8 preparedness and action in emergency
advertisement

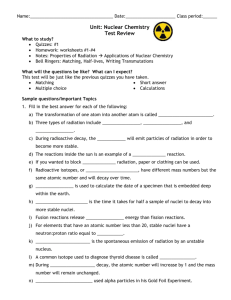
8. PREPAREDNESS AND ACTION IN EMERGENCY The requirements for protection of workers in emergency exposure situations are set out in the BSS [#502] and GSR Part 7 [#554]. Guidance on radiation protection of emergency workers and first responders are provided in Refs. [#563], [#501] and [#557]. The Table 8-1 presents four groups of workers to be exposed in an emergency exposure situation either due to their involvement in the emergency response or due to the nuclear or radiological emergency at a facility or an activity itself. Table 8-1. Exposure groups of workers in emergency exposure situation Group Definition A Emergency workers who have specified duties in response to a nuclear or radiological emergency; B Workers performing their duties at working places and being not involved in response to a nuclear or radiological emergency; C Workers who are asked to stop performing their duties at working places and to leave the site; D Workers who are accidently exposed as a result of an accident or incident at a facility or in an activity and whose exposure is not related to the emergency response. Considering the wide range of scenarios in a nuclear or radiological emergency and potential exposure to the above group of workers (such as designated emergency workers, administrative staff at the site, employees of nearby operational units etc.) an appropriate protection strategies should be applied. Protection of emergency workers specified in group A (as defined in Table 8-1) should be provided in line with the requirements set out in the BSS for emergency exposure situation and in GSR Part 7 [#554]. Protection of workers grouped in group B should be provided in the same way as for workers in planned exposure situation in line with the requirements set out in BSS [#502]. Protection of workers grouped in group C should be provided in the same way as for members of the public in emergency exposure situation in line with the requirements set out in GSR Part 7 [#554]. Protection of workers who are accidently exposed (group D) in relation to medical follow-up, treatment and dose assessment should be in line with BSS [#502] and in GSR Part 7[#554]. Protection of members of the public who willingly and voluntarily help in response to a nuclear or radiological emergency, i.e. helpers in an emergency, is not specifically addressed in this publication. However, they should be registered and integrated into the emergency response operations and provided with the same level of protection as for emergency workers not designated as such at preparedness stage in accordance with GSR Part 7 [#554]. 8.1. Emergency planning and responsibilities The Requirement 4 of the GSR Part 7 [#554] states that the identified hazards and potential consequences of an emergency shall provide a basis for establishing arrangements for preparedness and response for a nuclear or radiological emergency. The assessment of radiological hazards in the State provides the solid base for graded approach to developing 1 the emergency plans at all levels of emergency response. Concept of operation of emergency workers at scene of emergency is important element of emergency plan, which also describes the organizational structure, roles and responsibilities, means and principles for protecting the public and environment during an emergency. Development of concept of operation is the major stage of preparation of the emergency plans at all levels of response. Concept of operation is the general idea on how to act in case of realisation of particular facility-specific scenario of development of emergency situation on the site and off the site. Each scenario of exposure of emergency worker could be envisaged as a point in the threedimension system of emergency coordinates of 1. Emergency preparedness category (EPC), 2. Emergency class (EC), and 3. Emergency planning zone or distance (EPZ). Position in range of values of EPC-EC-EPZ fully defines the concept of operation in emergency as shown in Figure 8- 1. Operator Emergency class Government Emergency planning zone Emergency preparedness category Response organization Figure 8- 1. Concept of operation in the system of EPR coordinates. Concept of operation of emergency workers in event of radiation emergency should be developed at preparedness stage because of joint work of the government, operator of hazardous facility or practice, local authority, and response organization. The government at national or local level governs that work through coordinating authority defined in Ref. [#540] or through coordinating mechanism defined in Ref. [#554]. The emergency plan should include: (a) The persons or organizations responsible for ensuring compliance with requirements for protection and safety of workers in a nuclear or radiological emergency including those for controlling the exposure of emergency workers; (b) Defined roles and responsibilities of all workers involved in the response to a nuclear or radiological emergency; (c) Details on adequate self-protective actions to be taken, protective equipment and monitoring equipment to be used, and dosimetry arrangements in accordance with expected level of exposure and risk; (d) Consideration of access control for workers in a nuclear or radiological emergency on the site. 2 Table 8- 2. Emergency preparedness categories. E P C I II Description Criteria Facilities, for which on-site events (a), (b) (including those not considered in the design) are postulated that could give rise to severe deterministic effects off the site that warrant precautionary urgent protective actions, urgent or early protective actions and other response actions to meet the goals of emergency response in accordance with international standards, or for which such events have occurred in similar facilities. Facilities for which emergencies have been postulated that could result in severe deterministic health effects off-site, including: Reactors with power levels greater than 100 MW(thermal) (power, nuclear ship and research reactors); Facilities and/or locations with spent fuel pools that may contain some recently discharged irradiated reactor fuel with a total of more than about 0.1 EBq of Cs-137 (equivalent to the inventory in a 3000 MW(thermal) reactor core); Facilities with inventories of dispersible radioactive material with IDM (c) exceeding 10 000. Facilities for which emergencies have been postulated that could result in doses warranting urgent protective action being taken off-site, including: Reactors with power levels greater than 2 MW (thermal) and less than or equal to 100 MW (thermal) (power reactors, nuclear ship and research reactors); Facilities and/or locations containing recently discharged irradiated reactor fuel requiring active cooling; Facilities with inventories of dispersible radioactive material with IDM (c) in the range of 10 000 – 100 that is sufficient to result in doses warranting urgent protective action being taken off-site. Facilities, for which on-site events (a), (b) are postulated that could give rise to doses to people off the site that warrant urgent or early protective actions and other response actions to meet the goals of emergency response in accordance with international standards, or for which such events have occurred in similar facilities. Category II does not include facilities for which on-site events are postulated that could give rise to severe deterministic effects off the site, or for which such events have occurred in similar facilities. 