SAAHE-Plenary-2014-Steve
advertisement

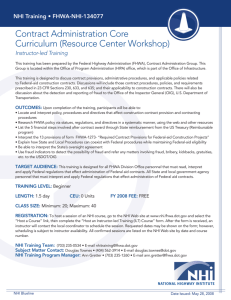
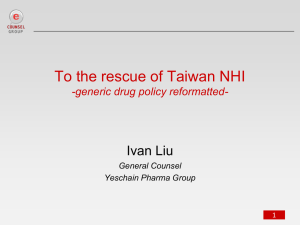
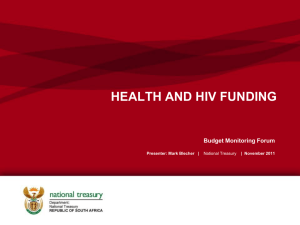
1 SAAHE Plenary Speech 27th June 2014 Steve Reid Primary Health Care Directorate Faculty of Health Sciences University of Cape Town HEALTH PROFESSIONALS EDUCATION FOR THE NHI Thank you for the honour of being the first South African plenary speaker at SAAHE. I guess I should do that justice by bringing some of the excellent ideas presented yesterday into our local context. This is a talk about the future, thinking about and planning the next generation of health professionals. It is therefore in the realm of imagination - yours and mine - to project us forward to 2025 and begin our thinking with that context in mind. Thanks to Brian O'Connell, Jason Frank and Ian Couper yesterday, I have an excellent base to build on. My area of work is in the area between health sciences education and health systems, and within both of those, between personal clinical care and population-based care. Jason Frank gave us an eloquent outline of competency-based education, and Ian Couper emphasized the importance of context. I want to put this competence into the future context of a single national health system, such as has been proposed in terms of the NHI. Professor O'Connell recounted the poem Caravel, about the appearance of a ship for the first time off the north American coast, and likened the HIV epidemic 20 years ago to this apparition. At that time, we did not recognise it, we did not know how to respond. The NHI is like our contemporary Caravel, but the difference is that it is not an entirely foreign object - it is the “Big Canoe” of our own construction. The aim of my lecture is to encourage all of us to help build it, together. So I would like to get into this through a story - an imagined story, constructed from what we 2 what we know now - that approximates the situation as best as we can. I would like to do it through a story because stories allow for complexity and a certain quirkiness, individuality and digressions, and they take the contextual situation into account as part of the story. Instead of reams of statistics, or cross-sectional views, stories are longitudinal in nature, and therefore more dynamic. You can't take notes from a story - rather, you have to engage your own imagination and become an active participant. And since this is all conjecture, I can make it up as I go along. So here goes. Thinking forward, a first year medical student in 2015 will graduate in 2020, complete CS in 2023 and be ready to practice independently in 2024. So if all goes according to plan, our medical intake in 6 months from now will be NHI doctors. I will retire in 2024 and in my retirement I plan to buy a small farm to grow tomatoes in KZN, so I will depend on the students that we produce over the next 9 years for my geriatric health care. This is the same time frame as the plan for full implementation of the NHI, with the NDP looking at 2030, the same as the Western Cape Health Department's vision. So what will the South African health system be like in 2025? Maybe if we can imagine it as clearly as possible, we could think what we need to do now in terms of educating the next generation. One of the students who will enroll as a medical student in January 2015, could be my doctor in 2025. She is preparing her application right now as we speak, making plans to write the National Benchmark Test ahead of submitting her application next month. I say "she" because for every male student we will admit 2 female students in 2015, in the absence of any admission policy that uses gender as a criterium. So let us call her "Sibongile", which means literally "we have given thanks". I hope this is prophetic in that I will be able to give thanks for her clinical competence and psychosocial approach when she looks after me in 2025, as a result of the education that she will receive in YOUR hands over the next 9 years. You see, in 2025, a year after she has completed her year of community service, she will 3 become my GP in the National Health Insurance system. Having grown up in rural KZN, she will return there in order to be closer to her family (but not too close). She will benefit from the extra points in the selection criteria as a result of being from a rural area, which is one of the few successful interventions that we can claim as being evidence-lead. I will also be heading back to rural KZN as a new retiree. Most of my current Discovery Health membership benefits will have been converted into the basic NHI package of services, and I will pay a much smaller premium for top-ups, which could include the services of a dentist, optician, and home-based care should I need them. As a retiree, the reduced premiums will be a welcome relief. When I sign on and am registered as a NHI patient at the clinic nearest to my tomato farm, all my chronic medications, primary care, and hospital admissions will be covered by the NHI. My only anxiety is the quality of the care that I will receive. Will it be adequate? Will there be an uninterrupted supply of the right drugs for me should I need them? Will the hospitals in rural KZN be adequately staffed and supervised? Will Sibongile, who has been