced wound dressing material which was then tested in vivo in full thickness wounds in rats. The rats had full thickness dorsal wounds bilaterally and treated with experimental agent on one side, and control on the contralateral side. The animals were studied at either seven or fourteen days and the skin of each surgical wound was excised. The use of 4mm ×4 mm pieces as wound dressings resulted in significantly less cutaneous scarring, as measured by collagen I/ collagen III rations, and as measured clinically. Chitin nanofibrils/chitosan glycolate can be manufactured into a spray, gel or impregnated onto a dressing for wound care. Using a rat model, Mattioli-Belmonte et al.[8] demonstrated that each of these delivery systems has a specific application: use for superficial abrasions, shallow wounds in aesthetic areas, and slow healing dermo-epidermal wounds, respectively. Enhanced tissue repair and reduced scarring was seen in all the applications. Although the results from all of these studies are impressive, they have not been examined in human clinical trials. Silver has long been heralded for its antimicrobial properties and has demonstrated efficacy against multi-drug resistant organisms as well as exhibiting anti-inflammatory properties.[9,10]Nanoscale fabrication techniques have allowed manufacturing silver into nanoparticles, which markedly increases the rate of silver ion release, and thus increasing its clinical utility.[10,11] A nanocrystalline silver dressing was recently evaluated in chronic wounds by Sibbald et al.[9] In a prospective, uncontrolled study, a variety of chronic, nonhealing wounds (foot, pressure, and venous stasis ulcers, and miscellaneous wounds) were treated with a nanocrystalline sliver dressing [Figure 1]. Surface bacterial counts were found on semi-quantitative swabs to be significantly diminished in those wounds treated with nanocrystalline dressing. Since bacteria contribute to tissue damage leading to poor wound healing, the decreased bacterial load from silver nanocrystalline dressing facilitates wound healing.. Additionally, growth factors have been shown to play a critical role in the proliferative phase of wound healing. Growth factors serve to attract the cells necessary for fibroblast and epithelial cell growth and migration, as well as initiating the formation of new blood vessels into the area of injury. Novel polymerized Review Article nanocarriers have been produced, which can provide for consistent and significant dosages of growth factors. The growth factors are embedded into the polymerized nanocarriers that allow sustained release of these bioactive molecules. The nanocarrier drug delivery system has beensuccessful in treating wounds in a clinical setting.[10] The cosmetic and topical skin care industries have also benefited from advances in nanotechnology. For example, micronized zinc oxide and titanium dioxide are used in sunscreen manufacturing by functioning as UV blockers in these products. Their nanoscale fabrication increases their transparency on skin and allows increased user compliance. In addition, it also increases their refractive index, resulting in a “stronger” sunscreen.[12] Lipid nanoparticles have been added to various cosmetic and dermal products to increase contact with the stratum corneum. Therefore, it allows increased drug penetration in to the skin, improved hydration through their occlusive properties, and provide controlled release of active ingredients.[13] In an open clinical trial, fullerene gel applied to patients with acne vulgaris showed a significant reduction cutaneous inflammation and infection, suggesting yet another application of nanotechnology in skin care.[14] IMPLANTS AND PROSTHESES In 2012, breast augmentation and implant-based breast reconstruction after mastectomy were the most common plastic surgery procedures. Breast implants that contain nanofiber coatings for the delivery of tumor-specific anti-cancer drugs are currently being evaluated.