3 E P C Description Criteria III Facilities, for which on-site events (b) are postulated that Facilities for which emergencies have been postulated that could result in could warrant protective action and other response doses warranting urgent protective action being taken on-site, including: actions to meet the goals of emergency response in Reactors with power levels of less than or equal to 2 MW (thermal); accordance with international standards on the site, or Facilities with inventories of radioactive material with IDM (c) in the range for which such events have occurred in similar of 100–0.01 that is sufficient to result in doses warranting urgent facilities. protective action being taken on-site. Facilities with radioactive sources in category 1 – 4 [#574], which activity Category III does not include facilities for which events exceeds 1/100 of D-values defined in Ref. [#512]. are postulated that could warrant urgent and early protective actions off the site, or for which such events have occurred in similar facilities. IV Activities and acts that could give rise to a nuclear or radiological emergency that could warrant protective actions and other response actions to meet the goals of emergency response in accordance with international standards in an unforeseen location. Category IV represents a level of hazard that applies for all States and jurisdictions. V Areas within emergency planning zones and distances (e) in a State for a facility in category I or II located in another State. These activities and acts include: (1) transport of nuclear or radioactive material and other authorized activities involving mobile dangerous sources (d) such as industrial radiography sources, nuclear powered satellites or radioisotope thermoelectric generators; and (2) theft of a dangerous source (d) and use of a radiological dispersal device or radiological exposure device. This category also includes: (i) detection of elevated radiation levels of unknown origin or commodities with contamination; (ii) identification of medical symptoms due to radiation overexposure; and (iii) transnational emergency as a result of a nuclear or radiological emergency abroad that is not a category V. EPC I facilities in neighbouring country nearer than 50-300 km from national border, or EPC II facilities nearer than 5-50 km from national border (a) Involving release of radioactive material, or external exposure that originates from a location on the site. (b) Such events include nuclear security events. 4 (c) IDM is an index of dispersible radioactive material inventory equal to sum of ratios of activity of all stored radionuclides to corresponding D2 value characterizing its radiotoxicity in dispersed form, as defined in Ref. [#512]. (d) Dangerous are the radionuclide sources in category 1-3 [#574], which activity exceeds D-values defined in Ref. [#512]. (e) Default sizes of emergency planning zones and distances are given in Table 8- 4. 5 Emergency preparedness categories Arrangements for the protection of workers in a nuclear or radiological emergency should be a part of the emergency plan based on the assessment of Emergency Preparedness Category (EPC) of the facility or the area in accordance with international requirements in GSR Part 7 [#554]. The five emergency preparedness categories (hereinafter referred to as ‘categories’) establish the basis for a graded approach to be applied for developing generically justified and optimized arrangements for preparedness and response for a nuclear or radiological emergency. The degree of planning should be commensurate with the nature and magnitude of the risk and the feasibility of mitigating the consequences should an emergency occur. Emergency Preparedness Categories (EPC) shown in Table 8- 2 combine assessed hazards for the purposes of the international requirements. This table is a combination of Table III and Table A5-II from [#571].The table provides suggested criteria from [#576] for determining emergency preparedness categories for facilities and practices. Emergency classes Requirements and guidance for emergency response are specified in the international requirements in Ref. [#554] for five classes of emergency, which are the follows. i. General emergencies at facilities in EPC I or II for an emergency that warrants taking precautionary urgent protective actions, urgent protective actions and other response actions on the site and off the site. ii. Site area emergencies at facilities in EPC I or II for an emergency that warrants taking protective actions and other response actions on the site and in the vicinity of the site. iii. Facility emergencies at facilities in EPC I, II or III for an emergency that warrants taking protective actions and other response actions at the facility and on the site but does not warrant taking protective actions off the site. Emergencies in this class do not present an off-site hazard. iv. Alerts at facilities in EPC I, II or III for an event that warrants taking actions to assess and to mitigate the consequences at the facility. v. Other nuclear or radiological emergencies for emergencies in EPC IV or V that warrant taking protective actions and other response actions at any location. It is required that the operator of EPC I, II or III facility is responsible for declaration of the emergency and its’ classification. The class of emergency when declared, defines in general the protective and other actions which have to be undertaken by the emergency workers. The international requirements in Ref. [#554] provide that relationship as follows. 1. Upon declaration of General emergency, appropriate actions shall promptly be taken, according to the available information relating to the emergency: (a) to mitigate the consequences of the emergency on the site and (b) to protect workers in group B, C and D from Table 8-1 and visitors on the site and people off the site. 2. Upon declaration of Site emergency, actions shall promptly be taken: (a) to mitigate the consequences of the emergency on the site and to protect workers in group B, C and D from Table 8-1 and visitors on the site, (b) to increase the readiness to take protective actions and other response actions off the site if this becomes necessary on the basis of observable conditions, reliable assessments and/or monitoring results, and (c) to conduct monitoring and sampling off the site. 3. Upon declaration of Facility emergency, actions shall promptly be taken: (a) to mitigate the consequences of the emergency and 6 (b) to protect workers in group B, C and D from Table 8-1 and visitors on the site. 4. Upon declaration of Alert, actions shall promptly be taken (a) to assess and to mitigate the consequences of the event and (b) to increase the readiness of the on-site response organizations. 