assigned as the doctor to my local clinic, be not only adequately trained, but motivated to be an active part of this system, a leader even? Maybe I should increase my top-up medical aid just in case you all don't do a good enough job. Discovery will probably urge me to do so as I retire, with dire scenarios of inadequate coverage by the NHI. But no, I will trust the system, I will trust your efforts to educate Sibongile adequately, so that when I fall off my mountain bike and suffer a mild concussion (aged 66), she will make an appropriate clinical assessment and know what to do, a few months out of her community service. Most importantly, I hope she won't just send me home with Panado, but will take pains to check my GCS a few times over the next 24 hours and give my wife a check-sheet of danger signs. And I hope she won't patronize me, treating me as an imbecilic geriatric, even if I appear a bit groggy at first presentation. These thoughts pass through my mind as I construct the story and imagine the scenario. Hold that story - I'll come back to it. A small diversion (which is in the nature of stories) to tell you something about tomatoes, which has nothing at all to do with the education of health professionals, but everything to do with health. LYCOPENE, a carotenoid phytonutrient, is the most potent ANTIOXIDANT naturally 4 present in many fruits and vegetables. OXIDATIVE STRESS is mediated by highly reactive oxidant molecules that are generated endogenously through normal metabolic processes, life style activity and the diet. Antioxidants provide an effective means to combat the deleterious effects of oxidative stress and are increasingly being considered as strategic CHEMOPREVENTIVE AGENTS in the management of human diseases. Tomatoes and processed tomato products constitute the major source of dietary lycopene accounting for up to 85% of the daily intake. There is considerable scientific interest in the role of lycopene in the prevention of several degenerative diseases including CANCER, CORONARY HEART DISEASE and OSTEOPROSIS. So, once Tim Noakes' phase has passed and we have found a better balance between carbohydrates and fats in our diets, the age of lycopene will dawn on the public at large. And as a tomato grower I will be perfectly placed to supply the market with beautiful, tasty nutritious tomatoes, safe in the knowledge that I will be contributing to the better health of the population through the prevention of prostate cancer, hypertension, coronary heart disease, osteoporosis, and possibly even dementia. The principle of universal access demands that we not only provide access to a basic package of health services for every South African citizen, but that we be primarily concerned with keeping people healthy, and not just treating them when they become acutely or chronically ill. Our NHI doctors need to be part of a system of prevention and health promotion, and have a high level of skills to do this. Sibongile (may we give thanks) needs to talk to me not only about my diet (low carbs and lots of tomatoes), but also about my mountain biking habits, especially about wearing a helmet. And if I don't listen, either because of post-concussion syndrome or just because I refuse to be told what to do (others known as bloody-mindedness), I hope that she enlists the assistance of my wife, who is already working on a plan to transform my bloody-mindedness into mindfulness (another of the latest trends). But ultimately she should know that I will probably only take advice from my mates, so some appropriate health education on the prevention and effects of head injuries to the local mountain-biking club 5 would probably make the most impact. And maybe she should invite the local rugby club to the same event, and kill two birds with one stone. The problem is that transformation in sport is even slower than transformation in the health system, so we are still talking here about a bunch of white men in 2025. Whether all those beer-swilling white males will listen to a young black female doctor will be a test of the extent to which YOU have been successful in integrating her cultural competence with her clinical skills through the bio-psycho-social approach, in order to establish her credibility in the community that she is responsible for. Is this too far fetched? For those who don't like stories as much as Powerpoint, here are some bullet points about the NHI. (Bullets are such a military metaphor - like if you don't listen I will shoot you - with Powerpoint!) So I am going to extend the metaphor and shoot: The ABC of the NHI Constitution: Section 27 Social solidarity: not just health sector Universal coverage: population-based Pre-payment of costs: collective protection Pooling of insurance funds Sources of income Purchaser-provider split Benefits packages Primary level of care Civil society participation Legal perspectives Human resources for health A rapid review of the 11 pilot sites conducted in 2013 found: Uneven but significant progress in introducing NHI in the pilot districts Quality improvement teams and Facility Improvement Teams are having an impact Conditional grants have helped PHC Re-engineering strategies have been started but are not at full capacity 6 Pilot districts are ready for GPs in 1/3 of