In adult patients undergoing EVD insertion, does the risk of adverse
advertisement

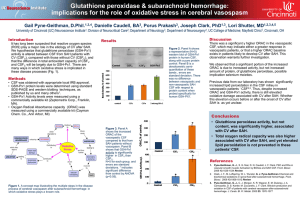
Evidentiary table 1 PICO Questions: Is there an increased risk of adverse mechanical or infectious events in adult patients undergoing EVD insertion outside the OR? In adult patients undergoing EVD insertion, does the risk of adverse events vary depending on the training, procedural experience or specialty of the clinician performing the procedure? Reference Patient Underlying Study [ #] number Clinical Design Condition(s) 13 188 2, 3, 4, 6 CS-R Gardner 2009 Endpoint Findings Quality Post-procedural hemorrhage following EVD insertion in OR vs outside OR No significant difference in post-procedural hemorrhages whether the EVD was placed in the OR versus ICU low 21 Foreman 2015 To compare safety and accuracy of placement between EVDs placed in the ICU versus OR Complications low of hemorrhage, infection, and non-functional drains may be mitigated by ventriculostomy placement in the OR. 150 1-6 CS-R Comments Patients who underwent ventriculostomy placement in the ICU differed in important ways (i.e. indication for placement and the administration of pre- procedure prophylactic antibiotics) from patients treated in the OR 12 Kakarla 2008 346 1, 2, 8 CS-R To study the safety and accuracy of ventriculostomy by neurosurgical trainees 8 O’Neill 2008 29 1, 2, 5, 6, 7 CS-R To evaluate accuracy and complication rates of EVD insertions by nonneurosurgeons Neither the moderate resident's training experience nor the side of placement seemed to affect accuracy No significant low Mixed differences in population of complication EVD and rates relative to fiberoptic ICP neurosurgical monitors series when EVD performed by nonneurosurgeons Key: Underlying Clinical Condition 1=ICH 2=SAH 3=IVH 4=TBI 5=tumor 6=infection 7=nontraumatic 8=unknown Study Design: CS-R=Case series cohort-retrospective, CS-P=Case series cohort-prospective, R=randomized trial Evidentiary table #2 PICO Question: In adult patients undergoing EVD insertion, does the risk of adverse events vary depending on the training, procedural experience, or specialty of the clinician performing the procedure? Reference Patient Underlying [ #] number Clinical Condition(s) 33 728 Craniotomy, Pollock shunt, JR 2001 Spinal surgery, stereotactic bx 35 29 1, 2, 3, 5, 6, Ehtisham 2009 Study Endpoint Design Findings Quality CS-R Surgical AEs in relation to # assisted cases Inverse relation between number of assisted cases and rate of AEs low CS-R EVD-related AEs low 12 Kakarla 2008 CS-R Accuracy of placement, AEs 1 infection (3.4%), 5 catheter tract hematomas <5cc (20.7%) when EVD inserted by NI Supervised junior trainee AE rates same as experienced residents 346 1, 2, 3, 4, 8 Comments low Key: Underlying Clinical Condition 1=ICH 2=SAH 3=IVH 4=TBI 5=tumor 6=infection 7=nontraumatic 8=unknown Study Design: CS-R=Case series cohort-retrospective, CS-P=Case series cohort-prospective, R=randomized trial AEs=Adverse Events, NI=neurointensivist Evidentiary table #3 PICO Question: What is the risk of bleeding with insertion of an EVD? Reference [ #] Patient Underlying Study Endpoint number Clinical Design Condition(s) 346 1, 2, 3, 8 CS-R Placement accuracy and AEs Findings Quality Comments 4 sympto matic bleeds low No risk factors for bleeding were identified #35 Ehtisham 2009 29 1, 2, 3, 4, 5, 6, 8 CS-R Placement accuracy and AEs low All procedures by neurointensivist. #11 Maniker 2006 160 1, 2, 3, 4, 5, 7 CS-R Hemorrhagic AEs low #13 Gardner 2009 188 1, 2, 3, 4, 6 CS-R Hemorrhagic AEs 0 sympto matic bleeds 4 sympto matic bleeds 77 (41%) bleeds #44 Naff 2011 48 1, 3 R AEs 28% low (for sympto matic bleeds) Non-significant increase in bleeding with smaller diameter catheter MR showed many bleeds, most small. 