5. Upon declaration of other nuclear or radiological emergencies and the level of emergency response, actions shall promptly be taken: (a) to mitigate the consequences of the emergency on the site, to protect those in the vicinity (e.g. the public, workers, emergency workers) and (b) to determine where and for whom protective actions and other response actions are warranted. Emergency planning zones or distances On the site area of facilities in EPC I, II, or III requires special attention for planning emergency response on the site: to protect workers in group B and D from Table 8-1 and visitors on the site, to prevent development of the catastrophic conditions on the site, to prevent the severe release off the site, to provide the mitigatory and recovery actions on the site to regain the control over the source. The doses of emergency exposure of emergency workers on the site of the facilities in EPC I, II, or III could exceed the threshold levels of development the severe deterministic effects given in [#554], [#501] and presented in Table 8- 3. The emergency response teams of the facility or off-site specialised response organizations form the group of emergency workers performing the tasks on the site. As the rule those tasks are conducted in the most risky and hazardous conditions. Table 8- 3. Criteria for preventing or minimizing severe deterministic effects. Dose quantity Dose criterion External acute exposure (<10 h) AD Re d marrow (a) 1 Gy AD Foetus AD Tussue AD Skin 0.1 Gy (b) 25 Gy at 0.5 cm (c) 10 Gy to 100 cm2 Internal exposure from acute intake (Δ = 30 d)d AD ( ) Re d marrow (d) 0.2 Gy for radionuclides with Z>90 (e) 2 Gy for radionuclides with Z<89 (e) AD() Thyroid 2 Gy AD ( ) Lung 30 Gy AD() Colon 20 Gy 7 AD() Foetus (a) (g) 0.1 Gy AD Re d marrow represents the RBE weighted dose to internal tissues or organs (e.g. red marrow, lung, small intestine, gonads, thyroid) and to the lens of the eye from exposure in a uniform field of strongly penetrating radiation. (b) Dose delivered to 100 cm2 at a depth of 0.5 cm under the body surface in tissue due to close contact with a radioactive source (e.g. source carried in the hand or pocket). (c) The dose is to the 100 cm2 dermis (skin structures at a depth of 40 mg/cm2 (or 0.4 mm) below the body surface). AD() T is the RBE weighted dose in organ or tissue T delivered over the period of time Δ by the intake of radioactive material that will result in a severe deterministic effect in 5% of exposed individuals. (d) (e) Different criteria are used to take account of the significant difference in the radionuclide specific intake threshold values for the radionuclides in these groups. For the purposes of these generic criteria, ‘lung’ means the alveolar-interstitial region of the respiratory tract. (f) (g) For this particular case, means the period of in utero development. The international requirements in Ref. [#554] are that, off-site of facilities in category I or II, arrangements are required to be made for effectively making and implementing decisions on urgent protective actions within the following emergency planning zones or distances. i. A precautionary action zone (PAZ), for facilities in category I, for which arrangements shall be made to take urgent protective actions and other response actions, before any significant release of radioactive material occurs, in order to avoid or to minimize severe deterministic effects. ii. An urgent protective action planning zone (UPZ), for facilities in category I or II, for which arrangements shall be made to initiate urgent protective actions and other response actions, if possible before a significant release of radioactive material occurs or after release occurs in order to reduce the risk of stochastic effects. iii. An extended planning distance (EPD) from the facility, for facilities in category I or II, is the area beyond the UPZ for which arrangements shall be made to conduct monitoring and assessment of the radiological situation off the site in order to identify areas within a period of time that would allow reducing the risk of stochastic effects effectively by taking: (a) urgent protective actions and other response actions within a day following a significant release and (b) early protective actions and other response actions within a week to a month following a significant release. iv. An ingestion and commodities planning distance (ICPD) from the facility, for facilities in category I or II, is the area beyond the EPD for which arrangements shall be made to take response actions (a) to protect the food chain and water supply systems as well as commodities other than food from contamination following a significant release and (b) to protect the public from ingestion of food, milk and drinking water and from use of commodities other than food that may be contaminated following a significant release. Suggested dimensions of these zones for facilities in EPC I, II and III are defined in Ref. [4] and presented in Table 8- 4. As a rule, the emergency zones for nuclear installation are 8 established with account of the potential for radiological consequences for people off the site and the feasibility of implementing emergency plans, and of any external events or phenomena that may hinder its implementation. Table 8- 4. Suggested emergency zones and area sizes for nuclear installations and facilities with dispersible radioactive material. Facilities PAZ, km UPZ, km EPD, km ICPD, km 100 300 50 100 Reactor facility Power higher than 1000 MW (th) Power from 100 to 1000 MW (th) 3–5 15 - 30 Power from 10 to 100 MW (th) None 0.5–5 2 – 25 5 – 50 Power from 2 to 10 MW (th) None 0.5 1–2 2–5 Power lower than 2 MW (th) None None None None Facility with dispersible radioactive material 105 ≤ IDM (a) 300 50 100 0.5–5 2 – 25 5 – 50 0.5 1–2 2–5 15 - 30 103≤ IDM <104 None 102≤ IDM <103 None 104≤ IDM <105 (a) 100 3–5 IDM < 100 None None None None IDM is an index of dispersible radioactive material inventory equal to sum of ratios of activity of all stored radionuclides to corresponding D2 value characterizing its radiotoxicity in dispersed form, as defined in Ref. [#512]. In response to nuclear emergencies in EPC I and II the arrangements for protection of the emergency workers should take into account that The doses of emergency workers performing the transitory tasks in PAZ could exceed the threshold levels of development the severe deterministic effects given in Table 8- 3; The doses of emergency workers performing the transitory tasks in UPZ but beyond the PAZ unlikely could exceed the threshold levels of development the severe deterministic effects given in Table 8- 3. Nevertheless, the daily effective dose of emergency workers performing lasting tasks in UPZ could exceed 10 mSv/d; The daily effective dose of emergency workers performing lasting tasks in EPD unlikely could exceed 10 mSv/d; The daily effective dose of emergency workers performing lasting tasks in ICPD unlikely could exceed 1 mSv/d. In response to radiological emergencies in EPC III and IV the arrangements have to be at place for establishing safety perimeter of inner cordoned area around the scene of event. That inner cordoned area should cover the territory with ambient dose rate of 100 µSv/h at 1 m above the ground surface. The access of emergency workers (first responders) to that territory should be controlled and limited in line with guidance in Ref. [#563]. Expected size of such areas depends on the nature of event as given in Table 8- 5. 