[15] This technology has the potential to revolutionize cancer care, by facilitating area-specific chemotherapy to the tumor bed, while alleviating some of the undesirable effects of current systemic chemotherapy regimens. In addition, utilizing nanoscale technology in manufacturing can improve the strength of breast implants. The shell of silicone breast implants is made up of cross-linked and reinforced silicone rubber nanocomposite. The silicone rubber is weak and therefore must be reinforced, most commonly with nanosized SiO2. Finally, even with modern breast implants, capsular contracture continues to be one of the significant long-term complications of long-term breast implant placement. It has been demonstrated in a rat model that surface modification of implants with antifibrotic drugs (e.g., halofuginone) can decrease capsule formation.[16] Review Article TISSUE AND ORGAN ENGINEERING Nanotechnology has been used to construct and repair various tissues utilized in plastic surgery. Electrospun nanofiber matrices have been developed for skeletal muscle regeneration in both in vitro and in vivo experimental models.[17] Reconstructive plastic surgeons are currently using cartilage engineering that has been utilized in orthopedic surgery for many years. The engineering of auricular cartilage for ear reconstruction is an established technique. Additionally, nasal cartilage is being examined for complex nasal reconstruction after cancer, trauma, or congenital defects.[18] Artificial skin has long been used for the treatment of skin defects. Currently, the use of scaffolds composed of polylactic and polyglycolic acids embedded with various growth factors are used to improve skin healing.[19,20] With precise manufacturing techniques and the utilization of novel biomaterials, the development of these products can provide enhanced aesthetic appearance after reconstruction. This has been proven to be safe, reliable, and reproducible. NERVE TUBULIZATION Nerve regeneration is an area of particular interest to both plastic surgeons and nanotechnology researchers. Plastic surgeons perform majority of the peripheral nerve surgeries involving the hands, face, and trunk..[21,22] Traumatic nerve injuries resulting in loss of nerve tissue over 5mm frequently require nerve grafting, often from an autologous source. Donor sites for this procedure, however, are limited. To avoid the morbidity of autologous nerve grafting, nanoscale manufacturing techniques have been employed to develop new approaches in peripheral nerve repair. Tubular and porous nanostructured conduits, using various natural materials, have been developed to guide regenerating nerves. These structures have been loaded with various biomaterials or cell types (e.g., embryonic stem cells, Schwann cells, neural stem cells) to aid regeneration. Chitosan nanofiber mesh tubes were studied in sciatic nerve injuries in a rat model by Wang et al.,[23] in which they noted partial recovery of sensory function as the nerves elongated through the tubes. Biodegradeable micropatterned scaffolds that mimic the extracellular membrane can also be coated with laminin and seeded with Schwann cells to guide neuron alignment and promote axon regeneration after injury.[19] Currently researchers are designing neural interfaces between the peripheral and central nervous system, and limb prostheses for Review Article patients with traumatic amputations and spinal cord injuries.[24,25] NANOTECHNOLOGY IN BONE BIOLOGY AND REPAIR Current developments in bone matrix depends on the understanding that the bone microenvironment is made up of progenitor cells, mineralized extracellular matrix scaffold, soluble chemical signals (such as cytokines), and mechanical stimuli.[26] Nanoscale fabrication techniques can improve each of these components. Scaffolds made of nanomaterials provide a geometric porous structure that allows osteoblastic differentiation.[27] Such techniques are conceptually simple, yet were not technically possible until the development of modern nanoscale fabrication techniques. Advances in fabrication and manufacturing make nanotechnology an exciting and powerful tool in the development of bone reconstruction. BONE PROSTHESES Nanotechnology can be used to manipulate the surfaces of standard bone replacement implants to maximize tissue ingrowth while minimizing inflammation. Raimondo et al.