1 required surgery. Overall symptomatic bleeds unknown rtPA dose escalation. #12 Kakarla 2008 low # 43 Dey 2015 250 1, 3 R Bleeding, infection 16.8% bleeds, 2.4% sympto matic low CLEAR-III ongoing. Blinded for rtPA vs placebo reduced evidence quality for bleeding outcome Key: Underlying Clinical Condition 1=ICH 2=SAH 3=IVH 4=TBI 5=tumor 6=infection 7=nontraumatic 8=unknown Study Design: CS-R=Case series cohort-retrospective, CS-P=Case series cohort-prospective, R=randomized trial, AE=adverse events Evidentiary table #4 PICO Question: What procedural factors are associated with a decreased risk of catheter malposition? Reference Patient Underlyin [ #] number g Clinical Condition( s) 12 346 1,2,3,4,8 Kakarla 2008 Study Design Endpoint Findings Quality Comments CS-R 77% ideal 10% functional 13% malposition low Freehand placement 47 Patil 2013 109 1,2,3,4,5,7 CS-R Devised grading system for accuracy of positioning Malposition rates low Freehand placement 48 Bergdal 2013 147 1,2,3,4,5 CS-R Correct EVD placement low Bolt with freehand placement or freehand alone 49 Huyette 2008 50 Abdoh 2012 97 1,2,3,4,5 CS-R Catheter positioning low Freehand at bedside 66 2,3 CS-R Catheter positioning 79% ideal; TBI indication less often associated with ideal placement Bolted EVDs more accurate, and associated with lower reoperation rates. 22.4% malposition rate, only 56% in target location 4% extraventricular, 20% contralateral low Freehand bedside Key: Underlying Clinical Condition 1=ICH 2=SAH 3=IVH 4=TBI 5=tumor 6=infection 7=nontraumatic 8=unknown Study Design: CS-R=Case series cohort-retrospective, CS-P=Case series cohort-prospective, R=randomized trial AEs=Adverse Events, NI=neurointensivist Evidentiary table #5 PICO Question: In adult patients requiring EVD, what is the optimal method and timing of VTE prophylaxis? Reference [ #] Patient number Underlying Clinical Condition(s) Risk of Hemorrhage with Prophylaxis #88 100 Craniotomy Macdonald 2003 Study Design Endpoint Findings Quality Comments Pilot single center RCT DVT/PE within 1 month No significant differences in rates of DVT (0% vs 2%) or hemorrhage (2% vs 4%) in patients between heparin or LMWH VTE prophylaxis starting at the time of surgery No significant differences in the incidence of new hemorrhages (19.6% vs 16.3%), radiographicallysignificant hemorrhages (1.8% vs. 7.3%) and clinically significant hemorrhages (1.8% vs.3.6%) between patients Low Underpowered to detect small differences in clinically significant endpoint Postoperative intracranial hemorrhage #14 Tanweer 2013 99 1,2,3,4,5,6 CS-R EVDassociated hemorrhage LOW starting heparin prophylaxis within 24 hours or after 24 hours Grad[14]uated Compression Stockings (GCS) #76 2518 Ischemic Multicenter CLOTS stroke, RCT trial 1 hemorrhagic 2009 stroke #62 Agnelli 1998 307 5 (patients undergoing elective neurosurgery) Multicenter RCT Proximal DVT No significant difference in DVT with thigh length stockings. Significant increase in skin breakdown with stockings (odds ratio 4.2, 95% CI 2.4-7.3) Moderate Establishes potential harm from graduated compression stockings in comparable population Symptomatic PE or any DVT within 8 days Decreased rate of DVT in patients receiving LMWH + GCS compared to GCS alone (32% vs. 17%; p<0.01) High GCS alone associated with high rate of DVT, which is substantially reduced by addition of LMWH prophylaxis Low True efficacy in reducing PE in neurosurgical patients not No significant difference in major or minor bleeding between groups Inferior Vena Cava (IVC) Filters #84 400 Patients with Decousus proximal 1998 DVT Multicentre RC: pts randomized to anticoagulation PE within first 12 days of randomization No difference in PE at 2 years with IVC added to + IVC filter OR anticoagulation alone Intermittent Pneumatic Compression #78 2876 Ischemic Dennis stroke, 2013 hemorrhagic stroke Multicenter RCT anticoagulation clear as all patients in this study received anticoagulation. At 8 years follow up: Decrease in PE with IVC filter (6.2% vs. 15.1%; p<0.01) Increased DVT with IVC filter (35.7 vs. 27.5%; p=0.04) No difference in mortality Proximal DVT within 30 days Decreased VTE with IPC (adjusted OR 0·65 [95% CI 0·51–0·84]) Increased skin breakdown with IPC (3% vs. 1 %; p<0.01) However utility in