Point-of-care CD4 counter for resource-poor areas
advertisement

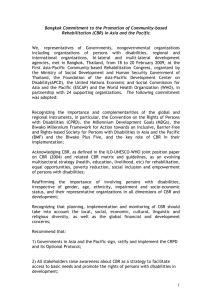
Senior Design 2010-2011 Point-of-care diagnostic device for monitoring CD4 levels of HIV patients in resource-poor settings Lina M. Aboulmouna Peter F. DelNero Parker A. Gould Rosalynne R. Korman Christopher M. Madison Stephen R. Schumacher Advisor: Dr. Kevin T. Seale Abstract The goal of this project is to design a point-of-care device that quickly and cost-effectively determines the CD4 count of an HIV-positive patient. This count is essential in determining a patient’s suitability for antiretroviral treatment. The device is comprised of a microfluidic platform for immunology and cell trap-based separation of white blood cells, coupled with a CCD camera to capture and quantify fluorescent signals from tagged CD4 cells. This device is designed to facilitate a simple, quick diagnosis of a patient’s stage in the HIV/AIDS progression, which is crucial in the resource-poor medical setting found in many developing countries. The design parameters include a per-test cost of under $2, minimal power requirements, simple operation by minimally-trained technicians, and same-day test results. The motivation for this project stems from the Gates Foundation CD4 Initiative for a low-cost, point-of-care device to replace flow cytometry for accurate CD4 cell counting in under-developed regions. Introduction Acquired immunodeficiency syndrome (AIDS) is a disease caused by the human immunodeficiency virus (HIV). Not everyone who is HIV-positive has AIDS; only when HIV has depleted CD4 T helper lymphocytes beyond the given threshold of 200 cells per microliter of whole blood is the patient considered to have AIDS. There is an inverse relationship between the replication of HIV-1 and the destruction of lymphocytes. As HIV progresses, more and more 1 HIV-1 RNA circulates in the bloodstream while fewer and fewer CD4 cells are left. CD4 lymphocyte counts are predictive of progression to AIDS and, eventually, death.1 The World Health Organization has declared finding an affordable and effective way to obtain CD4 lymphocyte counts in resource poor areas a high priority.2 Similarly, the Gates Foundation has identified low-cost HIV diagnostics as one of its Grand Challenges in Global Health.3 CD4 counts provide important information to an attending physician on the current stage of the disease, when to initiate antiretroviral treatment, how the patient is responding to treatment, and when to consider modifying the current treatment regimen. Flow cytometry is the traditional method for obtaining CD4 counts. However, flow cytometry is generally limited to developed countries because of its requirements of expensive instrumentation and a trained staff.4 Lacking the financial and technical means to obtain these CD4 counts, HIV/AIDS treatment in poor countries is often started too soon or too late, which can result in poor clinical outcomes, unnecessary burdens on the patient, and imprudent or inefficient use of the limited resources available. Along with other signs and symptoms, CD4 lymphocyte counts are used to stage the progression of HIV infection according to standards set by the Centers for Disease Control and Prevention (CDC). Patients with HIV who have CD4 counts above 500 cells/µL are in stage 1 infection, O’Brien, WA, Hartigan, PM, Daar, ES, Simberkoff, MS, and Hamilton, JD. Changes in plasma HIV RNA levels and CD4þ lymphocyte counts predict both response to antiretroviral therapy and therapeutic failure, VA Cooperative Study Group on AIDS. Ann Intern Med 126: 939–945 (1997). 1 2 http://www.who.int/hiv/pub/guidelines/artadultguidelines.pdf 3 http://www.nature.com/nm/journal/v13/n10/full/nm1007-1131.html Rodriguez, WR, et al. A Microchip CD4 Counting Method for HIV Monitoring in Resource-Poor Settings, PLoS Medicine, July 2005, Volume 2, Issue 7. 