[28] recently investigated the use of electron beam absorption to resurface standard titanium and polyethylene implant surfaces. Then they evaluated them for surface characterization, surface energy and contact angles, and osteoblast and endothelial cell adhesion [Figure 2]. They found that the nano-roughened surfaces were more favorable in each category.While unmodified titanium surfaces demonstrated excellent adhesion of both osteoblasts and endothelial cells, once modified, the polyethylene surface showed significantly increased osteoblast adhesion and showed similar endothelial cell adhesion. This study introduces a novel process to efficiently nano-roughen materials and provides an additional example of nanotechnology use to enhance the performance of standard synthetic materials. Liu et al.[29]re-emphasizing the importance of the homogenous dispersion of poly-DL-lactic-co-glycolic acid (PLGA) nanoparticles for optimal enhancement of cell adhesion. They demonstrated that PLGA prosthetics enhanced with a well-dispersed nanoceramic coating had improved load-bearing limitations. This improved mechanical strength was most likely due to the strong bonds between nanoparticles and PGLA, as conveyed by the fine ultrastructure of the Review Article particles. This enhancement of mechanical strength, through the application of nanoparticles, is a previously underappreciated finding in nanomaterials. Finally, this work highlights that the three-dimensional structure of nanoparticles and its interactions can increase their applications. Hydroxyapatite (HA) is currently used to fill bone defects by itself or as a prosthetic coating. While HA has advantages over other bioceramics, such as creating strong bonds with native tissues, it lacks a homogeneous degradation phase. Given the nanoscale architecture of native bone crystals, manufacturing HA on a nanoscale would theoretically improve its utility. Poinern et al.[30] have investigated the effects of thermal and ultrasonic techniques for the development of these particles and demonstrated that either technique can generate particles of similar consistency. El-Fattah et al.[31] histomorphometrically analyzed the tissue by growth and scaffold degradation in 3 groups of rats with identical bone defects: one filled with mirco-HA, one with nano-HA and one control group without filler. They found increased reactive bone formation and biocompatibility in nano-HA group compared to other groups. These findings have immediate implications for improving the utility of HA for craniofacial, hand, extremity, and truncal bone reconstructive applications. BONE REGENERATION In addition to aiding the development of bone prosthetics, nanotechnology also provides many inroads to improve bone regeneration. The induction of progenitor cells into osteoblasts is an important component of bone regeneration. A novel application of nanotechnology to achieve this goal is the application of specific nanoscale surfaces to produce specific cellular responses, such as osteoblastic differentiation. Oh et al.[27] investigated the effect of culturing human mesenchymal stem cells (hMSC) on titanium dioxide (TiO2) nanotubes ranging in size from 30 nm to 100 nm. They found that the larger nanotubes forced the elongation of the hMSCs and consequently encouraged differentiation into osteoblastic cell lines. They proposed that smaller nanotubes capture local proteins easily and establish an extracellular matrix-like environment allowing for easy hMSC adhesion. In larger nanotubes, there is less capture of local proteins and the hMSCs require to stretch and develop filopodia to elongate across the surface and establish adequate adhesion [Figure 3]. This geometrical manipulation provides the cytoskeletal stress Review Article theorized to induce osteoblastic differentiation. This technique could feasibly improve previous methods of osteoinduction that involve gene therapy.[32] NANOTECHNOLOGY IN MAXILLOFACIAL SURGERY Nanotechnology has the potential to bring enormous changes to the fields of maxillofacial surgery and dentistry through the aid of nanorobotics, nanomaterials, and biotechnology.