primary prophylaxis may be limited by associated increase in subsequent DVT Moderate Establishes efficacy of IPC at preventing VTE in comparable population; with associated small risk but significant risk of skin breakdown. Trend towards decreased mortality with IPC (11% vs. 13%; p=0.06) Key: Underlying Clinical Condition 1=ICH 2=SAH 3=IVH 4=TBI 5=tumor 6=infection 7=nontraumatic 8=unknown Study Design: CS-R=Case series cohort-retrospective, CS-P=Case series cohort-prospective, R=randomized trial Evidentiary table 6 PICO Question: Infection Introduction Reference Patient Underlying [ #] number Clinical Condition(s) #97 34 3,6 Chan 1988 #98 87 1,2,3,4,5,8 Omar 2010 Study Endpoint Findings Design Quality Comments CS-P VL VRI No infections Unique, experimental EVD system 32% VRI VL VRI definition: (+) total, 52% culture AND (+) gram with VRI stain AND CSF changes after 10 (WBC>11, glucose<25, days protein>40) #101 172 2,3,4,5 CS-P VRI Risk(life VL VRI definition: (+) Mayhall table) of culture 24h after 1984 infection: insertion D#5=9%, D#8=21%, D#10=37%, D#11=42% Key: Underlying Clinical Condition 1=ICH 2=SAH 3=IVH 4=TBI 5=tumor 6=infection 7=nontraumatic 8=unknown Study Design: CS-R=Case series cohort-retrospective, CS-P=Case series cohort-prospective, R=randomized trial Endpoint: VRI=Ventriculostomy related infection Quality: VL=very low, L=low, M=moderate, H=high, VH=very high CS-P VRI Evidentiary table 7 PICO Question: In adult patients with an EVD, does the risk of infection increase with duration of placement? Reference [ #] #31Arabi 2005 #102 Korinek 2005 Patient Underlying Study Endpoint Findings number Clinical Design Condition(s) 1.2 OR 84 4,7,8 CS-P VRI Quality Comments VL total, OR (< 7 days) 2.82; OR >7 days 1.18 175 1,2,3,4,8 CS-P, CS-R VRI EVD >5d vs EVD>10d not a risk factor for infection. Days VL VRI Definition: Primary: (+)culture of known pathogen, secondary: "contaminant" with CSF or clinical meningitis OR CLINICAL only (CSF and pt changes) VRI Definition: Fever >38.5C, (+) a positive CSF culture associated with CSF #103 Scheithauer 2009 1333 NA CS-P VRI #104 Arif 2012 104 1,2,3 CS-R VRI mean+/SD VRI 12.5+/11, noVRI 9.4+/-7 No L significant difference in VRI in EVDs in less than or more than 9 days pleocytosis (>15 cells) CSF:plasma glucose ratio of less than 0.5 VRI Definition: CDC definition + CSF cellular and chemical changes + Clinical changes EVD> 8 days 16/19 VRI; EVD<4 days 3/19 VRI VRI Definition: (+) CSF culture. In the absence of positive culture, infection was defined as greater than 50% PMN on CSF count with a minimum of 50 cells or VL #105 Bota 2005 638 1,2,3,4,6,7 CS-P VRI #106 Camacho 2011 119 1,2,4,5 CS-P VRI #107 Chi 2010 197 1,2,3,4,5,8 CS-R VRI #108 Lyke 2001 157 1,4,5,7,8 CS-P VRI No infxn L until d#3, linear increase d3-10, sharp cutoff of infections after D#10 Catheter VL days noVRI 7 (133); VRI: 10.3(426) Mean VL daysVRI:20+/7.8d, noVRI 14.7+/10d VRI: 8.5d (2-23), no-VRI: 5.1d (1- VL CSF glucose less than 15mg/100ml VRI Definition: Per Lozier, et al. [91] VRI Definition: CDC, Horan, et al. [92] VRI Definition: Clinical suspicion + culture of a pathogen from CSF (except d#1) VRI Definition: Recognized pathogen OR 23). 73% of VAI developed after 6d skin flora and 1 or more criteria:(+) gram stain, low glucose, high protein, CSF PMN>10, excluded those with only (+) CSF parameters and (-) culture Key: Underlying Clinical Condition 1=ICH 2=SAH 3=IVH 4=TBI 5=tumor 6=infection 7=nontraumatic 8=unknown Study Design: CS-R=Case series cohort-retrospective, CS-P=Case series cohort-prospective, R=randomized trial Endpoint: VRI=Ventriculostomy related infection Quality: VL=very low, L=low, M=moderate, H=high, VH=very high Evidentiary table 8 PICO Question: In adult patients, do prophylactic systemic antimicrobials reduce the incidence of VRI? Should a periprocedural or duration regimen be used? Reference [ #] Patient number Arabi 2005 [31] 84 (58 for comparison) Underlying Clinical Condition(s) 4,7,8 Study Design Endpoint Findings Quality Comments CS-P VRI