4 2 CD4 counts between 500 cells/µL and 200 cells/µL are in stage 2, and CD4 counts of 200 cells/µL and below are in stage 3 and are classified as having AIDS.5 Both the World Health Organization (WHO) and the CDC recognize the importance of CD4 counts in deciding when to initiate antiretroviral treatments and when to adjust treatments. These organizations have provided guidelines for making these decisions based on the CD4 count for a particular patient.6 There are other methods of quantifying the progression of HIV and AIDS, such as CD4/CD8 ratios and nucleic acid amplification tests. Based on the CDC’s standards for the stages of HIV and AIDS, as well the work of others in the field, we have decided to focus this project on obtaining accurate CD4 counts. History and Context Previous work Rodriguez et al. previously fabricated a microchip similar to our proposed device for HIV diagnostics.4 However, our device differs significantly in the manner by which a whole blood sample is tagged and filtered. Also, due to the pumping mechanism we have utilized, our device is significantly less expensive to fabricate and use. 5 6 http://www.aids-ed.org/aidsetc?page=cm-105_disease#S1X http://www.who.int/hiv/pub/guidelines/artadultguidelines.pdf 3 Methodology Microfabrication of device components Two microfluidic platforms connected by PEEK tubing (150µm inner diameter, 360µm outer diameter) comprise the HIV test platform. These components are fabricated by PDMS soft lithography using an SU-8 mold according to protocols developed at the Vanderbilt Institute for Integrative Biosystems Research and Education (VIIBRE). The protocol is briefly outlined below, and in Figure 1. The microfluidic device patterns were designed using Autodesk’s AutoCAD software package. These patterns were reproduced to scale by selectively etching a chrome-plated glass mask. Master molds were then fabricated on three-inch silicon wafers using MicroChem SU-8 photoresist and the chrome masks, in accordance with the standard photolithographic protocol practiced in the VIIBRE cleanrooms. Sylgard 184 PDMS (DowCorning) prepolymer was mixed with the corresponding curing agent at a 10:1 mass ratio, cast onto the mold, degassed in a vacuum chamber for 20 minutes, and then cured at 70°C for four hours. The PDMS was then carefully peeled from the mold and inlet/outlet holes were punched using sharpened Luer-Lock syringe tips. 4 Figure 1: Step-by-step procedures for photolithography and replica molding. The patterned PDMS and a glass coverslip were then exposed to an oxygen plasma for 30 seconds, and then placed in contact with one another, causing a hydrolysis reaction and a permanent bond between the PDMS and glass. The microfluidic peristaltic pump was fabricated using a similar replica molding-based protocol. An SU-8 patterned silicon wafer was spun with a thin layer of uncured PDMS, and then cured cubes of PDMS were placed above the inlet/outlet hole patterns. These cubes serve to provide structural stability for the inlet/outlet tubing connections. This two-layer PDMS device was then allowed to cure at 70°C for 4 hours, along with a flat, unpatterned, 1 mm thick layer of PDMS in a separate petri dish. After curing, the two-layer patterned PDMS device (both layers now sealed together) was removed from the silicon master, and inlet/outlet holes were punched. The device was then bonded to the concurrently prepared 1 mm thick layer of PDMS using an oxygen plasma. 5 Blood Sample Preparation Whole blood samples were acquired via finger stick from volunteers using the procedure established by the Vanderbilt University Institutional Review Board. Samples were obtained using a standard CVS brand finger-stick device. A 75 mm Fischer microhematocrit tube was used to collect approximately 35L of whole blood. Whole blood was aspirated directly from the hematocrit tube into the device through PEEK tubing. Pumping The peristaltic pump operates by compressing a microfluidic track with ring of ball bearings. The motor is automatically controlled through a microchip using Arduino software. The pump is also capable of manual control by rotating the shaft. The flow rate is determined by the diameter of the microfluidic track, which can be tailored to optimize sample loading. Figure 2: Hand-crankable peristaltic pump. A novel microfluidic pump was designed which allows manual pumping of inputs through the device. The pump’s rotation forces fluid through the device, and the hand-crank mechanism allows for the pump to be operated with no electrical power input. The device is composed of inlet ports for the various inputs, mixer elements to insure proper mixing, and the circular array of channels to allow pump action. 