[33] Nanorobots have a diameter of 0.5-3 µm and are made of components sized from 1 nm to 100 nm. They can be programmed, thus enabling clinicians to execute accurate procedures at the cellular and molecular levels. Specifically, they have roles in local anesthesia, diagnostics, therapeutics, dental and maxillofacial hard tissue repositioning, and dentifrice. In maxillofacial surgery, nanomaterials can be used as bone replacement materials, prosthetic implants, dental fillers, dental restorative materials, impression materials, and even for orthodontic wires exhibiting very high strength and excellent deformability, corrosion resistance, and surface finish. Finally, tissue engineering with natural nanomaterials holds the potential to completely reconstruct a patient’s dentition and craniofacial skeleton. DRUG DELIVERY Nanoscale technologies have numerous applications in drug delivery [Table 1]. Bone infections can be catastrophic and are difficult to manage even in the age of modern antibiotics and best surgical techniques.[34] Plastic surgeons are frequently involved in management of these problems because they provide technical expertise with vascularized tissue transfer and soft tissue reconstruction. Deep tissue infection with multiple drug resistant organisms coupled with the morbidity of serial operations and potentially toxic systemic therapies begs for the introduction of new approaches. The antimicrobial properties of silver have long been appreciated and current nanotechnological techniques have allowed the production of nanoscaled silver particles with a very high surface to mass ratio. Zheng et al.[38] examined PLGA composite grafts treated with nanosilver compared to PLGA controls [Figure 4]. They were able to demonstrate that this composite had strong antimicrobial properties and that the presence of the nanosilver did not affect the osteoinductive properties of PLGA in the presence of bone morphogenic protein-2 Review Article (BMP-2). In a rat model, nanosilver-PLGA composite grafts demonstrated complete healing without residual bacteria, while control animals had residual bacterial contamination. This study shows that silver can be used as an antimicrobial agent in grafts, while previous studies showed its topical use. Colilla et al.[36] examined silica-based mesoporous materials to characterize the features that determine the loading capacity and delivery of medications integrated into these devices. They specifically focused on silica-based mesoporous materials because they can be manufactured with a high degree of homogeneity with a tunable pore size. Their work highlights the importance of pore size, volume, and surface area in both drug adsorption and drug elution from the device. Nanotechnology has further applications beyond the fabrication of devices and materials on the nanoscale. Nanotechnology also allows us to study and quantify biological processes at this level using various techniques. Differences of regional bone on the nanoscale may allow for improved or novel harvesting techniques in addition to infrequently used donor sites for graft harvest. Through this knowledge, we can improvise the architecture of materials to increase success rate in tissue reconstruction. Leong et al.[37] have utilized tissue characterization on the nanoscale to categorize the various tissues present during bone callus formation. Understanding bone healing biology at the nanoscale will help us develop ways to improve this process for reconstructive purposes. CANCER TREATMENT Cancer treatment often involves multiple modalities, including surgery, chemotherapy, and radiation therapy. The single most important predictor of patient survival for cancer is complete surgical resection. Nanometer-sized particles such as quantum dots and colloidal gold have novel size-tunable properties that neither discrete molecules nor bulk materials can provide.