Periprocedural: Cefazolin OR Ceftriaxone OR Cefuroxime. VL VRI Definition: Primary: (+)culture of known pathogen, secondary: "contaminant" with CSF or clinical meningitis OR CLINICAL only (CSF and pt changes) VL VRI Definition: CDC, Horan, et al. [92] Antibiotic use associated with lower VRI rate; infection developed in 7 of 58 (12%) with antibiotics and in 12 of 41 (29%) when no antibiotics used (P = .03). #106 Camacho 2011 119 1,2,4,5 CS-P VRI Periprocedural: 1st or 2nd or 3rd or 4th generation cephalosporin. Use of antibiotics increased risk of VRI (nonsignificantly p=.22) with an OR of 1.8 #109 Dellit 2014 721 4 CS-R C. difficile colitis #101 Mayhall 1984 172 2,3,4,5 CS-P VRI #102 Alleyne 2000 [ 308 4,5,8 CS-P VRI Duration vs Periprocedural: Cefazolin No significant difference in VRI (p=.29). Significant drop in C. difficile when changed to periprocedural (5.4% to 2.4%, p=.04) Periprocedural: Nafcillin 4 doses. No significant difference between antibiotic and no antibiotic group (p=.09) VL VRI definition: (+) CSF culture VL VRI definition: (+) culture 24h after insertion Duration vs Periprocedural. Cefuroxime. No significant VL VRI definition: (+) CSF culture difference in VRI rate between duration (3.9%) and periprocedural (3.8%) #111 Poon 1998 228 4,5,8 R VRI Duration (D) vs Periprocedural (P) Amp/Sul +Aztreonam (D) vs Amp/Sul (P) Significant reduction in VRI in D cohort (p=.01), but more resistant organisms and higher mortality in D cohort. L #112 Saini 2012 42 1,2,3,4,5,8 R VRI #113 Wong 2006 255 4,5,8 R VRI Duration (D) vs VL Periprocedural (P). Ceftazadime. No significant difference in VRI between D (6.67%) and P(7.4%) Duration: Two VL antibiotic regimen. Amp/Sul +aztreonam vs Cefepime. Cefepime VRI definition: Not stated VRI definition: (+) CSF or EVD tip cultures. CSF drawn on D# 0,1,3,5 VRI Definition: At least one of the following criteria must have been met: (1)(+) Culture and/or (2) fever (>38 cohort with 6% VRI, Amp/Sul+aztreonam with 12% VRI #114 Blomstedt 1985 52 NA R VRI Duration: TMPVL SMX vs. placebo. No difference in VRI (1 from each group) Key: Underlying Clinical Condition 1=ICH 2=SAH 3=IVH 4=TBI 5=tumor 6=infection 7=nontraumatic 8=unknown Study Design: CS-R=Case series cohort-retrospective, CS-P=Case series cohort-prospective, R=randomized trial Endpoint: VRI=Ventriculostomy related infection Trimethoprim/sulfamethoxazole= (TMP/SMX) Ampicillin/Sulbactam=Amp/Sul Quality: VL=very low, L=low, M=moderate, H=high, VH=very high °C) and any of the following: (a) Increased white cells (>50% PMN), increased protein, and/or decreased glucose (<15 g/dL) or (+) CSF gram stain. All CSF infections within 3 months after EVD insertion considered to be related. VRI Definition: NA Evidentiary table #9 PICO Question: In adult patients with an EVD, does the use of antimicrobial-impregnated catheters reduce the incidence of VRI? Reference [ #] Patient number #115 Zabramski 2003 306 #116 Wong 2010 184 Underlying Clinical Condition(s) 2, 4,8 9, 4 Study Design Endpoint Findings Quality Comments R VRI ABX 1.3% vs. S 9.4% (p=0.002) H MLR for prediction of VRI ER placement (OR 7.3; p=0.035), Presence of other infection (OR 5.1;p=0.04 7), ABX catheter (OR 0.14, p=0.014) ABX 51% vs. S 57% (OR 1.3; 95% CI 0.7-2.2) VRI defined as positive CSF culture (i.e. organism grew on two different media) M VRI defined as a positive CSF culture and CSF white blood cell count > 10/mm3 CSF R VRI protein > 0.8 g/l, and CSF serum glucose ratio of < 0.4. Open label trial. #117 Pople 2012 484 1, 10, 11 R Proven VRI ABX 2.3 vs. S 2.8% (p=1.0) Suspected VRI ABX 17.6% vs. 20.4% (p=0.504) Duration of time to suspected infection ABX 8.8±6.1 days vs S 4.6±4.2 days (p=0.002) M Possible type 2 error Open label trial. Proven VRI was defined as positive gram stain and positive culture grown in agar. Suspected infection was defined as culture positive but not seen on gram stain or culture #118 Harrop 2010 Period 1 = 327 EVD 8 POC VRI Period 2 = 281 EVD Period 1 6.7% vs. Period 3 1.0% (p=0.005) L Period 3 = 195 EVD #119 