clinics Human resources for health remains a major challenge The basic idea of the NHI is to use the strengths and assets of the public sector, together with the strengths of the private sector, to create one large medical aid system to cater to the needs of all. Can this be done? Are there enough human resources? This is a graph of the absolute number of doctors over the past 100 years. It is my only graph, and my only look into the past. There are about 35000 doctors registered with the HPCSA who are not specialists, and another 10000 specialists, giving a total of 45000. These lines are likely to diverge further as the output of specialists remains linear, and the inclusion of Cuban-trained generalists accelerates the top line. Absolute Numbers of Registered Generalists vs Specialists in South Africa 1910-2009 7 It is worth looking at another country that has already travelled this path, to find out what our health system may look like in 2025. Brazil started on their transformation of the whole society with a new constitution in 1988, six years before our age of democracy dawned in South Africa. They created the SUS (Sistema Único de Saúde) in 1990, an equivalent of the NHI, with the aim of universal coverage, and so they have been at it for the past 24 years. We started in 2011, with a timeline of 14 years, so we have some catching up to do. If we look at Brazil vs South Africa, there are some striking differences and similarities: In 1994 they created the Programme Saude da Familia, or the Family Health System. Here is Dr Leonardo Targa, a GP in a small rural village in southern Brazil, whom we visited in his practice in Nova Petropolis in the province of Rio Grande do Sul, after a conference nearby that he helped to organise on rural health. Pinhal Alto is beautiful, hilly and forested, with productive small 8 farms in between, originally settled by German colonialists. Dr Targa met us at the entrance to his health centre and introduced us to his staff - a professional nurse, a nursing assistant, a pharmacy assistant, a clerk, a dental assistant as well as 5 community health agents. They are visited each week by different teams including a dietician, and a physiotherapist. He immediately lead us to this map of his area of responsibility. This Family Health team is responsible for the health of 2124 people, and Dr Targa is the only doctor - he has been their GP for the past 12 years. Every house was plotted and numbered on the map, and divided into sections, each of which was allocated to a community health agent like this one, Rejane, responsible for all the homes in white here. Another health agent looked after the red ones, and another the pink ones. They were particularly concerned about the health of these 3 9 families up here, which they regarded as at risk. It's difficult to see, but many of the houses have coloured pins, each indicating a different disease of a member of that family. The colour codes show that Rosa (red) pins indicate a pregnant woman, green for diabetics, orange for hypertensives, black (preto) for alcoholics and drug addicts, red (vermelho) for those on social grants or social risks, and white (branco) for serious mental illness. Each community health agent (along the top here: Cleonice, Rejane, Ivodia, Salete and Lucia) is responsible for the health of about 150 families, and they know exactly how many people have what conditions. Not many pregnancies, but a lot of hypertensives and mental illness. Currently (as of the 31st March) Dr Targa is concerned that they have a higher prevalence of hypertension than the provincial average, and a lower prevalence of diabetes than the 5% that is predicted. Are they missing the pre-diabetics in the community? Should 10 they be doing more active or more frequent screening, particularly in the families of known diabetics? These are the questions that worry him and his team. I am not unaware of the problems that Brazil faces 20 years since the PSF was begun. For example it has one of the highest caesarean birth rates in the world - upward of 50% nationally, and in private Brazilian hospitals it is even higher. There has been an increase in private health insurance in the last two decades as the Unified Health System has developed. But the significance of this case study is that here is a GP in a small rural community, in a practice that is clearly sustainable over the past 12 years, who is part of a well supported team that looks after the health of every single one of just over 2000 people. This is the primary health care approach in practice - it means health for all. This impressive primary care system has resulted in improvements in health outcomes that will ensure that Brazil meets the MDGs next year. It is population-based AND person-centred. There is science AND there is humanity: it is not a matter of one or the other. What would it take to produce health professionals - doctors, nurses, pharmacists, therapists, mid-level workers, community health workers - who are able to guide and lead primary health care teams like this, at scale across the country? What could or should we be doing over the next decade to feed skilled and reflexive graduates into this kind of system, motivated to make it work to the benefit of all the people in South