[38] These particles have potential for tumor localization, tumor margin detection, identification of important adjacent structures, mapping of sentinel lymph nodes, and detection of residual tumor cells or micrometastases. Contrast agents containing such particles can be accumulated in solid tumors through passive and active targeting mechanisms. In addition, intraoperative imaging can be used Review Article to overcome problems with tissue penetration of traditional optical methods [Figure 5]. Such agents include quantum dots, and surface-enhanced Raman scattering nanoparticles. Evaluating the long-term fate and toxicity of nanoparticles remains a challenge. Finally, it is important to design agents that are accumulated in tumors but are cleared from other organs and tissues. In conclusion, nanotechnology has a vast array of applications in plastic and reconstructive surgery [Table 2]. Specifically, wound management, topical skin care, implant and prosthetic design, tissue engineering, and drug delivery systems have each been influenced by advances in nanotechnology. As our understanding of biology on the nanolevel progresses, the use of this technology will increase exponentially. These characteristics make nanotechnology a powerful tool when applied to all aspects of tissue reconstruction. Review Article REFERENCES 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. Sahoo SK, Parveen S, Panda JJ. The present and future of nanotechnology in human health care. Nanomedicine 2007;3:20-31. Wong IY, Bhatia SN, Toner M. Nanotechnology: emerging tools for biology and medicine. Genes Dev 2013;27:2397-408. Saadeh Y, Leung T, Vyas A, Chaturvedi LS, Perumal O, Vyas D. Applications of nanomedicine in breast cancer detection, imaging, and therapy. J Nanosci Nanotechnol 2014;14:913-23. Rajesh O, Gitanjaly S, Surbhi M. Nano-Bio-Technology Excellence in Health CareNano-Bio-Technology Excellence in Health Care: A Review. Internet J Nanotechnol 2004;1. Available from: http://ispub.com/IJNT/1/2/7910 Hromadka M, Collins JB, Reed C, Han L, Kolappa KK, Cairns BA, Andrady T, van Aalst JA. Nanofiber applications for burn care. J Burn Care Res 2008;29:695-703. Choi JS, Leong KW, Yoo HS. In vivo wound healing of diabetic ulcers using electrospun nanofibers immobilized with human epidermal growth factor (EGF). Biomaterials 2008;29:587-96. Muzzarelli RA, Guerrieri M, Goteri G, Muzzarelli C, Armeni T, Ghiselli R, Cornelissen M. The biocompatibility of dibutyryl chitin in the context of wound dressings. Biomaterials 2005;26:5844-54. Mattioli-Belmonte M, Zizzi A, Lucarini G, Giantomassi F, Biagini G, Tucci G,Orlando F, Provinciali M, Carezzi F, Morganti P. Chitin nanofibrils linked to chitosan glycolate as spray, gel, and gauze preparations for wound repair. J Bioact Compat Pol 2007;22:525-38. Sibbald RG, Browne AC, Coutts P, Queen D. Screening evaluation of an ionized nanocrystalline silver dressing in chronic wound care. Ostomy Wound Manage 2001;47:38-43. Cortivo R, Vindigni V, Iacobellis L, Abatangelo G, Pinton P, Zavan B. Nanoscale particle therapies for wounds and ulcers. Nanomedicine (Lond) 2010;5:641-56. Wu J, Zheng Y, Wen X, Lin Q, Chen X, Wu Z. Silver nanoparticle/bacterial cellulose gel membranes for antibacterial wound dressing: investigation in vitro and in vivo. Biomed Mater 2014;9:035005. Morganti P. Use and potential of nanotechnology in cosmetic dermatology. Clin Cosmet Investig Dermatol 2010;3:5-13. Muller RH, Shegokar R, Keck CM. 20 years of lipid nanoparticles (SLN and NLC): present state of development and industrial applications. Curr Drug Discov Technol 2011;8:207-27. Inui S, Aoshima H, Nishiyama A, Itami S. Improvement of acne vulgaris by topical fullerene application: unique impact on skin care. Nanomedicine 2011;7:238-41. Puskas JE, Luebbers MT. Breast implants: the good, the bad and the ugly. Can nanotechnology improve implants? Wiley Interdiscip Rev Nanomed Nanobiotechnol 2012;4:153-68. Zeplin PH, Larena-Avellaneda A, Schmidt K. Surface modification of silicone breast implants by binding the antifibrotic drug halofuginone reduces capsular fibrosis. Plast Review Article 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. Reconstr Surg 2010;126:266-74. Klumpp D, Horch RE, Kneser U, Beier JP. Engineering skeletal muscle tissue--new perspectives in vitro and in vivo. J Cell Mol Med 2010;14:2622-9. Oseni A, Crowley C, Lowdell M, Birchall M, Butler PE, Seifalian AM. Advancing nasal reconstructive surgery: the application of tissue engineering technology. J Tissue Eng Regen Med 2012;6:757-68. Gerstle TL, Ibrahim AM, Kim PS, Lee BT, Lin SJ. A plastic surgery application in evolution: three-dimensional printing. Plast Reconstr Surg 2014;133:446-51. Hu MS, Maan ZN, Wu JC, Rennert RC, Hong WX, Lai TS, Cheung AT, Walmsley GG, Chung MT, McArdle A, Longaker