Muttaiyah 2010 120 patient s and 986 CSF 8 POC compar ed to historic al VRI ABX 5% vs. C 15% (P=0.0627) VL negative but positive gram stain or CSF leukocytos is with a white blood cell/red blood cell count of > 0.02 VRI defined as 2 positive CSF cultures and a concurrent increase in the CSF white blood cell count. ABX catheters introduced in period 3; baseline = period 1 VRI defined as a positive CSF culture sample s #120 McLaughli n 2011 75 control s 2 POC VRI 9.3% Time to Infection Median of 16 days VL and CSF leukocytos is > 5 x 106 / L, CSF leukocytos is were corrected for erythrocyt es in the CSF by subtractin g1 leukocyte for every 1000 erythrocyt es in the CSF. No Compariso n group. VRI defined as organism isolated via culture and fever, headache, nuchal rigidity, meningeal signs, irritability AND #121 Mikhaylov 2014 145 10, 1, 2, 9, 4, 5, Retro VRI ABX 4% vs. 10% (p=0.193) VL #122 Keong 2012 278 1, 2, 4, 12 R VRI Silver 12.3% vs. 21.4% (p=0.0427) H antimicrobi al treatment AND any of the following: positive gram stain, increased white blood cells, elevated proteins and/or increased decreased CSF glucose, organism isolated from blood culture. VRI defined as a positive CSF culture. Possible type 2 error VRI was defined as organisms seen on microscop #123 Lackner 2008 39 1,2,9, 5, POC compar ed to historic al control s VRI Silver 0% vs. S 25% (p<0.05) VL #124 Fichtner 2010 164 1,2,4,8 Retro VRI Silver 18.9% vs. S 33.7 (p=0.04) L #125 Lajcak 2013 403 patient s with 529 EVD 61 1,2,4,5 Retro VRI Silver 6.1% vs. S 13.8 (p=0.003) VL 2 R VRI Silver 10% vs. ABX L #126 Winkler y or isolated by culture or clinical meningitis requiring treatment. Possible Type 1 error. VRI defined as positive culture. VRI defined as positive culture or colonizatio n of catheter tip with microorga nism or raised liquor cell count > than 4 cells/mcl. VRI defined as positive CSF culture. Confirmed VRI 2010 #127 Lemcke 2012 18% (p=0.71) 95 1,2,4,10 Retro VRI Silver 9.4% vs. ABX 6.5% vs. S 15.6 defined as leukocyte count per visual field > 200 and clinical signs of CSF infection present and microorga nisms identified in the CSF or catheter tip. Probable VRI defined as leukocyte count per visual field > 100 and/or one or cmore of the confirmed VRI items. VL Possible type 2 error VRI defined as the identificati (p>0.05) on of microorga nisms in the CSF. Possible type 2 error Key: Underlying Clinical Condition 1=ICH 2=SAH 3=IVH 4=TBI 5=tumor 6=infection 7=nontraumatic 8=unknown 9=stroke 10=hydrocephalus 11=Edema 12=AVM 13=SDH Study Design: CS-R=Case series cohort-retrospective, CS-P=Case series cohort-prospective, R=randomized trial, POC = Prospective Observational Cohort, Retro = retrospective Endpoint: VRI=Ventriculostomy related infection, MLG=multivariate logistic regression Findings: ABX=antibiotic impregnated catheter, S=Silicone catheter, C=Control Quality: VL=very low, L=low, M=moderate, H=high, VH=very high Evidentiary table 10 PICO Question: Are additional intra-ventricular antimicrobials effective for the treatment of VRI as compared to intravenous antimicrobials alone? Reference [ #] Patient number Underlying Clinical Condition(s) 1, 4, 6 ( Staphylococcal VRI) Study Design #133 Pfausler 2003 10 #134 Remes 2013 #129 Wilke 2013 Endpoint R – Vent only Vs IV only -CSF bacteriologic clearance. -CSF vancomycin Levels 34 1,2,5,6,7 CS Vent+ IV Vs IV only 48 1, 2,3,5, 7 CS-R Vent+ IV Vs IV only -Time to CSF bacteriologic clearance. -Modified Rankin scale. -Attributable death. -Adverse effects. -Time to CSF bacteriologic clearance. -Time to normalization of CSF WBC count. -Length of stay. -Length of IV. VRI=Ventriculostomy related infection Quality: VL=very low, L=low, M=moderate, H=high, VH=very high Interventions: Vent- Intraventricular antimicrobials, IV: intravenous antimicrobials Findings Higher CSF vancomycin level with intraventricular compared to intravenous with no difference in CSF bacterial clearance Earlier time to CSF clearance and clinical outcome ( see text for details) All the outcomes were significantly