6 White blood cell trapping White blood cells were captured using a trap device developed in SyBBURE/VIIBRE. Cells are captured in the array of U-shaped traps as demonstrated in Figure 3. While red blood cells are small and flexible enough to squeeze through the gaps in each trap, white blood cells remain confined. The downstream flow prevents cells from escaping. In order to extract the maximum number of cells from a volume of blood, the outlet tube was connected to the inlet port and the sample was recirculated through the device. Figure 3: Microfluidic trap device. An array of U-shaped structures captures cells as they flow through the device. (Inset) Magnified diagram is of a cell trap containing two cells (green). Inset by K. Seale. Fluorescent CD4 labeling with FITC FITC-conjugated CD4 antibodies were used to label both CD4 Jurkat T lymphocytes and CD4 cells from whole blood. Cells were captured in the trap device, after which fluorescent antibodies were pumped through. Finally, the traps were rinsed with PBS solution to remove excess antibodies. Fluorescent images were captured using a Zeiss microscope equipped with a FITC filter. Off-chip labeling was accomplished by mixing antibody solution in a 1:5 ratio with cells and incubating for 30 minutes prior to loading the trap chambers. 7 Time-resolved fluorescent imaging Latex beads containing europium were conjugated to anti-CD4 antibodies according to the protocol developed with the aid of Dr. Robert Buck of Gauge Scientific: 1. Suspend antibodies and CMEUs (carboxylate-modified europium nanoparticles) at 30 g IgG/mg CMEU in the coating buffer: 10mM NaPO4 pH 8.0 . 2. Allow the antibodies to coat the CMEUs for 1-2 hours, with gentle shaking. 3. After the coating, spin down the CMEUs, remove supernatant, and resuspend in blocking buffer: either 10 mg/ml BSA in buffer, or 5% PEG in buffer. 4. Wash 2 or 3 times: Spin down the CMEUs at 10,000-12000g, remove supernatant, resuspend in blocking buffer. 5. Spin down CMEUs, remove supernatant, resuspend in Conjugate Dilution Buffer (obtained from Gauge Scientific). The Vanderbilt Reader, purchased from Gauge Scientific and shown in Figure 4, enables microsecond resolution of digital image acquisition, allowing autofluorescent noise to diminish before collecting images of the europium signal, as shown in Figure 5. Figure 4: The Vanderbilt Reader. A portable, point-of-care time resolved fluorescence (TRF) platform. This imaging device connects to a laptop via a USB connection. 8 Figure 5: TRF imaging generates a fluorescent excitation but does not capture an image until after a short time delay. This time delay allows cellular auto-fluorescence and background fluorescence (blue line) to decay to minimal levels, while the fluorescence from europium nanoparticles (red line) remains strong. Results and Discussion The microfluidic peristaltic pump was able to induce precise and reliable flow rates in the cell trap device. Manual operation was capable of controlling nanoliter volumes. Each revolution of the bearing yields approximately 200 nL of flow. In addition, the feasibility of direct trap loading and cell labeling on chip via aspiration of whole blood directly from a microhematocrit tube was confirmed experimentally: this result is summarized in Figure 6. This ability to perform all of the required mixing on chip represents a significant reduction in the difficulty of operation, thereby eliminating the need for pipets and trained technicians. By rinsing the pump device with buffer solution (and replacing the cell trap device), a second test can be performed immediately using the same blood sample. A second test provides significant confirmation to the outcome of the first test, which allows for more confident diagnosis. Flushing the pump with ethanol immediately prepares the device for the next patient. 9 Figure 6: FITC-CD4 antibodies identify CD4 cells in whole blood. Although the CD4 cells are initially indistinguishable in a sea of red blood cells (A), they become discrete when illuminated with fluorescence (B). As whole blood is flowed through the device, red blood cells pass through while some white blood cells are trapped. DIC (C) and FITC (D) images were taken at t = 0 sec, 6 sec, and 6 min. FITC images were thresholded (E) and overlayed on top of the corresponding DIC images (F). The number of trapped CD4 cells increases over time from 1 to 2 to 4, suggesting that the number of trapped CD4 cells will continue to increase as the whole blood is recirculated through the device. The multitrap nanophysiometer captured white blood cells (WBC) from whole blood. Recirculation of the blood helps to increase the cell trapping efficiency, which is crucial to producing a reliable diagnosis of CD4 cells per microliter. Fluorescent microscopy images show accumulation of CD4 cells over time in a localized field of view due to trapping, as seen in