9 Table 8- 5. Suggested radius of inner cordoned area (safety perimeter) for a radiological emergency. Radius of inner cordoned Situation area Initial determination - outside Unshielded or damaged potentially dangerous source 30 m around Major spill from a potentially dangerous source 100 m around Fire, explosion or fumes involving a potentially dangerous source 300 m radius Suspected bomb (potential RDD (a)) exploded or unexploded 400m radius or more to protect against the second explosion Initial determination - inside a building Damage, loss of shielding or spill involving a potentially dangerous source Affected and adjacent areas (including floors above and below) Fires, suspected RDD or other event involving a potentially dangerous source that can spread materials in the building Entire building and appropriate outside distance indicated (a) Radiological dispersal device (dirty bomb). The scene of emergency in EPC IV could has the heterogeneous contamination with “hot spots” inside the safety perimeter. It has to be taken into account that doses of emergency workers performing the transitory tasks in “hot spots” could exceed the threshold levels of development the severe deterministic effects given in Table 8- 3. The areas in EPC V are similar to these in EPC I or II. It is unlikely that this area will include the extension of PZA of the NPP in neighbouring State. Therefore The doses of emergency workers performing the transitory tasks in extension of UPZ but beyond the PAZ unlikely could exceed the threshold levels of development the severe deterministic effects given in Table 8- 3. Nevertheless, the daily effective dose of emergency workers performing lasting tasks in UPZ could exceed 10 mSv/d; The daily effective dose of emergency workers performing lasting tasks in extension of EPD unlikely could exceed 10 mSv/d; The daily effective dose of emergency workers performing lasting tasks in extension of ICPD unlikely could exceed 1 mSv/d. Summary of expected levels of health risks for emergency workers Table 8- 6 presents the summary of expected levels of health risks for emergency workers in different emergency preparedness categories. Criterion of developing the severe deterministic effect is exceeding the dose levels in Table 8- 3. Criterion of developing the stochastic effect is exceeding the dose level of detectability of stochastic effects which for external exposure is equal to 100 mSv of effective dose [#531], [#577], [#578]. 10 Table 8- 6. Expected health effects for EPC. E P C I I I Health risk Category of exposed persons Deterministic Stochastic On-site emergency workers and staff of the facility Likely Likely Off-site emergency workers Likely Likely On-site emergency workers and staff of the facility Likely Likely Off-site emergency workers I I I On-site emergency workers and staff of the facility I V First responders and emergency workers V Emergency workers Unlikely Likely Off-site emergency workers Likely Likely Unlikely Likely Unlikely Likely Unlikely Likely 8.2. Protection of emergency workers The fundamental difference between members of the public and emergency workers in an emergency exposure situation is that members of the public may receive doses unless some action is taken to prevent them, whereas emergency workers will receive doses due to specified duties assigned to them. Thus, to the extent possible, it is reasonable to continue to treat emergency workers’ exposures according to the requirements for planned exposure situations, in accordance with the graded approach, particularly in the later stages of the emergency exposure situation. The exposure of emergency workers starts with the assignment to undertake a particular action and finishes with completion of the assigned task or declaration of termination of the emergency. Protection of emergency workers should include, as a minimum; (a) (b) (c) (d) (e) (f) Training of emergency workers designated as such in advance; Providing instructions immediately before their use to those emergency workers not designated as such in advance1 on how to perform their specified duties under emergency conditions and how to protect themselves (‘just in time training’); Managing, controlling and recording the doses received; Provision of appropriate specialized protective equipment and monitoring equipment; Medical follow-up and psychological counselling, as appropriate; Obtaining informed consent to perform specified duties, when appropriate. Justification At the preparedness stage, the protective actions and other response actions to be taken in a nuclear or radiological emergency should be justified. Due consideration should be given to the detriment associated with doses received by the emergency workers implementing those 1 Emergency workers who are not designated as such at preparedness stage should be registered and integrated in into the emergency response operations in line with GSR Part 7 [#554] 11 actions. There should be a commitment to the justification process by all stakeholders (regulatory body, response organizations and interested parties). Optimization At the preparedness stage, the process of optimization, including the use of reference levels, should be applied to the protection of workers as well. There should be a commitment to the optimization process by all stakeholders (regulatory body, response organizations and interested parties). As part of the process of optimization, reference levels should be established. A reference level should represent the level of dose above which it is judged to be inappropriate to plan to allow exposures to occur and for which protective actions should therefore be planned and optimized. The doses to be compared with the reference levels are usually prospective doses, i.e. doses that may be received in the future, as it is only those doses that can be influenced by decisions on protective actions. They are not intended as a form of retrospective dose limit. The initial phase of a response to a nuclear or radiological emergency is characterized by a lack of information about the event and the need for urgency in implementing protective actions with involvement of emergency workers. Therefore, there is little or no scope for applying the optimization process when managing the protection of emergency workers during this initial phase of response. Efforts should be aimed at reducing any exposures as far as practicable taking into account the difficult conditions of the evolving emergency. When implementing protective actions during the late phase of a nuclear or radiological emergency and at the transition from an emergency exposure situation to an existing exposure situation, the optimization process should be applied to the protection of emergency workers in the same way as for workers in planned exposure situations. Restricting exposure of emergency workers