better with vent+IV ( see text for details) Quality Comments VL The study, though an RCT, was underpowered VL Underpowered VL Retrospective study with a scope for bias and confounding PICO Question: Are additional intra-ventricular antimicrobials effective for the treatment of VRI as compared to intravenous antimicrobials alone? Key: Underlying Clinical Condition 1=ICH 2=SAH 3=IVH 4=TBI 5=tumor 6=infection 7=nontraumatic 8=unknown Study Design: CS-R=Case series cohort-retrospective, CS-P=Case series cohortprospective, R=randomized trial Endpoint: Evidentiary table 11 PICO Question: In adult patients requiring an EVD, does routine CSF sampling increase EVD-related infections as compared to maintaining a closed system with sampling of CSF only when clinically indicated? Ref No. Author/ Year Patient number Study Design Endpoint Findings Quality Comments 84 Underlying Clinical Condition(s) 1, 4, 5, 6 31 Arabi/ 2005 CS-R Frequency of CSF sampling Very low Single center, small number of patients, retrospective review Stenager/ 1986 85 1, 2, 3, 4, 5 CS-P Very low Single center, small number of patients, CSF sampling included with other manipulations 136 Kitchen/ 2011 133 2 CS-R Frequency of manipulations was monitored; included CSF samples, irrigation when occluded, change of EVD Frequency of CSF sampling; compared control group with sampling when indicated vs. research group is frequent sampling Found no difference in VRI* – CSF daily samples vs. CSF samples when indicated Found no difference in VRI associated with number of catheter manipulations 135 Frequency of VRI was significantly lower in research group with sampling group Very low 137 Williams/ 2011 382 2, 4 CS-P Historical control group – daily CSF sampling vs. every 3rd day CSF sampling Very low 138 Williamson/ 2014 420 Not provided CS-R Monitored frequency of CSF sampling Switch to every 3rd day sampling was associated with a significant decrease in VRI (p = 0.02) Univariate and multivariable analysis Single center, retrospective review, control group very high VRI rate of 52.1%; comparison of the effect of sampling frequency on VRI in research group was complicated by implementation of an EVD management bundle Confounding influence was use of AI-EVD* in 75% of patients in prospective study arm of every 3rd day CSF sampling Single center, frequency of CSF sampling was monitored Low modeling found CSF sampling was associated with a significantly increased risk of VRI Key: Underlying Clinical Condition 1=ICH 2=SAH 3=IVH 4=TBI 5=tumor 6=infection 7=nontraumatic 8=unknown Study Design: CS-R=Case series cohort-retrospective, CS-P=Case series cohort-prospective, R=randomized trial VRI* = ventriculostomy associated infection, AI-EVD* = antibiotic-impregnated external ventricular drain catheter and not specified Evidentiary table 12 PICO Question: In adult patients requiring an EVD, do routine catheter changes decrease the incidence of VRI compared to no catheter changes? Ref No. First Author/ Year Patient number Study Design Endpoint Findings Quality Comments 84 Underlying Clinical Condition(s) 1, 4, 5, 6 31 Arabi/ 2005 CS-R Rate of VRI was significantly higher in patients with 2 or more EVDs (p < 0.001) Low Single center, small number of patients, retrospective review Mayhall/ 1984 172 4 CS-P VRI* rate – VRI rate in patients with single EVD placement vs the rate in patients requiring 2 or more EVDs VRI rate epidemiology study performed to identify risk factors for VRI 101 Very low Single center, observational study, recommendation based on small number of observations (only 19 positive culture cases). 