Figure 6. Alternative trap layouts with increased density and offset patterning were fabricated on 10 chrome masks to optimize WBC capture. The trap device is disposable and affordable, costing approximately $0.15 per chip. On-chip fluorescent labeling of WBCs from whole blood samples was performed with FITCconjugated anti-CD4 antibodies. Images were acquired from the Zeiss optical microscope and the ImageJ software suite was used for image analysis: several representative images are displayed in Figure 7. The labeling demonstrated selective binding to CD4 cells in whole blood with significant signal output after rinsing with buffer. This demonstrated that the only manual sample preparation required will be the original finger prick and loading a new trap device. Figure 7: CD4 cells can be labeled on chip. FITC-CD4 antibodies were flowed into a device containing Jurkat T cells. The excess antibodies were rinsed from the device, revealing the presence of newly-labeled CD4 Jurkat cells. A series of fluorescent pictures (A) is given, as well as the overlay of the fluorescent and DIC images (B). This is proof of concept that CD4 cells can be labeled on chip. Attempted conjugation of anti-CD4 antibodies to carboxylate-modified europium chelate nanoparticles did not yield detectable binding to CD4 cells. A reliable conjugation and labeling protocol has been investigated in collaboration with Dr. Buck of Gauge Scientific and Dr. Jay Dickerson of the Vanderbilt Physics Department. The detection threshold using the Vanderbilt 11 Reader portable TRF device was approximately 1:25 dilution from the original nanoparticle concentration (1% solids). These detection threshold test images are displayed in Figure 8. 1:1 1:10 1:25 1:50 1:100 Figure 8: TRF images of cell traps. Europium nanoparticles were pumped into a trap array, and a TRF images were taken. This figure demonstrates that europium phosphorescence can be detected at dilutions as low as 1:25. Also, the resolution of the TRF image was high enough to illustrate the microscale structure of the trap array, which promises to aid diagnosis by allowing trap-by-trap image analysis instead of less precise macroscale analysis. Healthy and immuno-suppressed data were simulated by combining measurements from the FITC-labeled whole blood with accepted concentrations of CD4 lymphocytes. Cell size and signal intensity data were used to calculate the relative signal ratio in healthy versus diseased patients. The absolute quantification of CD4 cells per microliter of blood is a function of the total signal intensity in the Vanderbilt Reader and the fraction of CD4 cells captured during recirculation. The signal intensity of the europium-chelate nanoparticles was used to estimate a minimum threshold of trapped cells needed to obtain a detectable signal in the Vanderbilt Reader, and from this threshold the minimum number of recirculation passes was calculated. Assuming the europium fluorescence of a particular labeled cell is equivalent to the fluorescent intensity observed in the device from the conjugated europium solution, calculations suggest that 6.8% of the device area must be illuminated to reach the detection threshold. However, this assumption depends on the concentration of CD4 receptors on the lymphocytes, which must be 12 determined experimentally with europium conjugated particles. According to these results, approximately 22700 cells must be captured; a finger-stick equivalent of 40% of CD4 WBCs in healthy patients and 150-250% in an AIDS patients. Therefore, unless the actual signal strength of europium-labeled cells is higher than the original diluted signal, a magnifying lens of at least 10x power should be added to the TRF detection system. Detection Threshold Calculations We performed a theoretical analysis of the fluorescent behavior of cells the trap device. The variables defined below are used in Equation 1. s = n = n+ = f+ = p = ℓ = number of pixels in the field of view (FOV) of the image of the trap device number of white blood cells in FOV number of CD4 cells in FOV fraction of white blood cells that are CD4 number of pixels that are lit due to fluorescence of a single tagged CD4 cell fraction of FOV that is illuminated The total number of pixels in FOV that are lit is given by (n+)(p), which is equal to (f+)(n)(p). Therefore, the luminance ℓ is given by Equation 1 ℓ= 𝑓+ 𝑛𝑝 (1) 𝑠 This value is exact if the cells in the trap device can be resolved by the imaging device (i.e. a single cell’s