Because the exposure of emergency workers is deliberate and controlled, the dose limits for workers should be assumed to apply unless there are overriding reasons not to apply them. In terms of para. 4.15 of the BSS and GSR Part 7 [#554], response organizations and employers have to ensure that no emergency worker is subject to an exposure in an emergency in excess of 50 mSv other than: (a) (b) (c) For the purposes of saving life or preventing serious injury; When undertaking actions to prevent severe deterministic effects and actions to prevent the development of catastrophic conditions that could significantly affect people and the environment; or When undertaking actions to avert a large collective dose. Reference levels expressed as guidance values for restricting the exposure of emergency workers should be defined in accordance with the assigned task as provided in Table 8- 7 [#554]. Where lifesaving actions are concerned, every effort should be made to keep individual doses of emergency workers below 500 mSv for exposure to external penetrating radiation, while other types of exposure need to be prevented by all possible means. However, while estimating dose to emergency workers, the exposure from all pathways, external and internal, should be assessed and included in the total. The value of 500 mSv should be exceeded only under circumstances in which the expected benefits to others clearly outweigh the emergency worker’s own health risks, and the emergency worker volunteers to take the action and understands and accepts this health risk. Table 8- 7. Guidance values for restricting exposure of emergency workers Tasks Guidance value 12 H P (10) (a) < 500 mSv Life saving actions and E (b) < 500 mSv, and 1 AD T (c) < AD T contained in Table 8- 3 2 This value may be exceeded with due consideration of the generic criteria in Table 8- 3 under circumstances in which the expected benefits to others clearly outweigh the emergency worker’s own health risks, and the emergency worker volunteers to take the action and understands and accepts this health risk. Actions to prevent severe deterministic effects and actions to prevent the development of catastrophic conditions that could significantly affect people and the environment H P (10) (a)< 500 mSv and E (b) < 500 mSv, and 1 AD T (c) < AD T contained in Table 8- 3 2 H P (10) (a)< 100 mSv Actions to avert a large collective dose and E (b) < 100 mSv, and 1 AD T (c) < AD T contained in Table 8- 3 10 (a). Personal dose equivalent H P (d) where d = 10 mm. For more details see Section 3. (b). Effective dose. For more details see Section 3. (c).. RBE weighted absorbed dose to an organ or tissue. For more details see Section 3. Regardless of the circumstances, response organizations and employers should make all reasonable efforts to keep the doses received by emergency workers below the values given in Table 8- 3 in order to prevent or minimize severe deterministic effects [#501]. 8.3. Managing the exposure of emergency workers In terms of para. 4.12 of the BSS [#502], the government needs to establish a programme for managing, controlling and recording the doses received by emergency workers in a nuclear or radiological emergency. Response organizations and employers should implement this programme. The group of emergency workers specified in group A in Table 8-1 may be further divided into three categories of emergency worker and may be defined: (a) Category 1: Emergency workers undertaking mitigatory actions and urgent protective actions on the site — include life-saving actions or to prevent serious injury or actions to prevent development of catastrophic conditions that could significantly affect 13 people and the environment, actions to prevent serious deterministic effects and actions to avert large collective dose. Emergency workers in this category have to be designated as such at preparedness stage. They are most likely to be operating personnel at the facility or activity, but may also be personnel from emergency services. They are employed either by a registrant or licensee (operating organization), or by a response organization, and will have received training in occupational radiation protection. (b) Category 2: Emergency workers undertaking urgent protective actions off the site to avert a large collective dose (for example, evacuation, sheltering, radiation monitoring etc.). They are most likely to be police, fire fighters, medical personnel, and drivers and crews of evacuation vehicles. Every effort should be made to designate emergency workers in this category as such at preparedness stage. They are to have predefined duties in an emergency response and should receive training in occupational radiation protection as first responders on a regular basis. They are not normally regarded as occupationally exposed to radiation and their employers are response organizations. (c) Category 3: Emergency workers undertaking early protective actions and other response actions off the site (for example, relocation, decontamination, environmental monitoring etc.) as well as other actions aimed to enable the termination of the emergency. Emergency workers in this category may or may not be designated as such at preparedness stage. They may or may not normally be regarded as occupationally exposed to radiation and may or may not have received any relevant training. Any limit in duration of work undertaken by emergency workers and conditions by which they will conduct the work should be implemented by planning the emergency work driven by dose guidance values. Tasks should be assigned depending on the category of emergency worker as follows: (a) Category 1 emergency workers should carry out actions to save life or prevent serious injury and actions to prevent severe deterministic effects and actions to prevent the development of catastrophic conditions that could significantly affect people and the environment; (b) Category 2 emergency workers should not be the first choice for taking lifesaving actions; (c) Category 1 and Category 2 emergency workers should carry out actions to avert a large collective dose2. (d) Category 3 emergency workers should carry out those actions in which they will not receive a dose of more than 50 mSv. Female workers who are aware that they are pregnant or breast-feeding should, in order to provide adequate protection for the embryo or foetus, notify the appropriate authority and should be excluded from emergency tasks listed in Table 8- 7 and or the infant are afforded the level of protection as required for members of the public (para 3.114 of the BSS [#502] and para I.4 of the GSR Part 7 [#554]). Emergency workers who undertake actions in which the doses received might exceed 50 mSv do so voluntarily and should have been clearly and comprehensively informed in advance of the associated health risks, as well as of available protective measures, and should be trained, to the extent possible, in the actions they are required to take. The 2 Helpers in an emergency should not be allowed to take actions that might result in their exceeding the guidance values of dose for taking actions to avert large collective dose given in Table 8- 7. 