MT, Lorenz HP. Tissue Engineering and Regenerative Repair in Wound Healing. Ann Biomed Eng 2014;10.1007/s10439-014-1010-z. Sivolella S, Brunello G, Ferrarese N, Della Puppa A, D'Avella D, Bressan E, Zavan B. Nanostructured guidance for peripheral nerve injuries: a review with a perspective in the oral and maxillofacial area. Int J Mol Sci 2014;15:3088-117. Konofaos P, Ver Halen JP. Nerve repair by means of tubulization: past, present, future. J Reconstr Microsurg 2013;29:149-64. Wang W, Itoh S, Konno K, Kikkawa T, Ichinose S, Sakai K, Ohkuma T, Watabe K. Effects of Schwann cell alignment along the oriented electrospun chitosan nanofibers on nerve regeneration. J Biomed Mater Res A 2009;91:994-1005. Sedaghati T, Yang SY, Mosahebi A, Alavijeh MS, Seifalian AM. Nerve regeneration with aid of nanotechnology and cellular engineering. BiotechnolApplBiochem 2011;58:288-300. Tavangarian F, Li Y. Carbon nanostructures as nerve scaffolds for repairing large gaps in severed nerves. Ceramics International 2012;38:6075-90. Biggs MJ, Dalby MJ. Focal adhesions in osteoneogenesis. Proc Inst Mech Eng H 2010;224:1441-53. Oh S, Brammer KS, Li YS, Teng D, Engler AJ, Chien S, Jin S. Stem cell fate dictated solely by altered nanotube dimension. Proc Natl Acad Sci U S A 2009;106:2130-5. Raimondo T, Puckett S, Webster TJ. Greater osteoblast and endothelial cell adhesion on nanostructured polyethylene and titanium. Int J Nanomedicine 2010;5:647-52. Liu H, Webster TJ. Mechanical properties of dispersed ceramic nanoparticles in polymer composites for orthopedic applications. Int J Nanomedicine 2010;5:299-313. Poinern GJ, Brundavanam R, Le XT, Djordjevic S, Prokic M, Fawcett D. Thermal and ultrasonic influence in the formation of nanometer scale hydroxyapatite bio-ceramic. Int J Nanomedicine 2011;6:2083-95. Abd El-Fattah H, Helmy Y, El-Kholy B, Marie M. In vivo animal histomorphometric study for evaluating biocompatibility and osteointegration of nano-hydroxyapatite as biomaterials in tissue engineering. J Egypt Natl Canc Inst 2010;22:241-50. Polini A, Pisignano D, Parodi M, Quarto R, Scaglione S. Osteoinduction of human mesenchymal stem cells by bioactive composite scaffolds without supplemental osteogenic growth factors. PLoS One 2011;6:e26211. Bhardwaj A, Bhardwaj A, Misuriya A, Maroli S, Manjula S, Singh AK. Nanotechnology in dentistry: Present and future. J Int Oral Health 2014;6:121-6. Uskokovic V, Desai TA. Simultaneous bactericidal and osteogenic effect of Review Article 35. 36. 37. 38. nanoparticulate calcium phosphate powders loaded with clindamycin on osteoblasts infected with Staphylococcus aureus. Mater Sci Eng C Mater Biol Appl 2014;37:210-22. Kose N, Otuzbir A, Peksen C, Kiremitci A, Dogan A. A silver ion-doped calcium phosphate-based ceramic nanopowder-coated prosthesis increased infection resistance. Clin Orthop Relat Res 2013;471:2532-9. Leong PL, Morgan EF. Measurement of fracture callus material properties via nanoindentation. Acta Biomater 2008;4:1569-75. Singhal S, Nie S, Wang MD. Nanotechnology applications in surgical oncology. Annu Rev Med 2010;61:359-73. Zheng Z, Yin W, Zara JN, Li W, Kwak J, Mamidi R, Lee M, Siu RK, Ngo R, Wang J, Carpenter D, Zhang X, Wu B, Ting K, Soo C. The use of BMP-2 coupled – Nanosilver-PLGA composite grafts to induce bone repair in grossly infected segmental defects. Biomaterials 2010;31:9293-300. Review Article FIGURES AND TABLES Table 1: Nanoscale drug delivery technologies[1](Used with permission) Drug delivery technology Materials Nanostructure forms Biologic Lipids Peptides Nucleic acids Polysaccharides Viruses Poly(lactic acid) Poly(glycolic acid) Poly(alkylcyanoacrylate) Poly(3-hydroxybutanoic acid) Poly(organophosphazene) Poly(ethylene glycol) Poly(caprolactone) Poly(ethylene oxide) Poly(amidoamine) Poly(L-glutamic acid) Poly(ethyleneimine) Poly(propylene imine) Silicon Silicon dioxide Carbon Gold Silver Palladium Platinum Versicles, nanotubes, rings Nanoparticles Polymeric Silicon based Carbon based Metallic Vesicles, spheres, nanoparticles Micelles, dendrimers Porous, nanoparticles Nanoneedles Nanotubes, fullerness Nanoparticles, nanoshells Table 2: Summary of nanotechnology applications in plastic and reconstructive surgery Material Device Application