135 Stenager/ 1986 85 1, 2, 3, 4, 5 CS-P VRI rate and catheter duration Risk of VRI increased after 5 days, recommended changing EVD site if monitoring required for more than 5 days VRI were equally distributed from day 2 to 11; no new infections after day 11 Very low 142 Holloway/ 1996 584 4 CS-R VRI rate and catheter duration Low 143 Lo/ 199 1, 2, 4 CS-R VRI rate Patients that had catheters replaced prior to 5-days did not have a lower infection rate. Incidence of infection declined after 10 days in single catheter group Univariate and Single center, small number of patients, indirect evidence based on analysis of VRI and catheter duration Single center, retrospective review, Low Single center, retrospective 2007 144 Park/ 2004 595 1, 2, 3, 4, 5 CS-R VRI rate and catheter duration 145 Wong/ 2002 103 4, 7, 8 R VRI rate – Group 1 – routine change of EVD site every 5 days vs. Group 2 – no change unless clinically required multivariate analysis found a significantly increased risk of infection associated with each EVD insertion (p < 0.001) Rate of infection plateaued after 4 days and was not affected by catheter changes No significant difference in VRI rate between two groups (p = 0.50) review Low Single center, retrospective review, indirect evidence Moderate Limited to two centers, small sample size, infection rate was twice as frequent in Group 1 (7.8%) compared to Group 2 (3.8%) reflecting a possible Type 2 error Key: Underlying Clinical Condition 1=ICH 2=SAH 3=IVH 4=TBI 5=tumor 6=infection 7=nontraumatic 8=unknown Study Design: CS-R=Case series cohort-retrospective, CS-P=Case series cohort-prospective, R=randomized trial VRI* = ventriculostomy associated infection Evidentiary table 13 PICO Question: In adult patients requiring an EVD does gradual weaning decrease the incidence of hydrocephalus and need for VP shunting as compared to immediate clamping? Ref No. First Author/ Year Patient number 146 Klopfenstein/ 2004 91 Underlying Clinical Condition(s) 2 Study Design Endpoint Findings Quality Comments R Comparison of VP shunting rates in a two groups: Group 1 – standard 4 day gradual weaning protocol vs. Group 2 – simple clamping No difference in VPshunting rates in the two groups. The gradual weaning group spent a mean of 2.8 more days in the ICU (p = 0.0002) and 2.4 more days in the hospital (p = 0.0314) Medium Single center, small number of patients, study limited to aneurysmal SAH patients. Key: Underlying Clinical Condition 1=ICH 2=SAH 3=IVH 4=TBI 5=tumor 6=infection 7=nontraumatic 8=unknown Study Design: CS-R=Case series cohort-retrospective, CS-P=Case series cohort-prospective, R=randomized trial Reference 130 and 142 are duplicates Evidentiary table 14 PICO Question: In adult patients requiring an EVD, does the type of dressing reduce VRI? Ref No. First Author/ Year Patient number 147 Bookland/ 2014 332 149 Honda/ 2010 911 Underlying Clinical Condition(s) 1, 2, 4, 5, 7, 8, Study Design Endpoint Findings Quality Comments CS-R Single center, retrospective review CS-R VRI rates were significantly decreased in the treatment group (3.54%) vs. the control group (15.1%) p = 0.002 VRI rates were decreased from 3.29 per 1,000 catheter days in the control group to 2.17 per 1,000 catheter days in the treatment group Low 1, 7, 8 VRI* rate in control group – semi-occlusive dressing EVD site vs. treatment group dressing of EVD wounds with cyanoacrylate VRI rate in control group – semi-occlusive gauze dressing changed only if necessary vs. treatment group – semi-occlusive gauze dressing changed every 48 hrs Very low Single center, retrospective review, only a trend for decreased VRI rate demonstrated Key: Underlying Clinical Condition 1=ICH 2=SAH 3=IVH 4=TBI 5=tumor 6=infection 7=nontraumatic 8=unknown Study Design: CS-R=Case series cohort-retrospective, CS-P=Case series cohort-prospective, R=randomized trial VRI*=Ventriculostomy related infection Evidentiary table 15 PICO Question: In adult patients, does routinely changing the tubing and collection devices decrease the incidence of EVD-related infection? Ref No. First Author/ Year Patient number Study Design Endpoint Findings Quality Comments 32 Underlying Clinical Condition(s) 8 150 Duncan/ 2011 CS-R Changing drainage sets weekly was associated with a decreased risk of VRI Very low Single center, retrospective review, very small number of patients, published as a peer reviewed meeting abstract Korinek/ 2005 377 8 CS-R Comparison of VRI* rates in control group – change