14 voluntary basis for response actions by emergency workers is usually covered in the emergency arrangements. In almost all emergencies, at best only the dose from external penetrating radiation will be measured continuously. Consequently, the operational guidance provided to emergency workers should be based on measurements of penetrating radiation (e.g. as displayed on an active or self-reading dosimeter). The dose from intakes, skin contamination and exposure of the lens of the eye should be prevented by all possible means for instance by the use of protective equipment, iodine thyroid blocking (where exposure to radioactive iodine might be involved) and the provision of instructions concerning operations in potentially hazardous radiological conditions. Such instructions should cover the application of time, distance and shielding principles, the prevention of ingestion of radioactive material and the use of respiratory protection. Available information about radiation conditions on the site should be used in aiding decisions on the appropriate protection of emergency workers. 8.4. Exposure assessment Response organizations and employers should take all reasonable steps to assess and record the exposures received by workers in an emergency. Once the total dose of emergency workers from all exposure pathways (including committed dose from intake) has been estimated, the Table $08-02 also provides guidance for the effective dose and equivalent dose to an organ or tissue for restricting further exposure in response to a nuclear or radiological emergency. The exposures of emergency workers in an emergency response and of workers who are accidently exposed should, if possible, be recorded separately from those incurred during routine work, but should be noted on the workers’ records of occupational exposure. The degree of accuracy required for any exposure assessment should increase with the level of exposure likely to have been received by the worker. Some pre-established guidance may help in the management of exposures of emergency workers in Category 1, expressed in terms of dose and directly measurable quantities such as dose rate or air concentration. The exposures of emergency workers should be monitored on an individual basis, using means appropriate to the situation, such as direct reading or alarm dosimeters. Records of occupational exposure should be generated and maintained in a simplified standard format by all response organizations and employers to avoid confusion. The information on the doses received and the associated health risks should be communicated to the emergency workers involved. Workers should not normally be precluded from incurring further occupational exposure because of doses received in an emergency exposure situation. More detailed guidance on exposure assessment in emergencies is given in section 7 and in paras 7.2287.243 of Ref. [#557]. 8.5. Medical attention Emergency workers and accidentally exposed employees should receive medical attention appropriate for the dose they may have received. Screening based on equivalent doses to specific radiosensitive organs as a basis for medical follow-up and counselling should be provided if an emergency worker or accidentally exposed employee has received an effective dose of 100 mSv over a period of a month or if the worker so requests. Screening based on equivalent doses to specific radiosensitive organs given in Table 8- 3 should be used as a basis for immediate medical examination, consultation and indicated medical treatment in accordance with GSR Part 7 [#554]. Emergency worker or accidentally exposed employee who receives doses in nuclear or radiological emergency should normally not be precluded from incurring further occupational exposure. However, qualified medical advice should be obtained before any further occupational exposure if an 15 emergency worker or accidentally exposed employee has received an effective dose exceeding 200 mSv or at the request of the worker. A particular concern should be whether a worker has received a dose sufficient to cause serious deterministic effects. If the dose received by the worker exceeds the criteria given in Table $08-03, protective actions and other response actions should be taken in accordance with GSR Part 7. Such actions may include: (a) Performing immediate medical examination, consultation and indicated treatment; (b) Carrying out contamination control; (c) Carrying out immediate decorporation3 (if applicable); (d) Carrying out registration for long term health monitoring (medical follow-up); (e) Providing comprehensive psychological counselling. Additional information related to medical response to emergencies can be found in Refs [#501], [#555], [#556]. 3 Decorporation is the biological processes, facilitated by a chemical or biological agent, by which incorporated radionuclides are removed from the human body. 16 REFERENCES [#501] FOOD AND AGRICULTURE ORGANIZATION OF THE UNITED NATIONS, INTERNATIONAL ATOMIC ENERGY AGENCY, INTERNATIONAL LABOUR ORGANIZATION, PAN AMERICAN HEALTH ORGANIZATION, WORLD HEALTH ORGANIZATION, Criteria for Use in Preparedness and Response for a Nuclear or Radiological Emergency, IAEA Safety Standards Series No. GSG-2, IAEA, Vienna (2011). [#502] INTERNATIONAL ATOMIC ENERGY AGENCY, Radiation Protection and Safety of Radiation Sources: International Basic Safety Standards. Interim edition, General Safety Requirements Part 3, Safety Standard Series No. GSR Part 3 (Interim), IAEA, Vienna (2011). [#503] INTERNATIONAL ATOMIC ENERGY AGENCY, The Radiological Accident in Samut Prakarn, IAEA, 2002 [#504] INTERNATIONAL ATOMIC ENERGY AGENCY, INTERNATIONAL LABOUR ORGANIZATION, WORLD HEALTH ORGANIZATION, Approaches to attribution of detrimental health effects to occupational ionizing radiation exposure and their application in compensation programmes for cancer: A practical guide / edited by Shengli Niu, Pascal Deboodt, Hajo Zeeb. Occupational Safety and Health Series, No. 73, Geneva, ILO, 2010 [#505] Cerveny T. J., MacVittie T. J., and Young, R. W., Acute radiation syndrome in humans In: Walker RI, Cerveny TJ (edsz.) Medical Consequences of Nuclear Warfare, Part I, Vol. 2. In: Zajtchuk R, Jenkins DP, Bellamy RF, Ingram VM (eds.) Textbook of Military Medicine. Falls Church, VA: Office of the Surgeon General, Department of the Army, USA, 1989, 17-36. [#506] Biodosimetry Assessment Tool (BAT) Version 0.7.5 Beta, Rev. A 23 May 2002. Armed Forces Radiobiology Research Institute, Bethesda, MD, USA. [#507] U.S. DEPARTMENT OF HOMELAND SECURITY, Dirty Bombs. Radiological Dispersal Device (RDD) Dirty Bomb Medical Preparedness and Response: Guidance for First Responders and Health Care Workers - Radioactive Illnesses, Radiation Injuries, Decontamination, U.S. Department of Homeland Security, 2011. [#508] Gus'kova A.K., Nadezhina N.M., Barabanova A.V., Baranov A.E., Gusev I.A., Protasova T.G., Boguslavskij V.B. and Pokrovskaya V.N., Acute effects of radiation exposure following the Chernobyl accident: immediate results of radiation sickness and outcome of treatment. In Medical aspects of the Chernobyl accident (Proceedings of the conference in Kiev 11-13 May, 1988). Vienna: IAEA; Technical Document Series No 516: 233-256; 1989. [#509] INTERNATIONAL ATOMIC ENERGY AGENCY, Lessons Learned from the Response to Radiation Emergencies (1945-2010), Emergency Preparedness and Response Series EPR-LESSONS LEARNED, IAEA, Vienna (2012) [#510] Abrahamson, S., Bender, M.A., Boecker, B.B., Gilbert, E.S. and Scott, B.R. Health Effects Models for Nuclear Power Accident Consequence Analysis. Modification of Models Resulting From Addition of Effects of Exposure to Alpha-Emitting Radionuclides. Part II: Scientific Bases for Health Effects Models. NUREG/CR-4214 Rev. 1, Part II Addendum 2 LFM-136 (1993). 