Africa? Graduates like Sibongile (may we give thanks) who are prepared to construct it as they practice, to stick it out through the glitches and frustrations, providing leadership as well as technical expertise to the managers, clinicians and communities who need it? There is a tendency to lose one's sense of agency when we talk about health systems at a national level. The big picture tends to leave us all a bit disempowered, and it is easy to feel that it is someone else's problem, that the national minister must just pronounce, and it will happen. But like any leader all he can do is point in a general direction. Of all the members of an orchestra, the only one who does not produce a sound is the conductor. We are the ones 11 who have to make it happen, each in our own particular sphere of influence. Well as you heard yesterday, earlier this year a team of us lead by Ian Couper were faced with exactly this question, as consultants to NMMU in their plans to develop a new medical school there. We had to consider particularly what the Eastern Cape will need in 10 years' time, and propose a foundation for a new medical education programme ab initio. These were the broad principles on which we based our recommendations: Principles of Medical Education suggested for NMMU 1. Social accountability and community engagement • Social accountability • Community engagement • Primary Health Care • Systems understanding 12 2. Competent caring clinicians with broad skills • Community-based and distributed learning • Integration of theory and practice • A biopsychosocial model of health care • A person-centred approach 3. Excellence in educational practice • Interprofessional education • Transformative learning • Dedication to inquiry 4. Promotion of access and diversity • Active recruitment • Multiple entry and exit pathways • Accountability of students to community I think that these are the important components of education for the NHI. Taking the conference theme as a point of departure, I would like to suggest that there are two broad directions that we need to take, in dynamic tension. Let me polarise them in this way: training on the one hand, and education on the other. We need an outcomes-based approach as elucidated by Jason Frank, including a focus on competence, technical skills and evidence, which has a basis in a certain reductionism, and leads to specialisation. Technical competence is central, but it needs to be located in a system that serves all the people of this country, and not just a few, which is what the NHI is about. I would balance such training with education, competence with different ways of seeing, technical skills with the ability to apply them to individuals in unique ways. I would balance evidence with imagination, reductionism with context, and specialisation with holism. Brian O'Connell talked about ways of knowing: science and religion, and challenged us to write some stories that make sense of where we are going. Brazil shows us what is possible for a middle income country, and gives us an idea of the struggles that lie ahead. Minister Motsoaledi has started writing a story for the 13 health sector, and he needs help. As health educationalists, it CANNOT mean business as usual, and more of the same. It is clearly crazy to continue doing the same thing and expect a different result. We have to think, and plan, and teach, and learn in a different way to the past. Confined as many of us are to our hospitals and faculties and departments within faculties, our "community" is our students and our colleagues. Our task as health educationalists is to guide and motivate and inspire the next generation of health professionals, WHILE we are busy teaching the technical skills. The opposite of transformative education could be said to be reproductive education, in which we seek to replicate ourselves in our students. Transformative education means that we have to transform ourselves into pro-active role models as educators who locate ourselves in our future context. It means that our students do not imitate us, but must challenge us and surpass us, and establish new ways of practicing in the future health system. Their ready use of technology is a good example. We need to produce the next generation of health professionals who are not only excellent technicians, but also informed and activated intellectuals, aware of their power and position in society, and prepared to use it, as we build the health system for all. So finally, my story is at an end, some bullets to take home Universal access is everyone’s business: it is part of social solidarity We already have the resources to make it happen Context is more important in education than we assume Educate the graduate with the future health system in mind: “big picture” outcomesbased Training and Education in synergy Transformative learning begins with us Tomatoes, lycopene and mountain biking included, I hope that my stories have helped you to project our work as educationalists into the future, and as Brian Connell suggested, to make sense of the trajectory of our country. This is about a pedagogy of hope. 14 Because it is my story and I made it up, I am thinking of changing the name of my imagined protagonist - from Sibongile, to Sibusisiwe: "we have been blessed".