Lipids, peptides, nucleic acids, polysaccharides, viruses Peptides, antibodies Vesicles, nanoparticles Activatable probes, tumor paints Tumor targeting, theranostics Polymers (poly- lactic acid, glycolic acid, caprolactone, propylene, etc) Vesicles, nanoparticles, dendrimers Drug delivery nanotubes, spheres, micelles, Drug delivery Review Article Silicone, silicone dioxide Nanoparticles, nanoneedles Nanotubes, fullerenes Drug delivery Semiconductor quantum dots Nanoparticles, nanoshells Tumor targeting Surface-enhanced Raman scattering Tumor targeting lactate, poly glycolic Layered scaffolds lactate, poly glycolic Contoured scaffolds lactate, poly glycolic lactate, poly glycolic Flexible scaffolds, bioreactors Hydrogel scaffolds Poly lactate, poly glycolic acid Collagen Rigid scaffolds, mineralized substrates Nanofibers Composite skin grafts, chronic wounds, burn wounds, skin diseases Customized fat grafts, breast reconstruction Functional muscle grafts, solid organ transplants Moldable cartilage scaffolds, craniofacial & skeletal reconstruction, dental restoration and reconstruction Bone grafts Chitosan Nanofibrils Wound, burn care Silver Nanoparticles Wound and burn care Zinc oxide, titanium dioxide Nanoparticles Sunscreen Fullerene, lipids Vesicles, nanoparticles Silicone, silicone dioxide Nanofiber, nanoparticle Breast implants Peptides, collagen, PLGA, chitosan Flexible nanofibers Nerve conduits PLGA, polyethylene Hydroxyapatite Nanoscale surfacing Bone prostheses and implants Bone replacement, implant coating Titanium, carbon Nanoparticles, coating Nanotubes Carbon, metal colloids Nanorobots Carbon Carbon Gold, silver, platinum palladium, Gold Poly acid Poly acid Poly acid Poly acid Titanium, nanotubes, scaffolds, implant Drug delivery Drug delivery, quantum dots, tumor detection Wound care Skin care products Bone regeneration scaffolds Tissue healing, bone replacement, tumor theronostics, anesthesia Review Article Ceramics (nonorgainic, nonmetallic compounds) Nanocoating, nanofibers, nanocomposites Bone restoration, reconstruction PLGA: Poly-DL-lactic-co-glycolic acid Figure 1: Histological staining of healed skin in each experimental group. Masson Trichome staining shows the distribution and density of collagen protein in healed skin in various groups. Collagen protein was stained blue, nuclei are stained black and the background (muscle, cytoplasm and keratin) are stained red. IHC staining shows the expression of collagen type I and type III of healed skin in normal skin, silver treated, and untreated groups, respectively. (Scale bar: 20 micrometers).[9](Used with permission.) Figure 2: Scanning electron microscopy images of (a) conventional titanium (Ti), (b) nanorough Ti, (c) conventional PE, and (d) nanorough PE. Scale bars in (a) and (b) are 200 nm while (c) and (d) are 1 μm.[28] (Used with permission) Figure 3: Filopodia of endothelial cells induced by nanotopography.[27](Used with permission) Figure 4: In vivo antibacterial activity of nanosilver particle- poly-DL-lactic-co-glycolic acid (PLGA) composite grafts. After 2-week contamination with 10[8] CFU S. aureus Mu50, rat femoral segmental defects with implanted grafts were harvested, fixed, decalcified, embedded, sectioned and stained with Taylor modified Brown and Brenn gram stain as well as HE. Compared to serious bacterial infection (black dots) found in control PLGA grafts (a), 1.0% nanosilver-PLGA composite grafts significantly reduced bacterial survival to colonized collation (b, red arrows). On the other hand, only limited bacterial colonies (red arrows) were observed in 2.0% nanosilver particle-PLGA composite grafts in vivo (c), and more red blood cells (blue arrows) were found in the grafts instead of phagocytes (black arrows).[38] (Used with permission) Figure 5: Active versus passive targeting of cancerous tissue. Nanoparticles passively diffuse Review Article through the highly permeable endothelial layer of blood vessels in cancer tissue. In addition, decreased lymphatic drainage from solid cancer tissue prevents the nanodrug from returning to the systemic circulation. Active nanodrugs target the tumor tissue with engineered tissue-specific ligands on the surface of the nanodrug.[2] (Used with permission)