of drainage sets every 3-days vs. changing drainage sets once per week VRI rates before and after implementation of a EVD care bundle 102 Very low Single center, retrospective review, indirect evidence against any manipulation of the EVD drainage system American Association of Neuroscience Nurses NA NA Expert consensus statement During the study period VRI rates were significantly associated only with CSF leak and protocol violations Inappropriate CSF bag sampling p = 0.0002 Inappropriate CSF tap sampling p < 0.0001 EVD manipulation p < 0.0001 Recommends against routinely changing EVD components 152 Very low Consensus statement Key: Underlying Clinical Condition 1=ICH 2=SAH 3=IVH 4=TBI 5=tumor 6=infection 7=nontraumatic 8=unknown Study Design: CS-R=Case series cohort-retrospective, CS-P=Case series cohort-prospective, R=randomized trial VRI*=Ventriculostomy related infection Evidentiary table 16 PICO Question: In adult patients does introduction of an EVD management bundle reduce the risk of EVD related infections? Ref No. First Author/ Year Patient number 140 Kubilay/ 2013 2,928 EVD* placements (no. of Underlying Clinical Condition(s) 8 Study Design Endpoint Findings Quality Comments CS-R VRI* rate following implementation of an EVD management bundle VRI rate decrease from 9.2% in the control period to 0.46% following bundle implementation Low Single center, retrospective review. Note: Bundle included an AI-EVD* catheter During the study period VRI rates were significantly associated only with CSF leak and protocol violations Inappropriate CSF bag sampling p = 0.0002 Inappropriate CSF tap sampling p < 0.0001 EVD manipulation p < 0.0001 VRI rate decreased significantly when the EVD management bundle included an AIEVD (p ≤ 0.005) VRI rates were decreased from 3.29 per 1,000 catheter days vs. 0.87 per 1,000 catheter days (p = 0.066) Very low Single center, retrospective review, indirect evidence against any manipulation of the EVD drainage system Medium Single center, retrospective review. Study periods without and with the use of AI-EVD strengthen the quality of the results Single center, retrospective review patients not provided) 102 Korinek/ 2005 377 8 CS-R VRI rates before and after implementation of a EVD care bundle 118 Harrop/ 2010 1,634 8 CS-R VRI rate following implementation of an EVD management bundle 149 Honda/ 2010 911 1, 7, 8 CS-R VRI rate before and after implementation of an EVD management bundle Low 154 Bader/ 1995 19 8 CS-R VRI rate following implementation of a best practice EVD bundle Infection rate reduced Very-low from 55.5% (n=9) in 6-month interval before vs. 0% (n=10) after implementation of bundle 155 Camacho/ 178 1, 2, 4, 5 CS-R VRI rate during a series Education Low 2013 of four educational interventions were interventions as part of useful in reducing EVD management theVRI rate. During bundle the study, EVD-related infection rates decreased from 9.5% to 4.8% per patient, from 8.8% to 4.4% per procedure, and the incidence density dropped from 14.0 to 6.9 infections per 1000 catheters-day (p = 0.027). 156 Dasic/ 95 8 CS-R VRI rate before and Infection rate reduced Low 2006 after implementation of from 27% before vs. an EVD management 12% after bundle implementation of bundle (p < 0.05) 157 Flint/ 262 EVD 1, 2, 3, 4, 5, CS-R VRI rate before and Infection rate reduced Low placements 8 2013 after implementation of from 9.8% before vs. (no. of an EVD management 0.8% after patients not bundle implementation of provided) bundle (p = 0.02) Key: Underlying Clinical Condition 1=ICH 2=SAH 3=IVH 4=TBI 5=tumor 6=infection 7=nontraumatic 8=unknown Study Design: CS-R=Case series cohort-retrospective, CS-P=Case series cohort-prospective, R=randomized trial EVD*=external ventricular drain, VRI*=Ventriculostomy related infection, AI-EVD*=antibiotic-impregnated EVD Single center, retrospective review, small number of patients Single center, retrospective review. Single center, retrospective review Single center, retrospective review. Note: Bundle included an AI-EVD catheter