17 [#511] INTERNATIONAL ATOMIC ENERGY AGENCY, WORLD HEALTH ORGANIZATION, Development of extended framework for emergency response criteria Interim guidance for comments. IAEATECDOC-1432, IAEA, Vienna (2005). [#512] INTERNATIONAL ATOMIC ENERGY AGENCY, Dangerous Quantities of Radioactive Material, Emergency Preparedness and Response Series EPR-D-VALUES, IAEA, Vienna (2006). [#513] Reassessment of the Atomic Bomb Radiation Dosimetry for Hiroshima and Nagasaki – Dosimetry System 2002. Radiation Effects Research Foundation, 2005. [#514] A long-term cohort study on the A-bomb survivors of Hiroshima and Nagasaki, recent results and a future scope. Toshiteru Okubo, Chairman of Radiation Effects Research Foundation, Hiroshima and Nagasaki, Japan. Materials presented in the IAEA. October 2009. [#515] INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION, Recommendations of the International Commission on Radiological Protection. ICRP Publication 26. Ann ICRP Vol 1, No 3 (1977). [#516] Libmann J. Elements of nuclear safety. IPSN, Paris (1996). [#517] UNITED NATIONS SCIENTIFIC COMMITTEE ON THE EFFECTS OF ATOMIC RADIATION. Sources and Effects of Ionizing Radiation. UNSCEAR 2006 Report to the General Assembly with Scientific Annexes. Annex A. Epidemiological studies of radiation and cancer. New York, United Nations (2006). [#518] González A.J. The radiological health consequences of Chernobyl: the dilemma of causation. Symposium on Nuclear Accidents. In: Nuclear accidents: Liabilities and guarantees: Proceedings of the Helsinki symposium, OECD Nuclear Energy Agency (1993). [#519] UNITED NATIONS SCIENTIFIC COMMITTEE ON THE EFFECTS OF ATOMIC RADIATION. Sources and Effects of Ionizing Radiation. UNSCEAR 2000 Report to the General Assembly with Scientific Annexes. Annex G. Biological effects at low radiation doses. New York, United Nations (2000). [#520] UNITED NATIONS SCIENTIFIC COMMITTEE ON THE EFFECTS OF ATOMIC RADIATION, Sources and Effects of Ionizing Radiation. UNSCEAR 2010 Report to the General Assembly. New York, United Nations (2011). [#521] UNITED NATIONS SCIENTIFIC COMMITTEE ON THE EFFECTS OF ATOMIC RADIATION, Sources and Effects of Ionizing Radiation. UNSCEAR 2012 Report to the General Assembly, New York, United Nations (2012). [#522] INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION, The 2007 Recommendations of the International Commission on Radiological Protection. ICRP Publication 103, Ann ICRP 37(2-4), Elsevier (2007). [#523] INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION, Recommendations of the International Commission on Radiological Protection. ICRP Publication 26, Ann ICRP 1(3), Pergamon Press, Oxford, UK (1977). [#530] KUTKOV V., BUGLOVA E., and MCKENNA T. Severe deterministic effects of external exposure and intake of radioactive material: basis for emergency response criteria, J. Radiol. Prot. 31, 237–253 (2011). [#531] INTERNATIONAL ATOMIC ENERGY AGENCY, Actions to Protect the Public in an Emergency due to Severe Conditions at a Light Water Reactor, Emergency Preparedness 18 and Response Series EPR-NPP PUBLIC PROTECTIVE ACTIONS, IAEA, Vienna (2013). [#532] MCKENNA T., KUTKOV V., VILAR WELTER P., DODD B., and BUGLOVA E. Default operational intervention levels (OILs) for severe nuclear power plant or spent fuel pool emergencies. Health Phys. 104 (2013) 459-470. [#533] U.S. NATIONAL ACADEMIES/NATIONAL RESEARCH COUNCIL, Health effects of exposure to low levels of ionizing radiation, BEIR V, National Academy Press, Washington. D.C. (1996) [#534] INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION, Pregnancy and Medical Radiation. ICRP Publication 84. Ann ICRP Vol. 30 No. 1, Pergamon Press, Oxford, UK (2000). [#535] UNITED NATIONS SCIENTIFIC COMMITTEE ON THE EFFECTS OF ATOMIC RADIATION, Sources and effects of ionizing radiation. UNSCEAR 1993 Report to the General Assembly with Scientific Annexes. Annex G. Hereditary effects of radiation, New York, United Nations (1993). [#536] KUTKOV V. A., DEMIN V. F. and GOLIKOV V. Ya., Standardization for ionizing radiation, Atomic Energy 85(2), 589-594, New York: Springer (1998). [#537] INTERNATIONAL NUCLEAR SAFETY ADVISORY GROUP, Defence in Depth in Nuclear Safety, INSAG-10, IAEA, Vienna (1996). [#538] KUTKOV V., KOCHETKOV O. and PANFILOV A., Strategy of control at source as a base for protecting workers against risks arising from exposure to ionizing radiation in the Russian Federation. In: Occupational Radiation Protection: Protecting Workers against Exposure to Ionizing Radiation, Int. Conf., 26-30 August 2002, Geneva, Switzerland, IAEA-CN-91/126, 39 – 44, CD-ROM Contr. Papers, Vienna, IAEA, (2003). [#539] UNITED NATIONS SCIENTIFIC COMMITTEE ON THE EFFECTS OF ATOMIC RADIATION. Sources and effects of ionizing radiation. UNSCEAR 2000 Report to the General Assembly with Scientific Annexes. Annex B. Exposures from natural radiation sources, New York, United Nations (2000). [#540] FOOD AND AGRICULTURE ORGANIZATION OF THE UNITED NATIONS, INTERNATIONAL ATOMIC ENERGY AGENCY, INTERNATIONAL LABOUR ORGANIZATION, OECD NUCLEAR ENERGY AGENCY, PAN AMERICAN HEALTH ORGANIZATION, UNITED NATIONS OFFICE FOR THE COORDINATION OF HUMANITARIAN AFFAIRS, WORLD HEALTH ORGANIZATION, Preparedness and Response for a Nuclear or Radiological Emergency, IAEA Safety Standards Series No. GS-R-2, IAEA, Vienna (2002). [#541] U.S. NATIONAL COUNCIL ON RADIATION PROTECTION AND MEASUREMENTS, Considerations regarding the unintended radiation exposure of the embryo, foetus or nursing child, NCRP Commentary 9, Bethesda, NCRP (1994). [#542] U.S. NATIONAL COUNCIL ON RADIATION PROTECTION AND MEASUREMENTS, Potential impact of individual genetic susceptibility and previous radiation exposure on radiation risk for astronauts, NCRP Report 167, Bethesda, NCRP (2010). [#543] INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION, Biological Effects after Prenatal Irradiation (Embryo and Fetus), ICRP Publication 90, Ann ICRP Vol. 33(1-2), Pergamon Press, Oxford, UK (2003). 