size is multiple pixels, or, more precisely, the fluorescence of a tagged cell is multiple pixels). However, this resolution constraint requires a powerful microscope and is therefore unsuitable for a point-of-care product. Another analysis, based on the illumination of the device as a whole, is needed. For this analysis, we define the following variables. H A V Ac ac = = = = = height of the trap chamber area of the trap chamber (as viewed from above) volume of the trap chamber area of the trap chamber occupied by CD4 cells (as viewed from above) cross-sectional area of a CD4 cell 13 N+ = total number of CD4+cells trapped in the trap chamber Using these variables, we can define the macroscopic luminance as ℓ𝑚 = 𝐴𝑐 𝐴 = 𝑎𝑐 𝑁+ 𝐴 (2) Finally, assuming that during a test, we flow in enough blood to exactly fill the trap chamber, then the CD4 count is exactly N+/V, i.e. the number of CD4 cells per volume of blood. But N+ is equal to Ac/ac, and V is equal to the area of the trap chamber times its height. Therefore, the CD4 count is given by 𝑁+ 𝑉 = 𝐴𝑐 𝑎𝑐 = 𝐻𝐴 ℓ𝑚 𝑎𝑐 𝐻 (3) Then, since the average cross-sectional area of a CD4 cell is about 40 µm2,7 and the height of the trap chamber is set by the production process (typically between 11 and 15 m) all that is required to determine the CD4 count is a measurement of the luminance. However, this macroscopic luminance is no longer an exact, pixel-by-pixel value. A correlation between the microscopic luminance ℓ and the macroscopic luminance ℓ𝑚 is necessary. In order to accomplish this, experiments are needed which measure the two luminances from a single trap device to calibrate the macroscopic luminance to its microscopic counterpart. A final consideration concerning the detection of CD4 cells in this device is how to achieve the requisite concentration of cells in the trap chamber for the imaging device to make a reliable measurement of the CD4 count in a sample. Our initial experiments suggest that it is necessary to recirculate the blood sample through the trap device in order to reach a high enough concentration of cells. Once again, we define variables for analysis of recirculation: 7 Abbas AK and Lichtman AH (2003). Cellular and Molecular Immunology (5th ed.). Saunders, Philadelphia. ISBN 0-7216-0008-5. 14 Vs = volume of whole blood sample Nt,i = number of CD4 cells remaining in the whole blood sample at the beginning of the sample’s ith pass through the trap Nr,i = number of CD4 cells captured in the trap after the sample’s ith pass through the trap fi = fraction of entering CD4 cells which were captured on pass i Using the definitions of fi, Nt,i, and Nr,i, we can write a recursive equation for fi: 𝑓𝑖 = 𝑁𝑟,𝑖 𝑁𝑡,𝑖−1 −𝑁𝑟,𝑖−1 = 𝑁𝑟,𝑖 𝑁𝑡,𝑖−1 −𝑁𝑡,𝑖−1 𝑓𝑖−1 = 𝑁𝑟,𝑖 𝑁𝑡,𝑖−1 (1−𝑓𝑖−1 ) (4) Next, assuming that the trap fraction fi is approximately constant—i.e. that trapping cells does not significantly affect the trap’s performance—then fi = fi-1 = f. Performing the recursion of Equation 4 yields 𝑓(1 − 𝑓)𝑖−1 = 𝑁𝑟,𝑖 (5) 𝑁𝑡,1 The total number of CD4 cells trapped after n passes of the sample through the device is the sum of the cells trapped by each pass. 𝑁𝑡𝑟𝑎𝑝𝑝𝑒𝑑 = ∑𝑛𝑖=1 𝑁𝑟,𝑖 = ∑𝑛𝑖=1 𝑁𝑡,1 𝑓 (1 − 𝑓)𝑖−1 = 𝑁𝑡,1 (1 − (1 − 𝑓)𝑛 ) (6) Modifying Equation 2 so that that N+ is replaced by the total number of cells trapped, we can relate the macroscopic luminance to the right-side of Equation 6: 𝑁𝑡,1 (1 − (1 − 𝑓)𝑛 ) = 𝐴ℓ𝑚 𝑎𝑐 (7) Rearranging yields 𝑁𝑡,1 𝑉𝑠 = 𝐴ℓ𝑚 𝑎𝑐 𝑉𝑠 (1−(1−𝑓)𝑛 ) (8) Therefore, the CD4 cell count of a sample of blood is given in terms of the area of the trap chamber (A), the cross-sectional area of a CD4+ cell (ac), the trapping efficiency of the device (f), the number of recirculation passes (n), and the macroscopic luminance (ℓ𝑚 ). A and ac are known quantities, n is determined by the duration of recirculation, ℓ𝑚 is measured by the 15 experiment, leaving only f to be determined experimentally. It seems plausible that f is approximately constant, but only for small values of n. Cost Considerations The cost of the CD4 counter per test is given by the detailed breakdown presented in Table 2. Table 2: Cost analysis of the point-of-care diagnostic device Item PDMS base and curing agent Sylgard 184 Anti-CD4 antibodies Europium nanoparticles Glass Slides PEEK tubing Photolithography (500k tests) Pump (500k tests) TRF Reader (500k tests) Total Amount 3g Capital Cost $0.31 Cost per test $0.31 .3ug 10uL 1 $ 0.14 $1.07 $0.12 $0.14 $1.07 $0.12 20cm 1 1 1 -- $0.40 $10 $60 $1020 $1,092 $0.04 $0.01 $0.01 $0.01 $1.71 Note that the PDMS base and curing agent are used in the making of the trap device as well as the pump. The costs of photolithography, the pump (motor and controls), and the TRF reader become negligible when their capital costs are divided by the number of tests they are expected to last: we estimate this to be about 500,000 tests. The price of the TRF reader estimated here is for a production model, rather than the prototype model used in this project. Conclusions, Recommendations, and Future Directions Significant progress toward a functional prototype for a point-of-care HIV diagnostic system has been accomplished. All of the components of the device were designed, fabricated, and tested for application in CD4 counting from whole blood samples. Thus far, protocols for microfluidic 16 pumping and recirculation, white blood cell trapping, on-chip fluorescent labeling of whole blood, and time-resolved fluorescent imaging with europium nanoparticles have been developed. With the exception of the TRF reader, current results indicate that each component of the pointof-care system is capable of meeting the design criteria proposed for a point-of-care diagnostic instrument as an affordable alternative to clinical blood testing in low-resource settings. Conjugation of europium nanoparticles to anti-CD4 antibodies and subsequent TRF analysis of whole blood remain the final steps for direct point-of-care application. Based on calibration images of nanoparticle solutions, this step may prove challenging with the current detection system. Assuming the europium fluorescence of a particular labeled cell is equivalent to the fluorescent intensity observed in the device from the conjugated europium solution, calculations suggest that 6.8% of the device area should be illuminated to reach the detection threshold. However, this assumption depends on the concentration of CD4 receptors on the lymphocytes, which must be determined experimentally with europium conjugated particles. According to these results, approximately 22700 cells must be captured; a finger-stick equivalent of 40% of CD4 WBCs in healthy patients and 150-250% in an AIDS patients. Therefore, unless the actual signal strength of europium-labeled cells is higher than the original diluted signal, a magnifying lens of at least 10x power should be added to the TRF detection system. Alternative methods for higher density WBC trapping have been proposed for future investigation but may still be insufficient for TRF detection. With an expected price of $1.71 per test, this platform is anticipated to match the target of $2 per test stipulated by global health initiatives like the Gates Foundation Challenge. Non-recurring engineering costs of the prototype system were distributed across their expected lifetime as 17 shown in Table 2. Reagents and disposable trap cartridges comprised the majority of the cost per test. The only sample preparation step is the initial loading of the blood into the PEEK tubing. Ultimately, operation with Lab-View and ImageJ will enable automated on-chip labeling and image processing capabilities. The disposable trap cartridge with a re-useable pump and imaging system is ideal for facile, affordable, point-of-care application. By containing hazardous biological samples on-chip, disposal of used chips becomes the only device-specific safety concern. Peripheral considerations for implementation of this diagnostic tool must be addressed. These include transportation and storage of antibodies, disposal of finger-pricks and used cartridges, and availability of reagents and finger-sticks. Once a complete working TRF prototype has been fabricated, the device’s ability to measure CD4 counts must be tested against conventional techniques like flow cytometry (R = 0.9). Because the test affords immediate, facile test replication, the precision can be reduced to R = 0.7 with a double positive as a clear diagnosis. Acknowledgements Our special thanks go to our project mentors Professor Kevin Seale and Professor John Wikswo, of the Vanderbilt Institute for Integrative Biosystems Research and Education, for their efforts to guide our work. In addition, we extend our sincere gratitude to Dan Morrow and Dr. Bob Buck of Gauge Scientific for providing their technical expertise in time-resolved fluorescent imaging. We also thank Loi Hoang for his help with pump operation and troubleshooting. Finally, we thank Professor Paul King for his feedback and guidance in completing our project. 18