19 [#544] U.S. NATIONAL COUNCIL ON RADIATION PROTECTION AND MEASUREMENTS, Uncertainties in the Estimation of Radiation Risks and Probability of Disease Causation, NCRP Report 171, Bethesda, NCRP (2012). [#545] DOUPLE et al., Long-term radiation-related health effects in a unique human population: Lessons learned from the atomic bomb survivors of Hiroshima and Nagasaki, Disaster Med. Public Health Prep. 5 (Suppl 1), S122–S133 (2011). [#546] PRESTON et al., Solid cancer incidence in atomic bomb survivors exposed in utero or as young children, J. Natl. Cancer Inst. 100(6), 428–436 (2008). [#547] U.S. NATIONAL ACADEMIES/NATIONAL RESEARCH COUNCIL. Health Risks from Exposure to Low Levels of Ionizing Radiation, BEIR VII, Phase 2, National Academies Press, Washington. D.C. (2006). [#548] UNITED NATIONS SCIENTIFIC COMMITTEE ON THE EFFECTS OF ATOMIC RADIATION. Sources and effects of ionizing radiation. UNSCEAR 2001 Report to the General Assembly with Scientific Annexes. Annex. Hereditary effects of radiation, New York, United Nations (2001). [#549] U.S. NATIONAL COUNCIL ON RADIATION PROTECTION AND MEASUREMENTS, Radiation dose management for fluoroscopically-guided interventional medical procedures, NCRP Report 168, Bethesda, NCRP (2010). [#550] UNITED NATIONS SCIENTIFIC COMMITTEE ON THE EFFECTS OF ATOMIC RADIATION, Sources and effects of ionizing radiation. UNSCEAR 1993 Report to the General Assembly with Scientific Annexes. Annex F. Influence of dose and dose rate on stochastic effects of radiation, New York, United Nations (1993). [#551] INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION, ICRP Statement on Tissue Reactions / Early and Late Effects of Radiation in Normal Tissues and Organs – Threshold Doses for Tissue Reactions in a Radiation Protection Context. ICRP Publication 118, Ann. ICRP Vol. 41 No 1-2, Elsevier (2012). [#552] INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION, 1990 Recommendations of the International Commission on Radiological Protection, ICRP Publication 60, Ann ICRP, Vol. 21, No 1-3 (1991). [#553] Cohen B. L. and Lee I. S., Catalogue of Risks Extended and Updated, Health Physics, Vol. 61 (1991) 317-335. [#554] FOOD AND AGRICULTURE ORGANIZATION OF THE UNITED NATIONS, INTERNATIONAL ATOMIC ENERGY AGENCY, INTERNATIONAL LABOUR ORGANIZATION, OECD NUCLEAR ENERGY AGENCY, PAN AMERICAN HEALTH ORGANIZATION, UNITED NATIONS OFFICE FOR THE COORDINATION OF HUMANITARIAN AFFAIRS, WORLD HEALTH ORGANIZATION, Preparedness and Response for a Nuclear or Radiological Emergency, IAEA Safety Standards Series No. GSR Part 7, IAEA, Vienna (2015)<to be updated>. [#555] INTERNATIONAL ATOMIC ENERGY AGENCY, WORLD HEALTH ORGANIZATION, Generic Procedures for Medical Response During a Nuclear or Radiological Emergency, Emergency Preparedness and Response Series, EPRMEDICAL, IAEA, Vienna (2005). [#556] INTERNATIONAL ATOMIC ENERGY AGENCY, PAN AMERICAN HEALTH ORGANIZATION, WORLD HEALTH ORGANIZATION, Cytogenetic Dosimetry: Applications in Preparedness for and Response to Radiation Emergencies, Emergency Preparedness and Response Series, EPR-BIODOSIMETRY, IAEA, Vienna (2011). 20 [#557] INTERNATIONAL ATOMIC ENERGY AGENCY, INTERNATIONAL LABOUR ORGANIZATION, Occupational Radiation Protection. IAEA Safety Standards Series No. <DS453>, IAEA, Vienna (2015)<to be updated> [#558] INTERNATIONAL COMMISSION ON RADIATION UNITS AND MEASUREMENTS, Quantities and Units in Radiation Protection Dosimetry, ICRU Report 51, ICRU, Bethesda (1993). [#559] INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION. Relative Biological Effectiveness (RBE), Quality Factor (Q) and Radiation Weighting Factor (wR). ICRP Publication 92. Ann ICRP Vol.33 No.4. Pergamon Press, Oxford, UK (2003). [#560] US NUCLEAR REGULATORY COMMISSION, EVANS, J.S., ABRAHAMSON, S., BENDER, M.A., BOECKER, B.B., GILBERT, E.S. and SCOTT, B.R. Health Effects Models for Nuclear Power Accident Consequence Analysis. Part I: Introduction, Integration, and Summary. NUREG/CR-4214 Rev. 2, Part I ITRI-141 (1993). [#561] INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION, Protection of the Public in Situations of Prolonged Radiation Exposure. ICRP Publication 82, Ann ICRP Vol. 29 No. 1-2. Pergamon Press, Oxford, UK (2000). [#562] EUROPEAN ATOMIC ENERGY COMMUNITY, FOOD AND AGRICULTURE ORGANIZATION OF THE UNITED NATIONS, INTERNATIONAL ATOMIC ENERGY AGENCY, INTERNATIONAL LABOUR ORGANIZATION, INTERNATIONAL MARITIME ORGANIZATION, OECD NUCLEAR ENERGY AGENCY, PAN AMERICAN HEALTH ORGANIZATION, UNITED NATIONS ENVIRONMENT PROGRAMME, WORLD HEALTH ORGANIZATION, Fundamental Safety Principles, IAEA Safety Standards Series No. SF-1, IAEA, Vienna (2006). [#563] COMITE TECHNIQUE INTERNATIONAL DE PRÉVENTION ET D’EXTINCTION DU FEU, INTERNATIONAL ATOMIC ENERGY AGENCY, PAN AMERICAN HEALTH ORGANIZATION, WORLD HEALTH ORGANIZATION, Manual for First Responders to a Radiological Emergency, Emergency Preparedness and Response Series EPRFIRST RESPONDERS, IAEA, Vienna (2006). [#564] UNITED NATIONS SCIENTIFIC COMMITTEE ON THE EFFECTS OF ATOMIC RADIATION. Sources and Effects of Ionizing Radiation. UNSCEAR 2000 Report to the General Assembly with Scientific Annexes. Annex J. Exposures and effects of the Chernobyl accident. New York, United Nations 2000. [#565] UNITED NATIONS SCIENTIFIC COMMITTEE ON THE EFFECTS OF ATOMIC RADIATION. Sources and Effects of Ionizing Radiation. UNSCEAR 2008 Report to the General Assembly with Scientific Annexes. Annex D. Health effects due to radiation from the Chernobyl accident. New York, United Nations 2011. [#566] Ghiassi-NEJAD M., MORTAZAVII S.M.J., CAMERON J. R., NIROOMAND-RAD A., and KARAM P. A., “Very High Background Radiation Areas of Ramsar, Iran: Preliminary Biological Studies,” Health Physics 82, no. 1, 2002: 87–93. [#567] UNITED NATIONS SCIENTIFIC COMMITTEE ON THE EFFECTS OF ATOMIC RADIATION. Sources and Effects of Ionizing Radiation. UNSCEAR 1994 Report to the General Assembly with Scientific Annexes. Annex B: Adaptive responses to radiation in cells and organisms. New York, United Nations 1994. [#568] LUCKEY T. D. Documented optimum and threshold for ionizing radiation, Int. J. Nuclear Law, 1, (2007) 378-409 [#569] Cohen, B. L.; Lee, I. S. A catalog of risks. Health Phys. Vol. 36 (1979) 707-722. 21 [#570] INTERNATIONAL ATOMIC ENERGY AGENCY, Safety Assessment and Verification for Nuclear Power Plants. IAEA Safety Standards Series No. NS-G-1.2, IAEA, Vienna (2001). [#571]FOOD AND AGRICULTURE ORGANIZATION OF THE UNITED NATIONS, INTERNATIONAL ATOMIC ENERGY AGENCY, INTERNATIONAL LABOUR ORGANIZATION, PAN AMERICAN HEALTH ORGANIZATION, UNITED NATIONS OFFICE FOR THE CO-ORDINATION OF HUMANITARIAN AFFAIRS, WORLD HEALTH ORGANIZATION, Arrangements for Preparedness for a Nuclear or Radiological Emergency, IAEA Safety Standards Series No. GS-G-2.1, IAEA, Vienna (2007). [#572] INTERNATIONAL ATOMIC ENERGY AGENCY, OECD/NUCLEAR ENERGY AGENCY, INES: The International Nuclear and Radiological Event Scale User's Manual. 2008 Edition, IAEA, Vienna (2009) [#573] UNITED NATIONS SCIENTIFIC COMMITTEE ON THE EFFECTS OF ATOMIC RADIATION. Sources and Effects of Ionizing Radiation. UNSCEAR 2008 Report to the General Assembly with Scientific Annexes. Annex C. Radiation exposures in accidents. New York, United Nations 2011. [#574] INTERNATIONAL ATOMIC ENERGY AGENCY, Categorization of Radioactive Sources, IAEA Safety Standards Series No. RS-G-1.9, IAEA, Vienna (2005). [#575] INTERNATIONAL ATOMIC ENERGY AGENCY, Code of Conduct on the Safety and Security of Radioactive Sources, IAEA/CODEOC/2004, IAEA, Vienna (2004). [#576] INTERNATIONAL ATOMIC ENERGY AGENCY, Considerations in Emergency Preparedness and Response for a State Embarking on a Nuclear Power Programme, Emergency Preparedness and Response Series EPR- EMBARKING, IAEA, Vienna, (2012). [#577] 22