Factors influencing carpal tunnel syndrome
advertisement

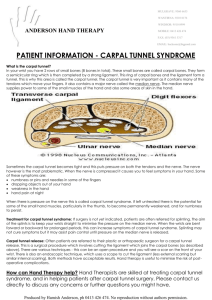
CONSULTATION DRAFT 6.5 Carpal tunnel syndrome Carpal tunnel syndrome is common during pregnancy, particularly in the third trimester. There is little evidence to support intervention in pregnancy but symptoms are likely to resolve after the birth. 6.5.1 Background Carpal tunnel syndrome results from compression of the median nerve within the carpal tunnel in the hand. It is characterised by tingling, burning pain, numbness and a swelling sensation in the hand that may impair sensory and motor function. Incidence during pregnancy • Due to differences in methods of diagnosis between studies (eg neurophysiologically confirmed, clinically diagnosed, patient-reported), there is great variability in estimates of the incidence of pregnancy-related carpal tunnel syndrome; estimates range from approximately 2% to 72% (Eogan et al 2004; Finsen & Zeitlmann 2006; Baumann et al 2007; Mondelli et al 2007; Padua et al 2010 ). Factors influencing carpal tunnel syndrome • In non-pregnant populations, carpal tunnel syndrome has been reported to occur more frequently in occupations that involve repetitive activity, forceful work or vibration (Palmar et al 2007). • In pregnancy, likely causes of carpal tunnel syndrome are hormonal changes (Ablove & Ablove 2009) and oedema (Pazzaglia et al 2005; Ablove & Ablove 2009). • Carpal tunnel syndrome is more common in the third trimester (Shaafi et al 2006; Baumann et al 2007). • Carpal tunnel syndrome is more common in women with gestational diabetes due to generalised slowing of nerve conduction (Ablove & Ablove 2009) but impaired median nerve conduction also occurs in pregnant women without gestational diabetes (Eogan et al 2004; Baumann et al 2007). 6.5.2 Discussing carpal tunnel syndrome Summary of the evidence The recent evidence on interventions to treat carpal tunnel syndrome during pregnancy is limited to small case series studies (n=20–30) that found reduced symptoms associated with night splinting (Finsen & Zeitlmann 2006) or steroid (dexamethasone) injections (Niempoog et al 2007; Moghtaderi et al 2011). Activity modification, avoiding positions of extreme flexion or extension of the wrists and avoiding exposure to vibration have been suggested as adjuncts to splinting (Mabie 2005; Borg-Stein et al 2006; Ablove & Ablove 2009) but there is no evidence that these are effective for carpal tunnel syndrome. While carpal tunnel syndrome usually resolves after the birth (Pazzaglia et al 2005), persistence of symptoms has been reported in more than 50% of women after 1 year and in about 30% after 3 years (Padua et al 2010). Consensus-based recommendation ix Advise women who are experiencing symptoms of carpal tunnel syndrome that the evidence to support either splinting or steroid injections is limited and symptoms may resolve after the birth. CONSULTATION DRAFT 6.5.3 Practice summary: carpal tunnel syndrome When: A woman has symptoms of carpal tunnel syndrome. Who: Midwife; GP; obstetrician; Aboriginal and Torres Strait Islander Health Practitioner; Aboriginal and Torres Strait Islander Health Worker; multicultural health worker, physiotherapist, occupational therapist. Provide advice: Explain that carpal tunnel syndrome is common due to increased fluid retention during pregnancy and may resolve after the birth. Discuss treatments: Explain that there is a lack of research about treatments for carpal syndrome during pregnancy and give advice on avoiding movements that may exacerbate symptoms (eg using a splint to keep the joint straight overnight). Take a holistic approach: For women whose occupations involve repetitive activity or vibration advise frequent breaks or a temporary change in role where possible. 6.5.4 Resources AAOS (2007) Clinical Practice Guideline on the Diagnosis of Carpal Tunnel Syndrome. Rosemont IL: American Academy of Orthopaedic Surgeons. http://www.aaos.org/Research/guidelines/CTS_guideline.pdf AAOS (2007) Clinical Practice Guideline on the Treatment of Carpal Tunnel Syndrome. Rosemont IL: American Academy of Orthopaedic Surgeons. http://www.aaos.org/Research/guidelines/CTSTreatmentGuideline.pdf Common discomforts in pregnancy. In: Minymaku Kutju Tjukurpa Women’s Business Manual, 4th edition. Congress Alukura, Nganampa Health Council Inc and Centre for Remote Health. http://www.remotephcmanuals.com.au 6.5.5 References Ablove R & Ablove T (2009) Prevalence of carpal tunnel syndrome in pregnant women. Wisconsin Med J 108(4): 194– 96. Baumann F, Karlikaya G, Yuksel G et al (2007) The subclinical incidence of CTS in pregnancy: Assessment of median nerve impairment in asymptomatic pregnant women. Neurol Neurophysiol Neurosci 3. Borg-Stein J, McInnis C, Dugan S et al (2006) Evaluation and management of musculoskeletal and pelvic disorders of pregnancy. Phys Rehab Med 18(3): 187–204. Eogan M, O’Brien C, Carolan D et al (2004) Median and ulnar nerve conduction in pregnancy. Int J Gynecol Obstet 87: 233–36. Finsen V & Zeitlmann H (2006) Carpal Tunnel Syndrome during pregnancy. Scand J Plast Reconstr Surg Hand Surg 40(1): 41–45. Mabie WC (2005) Peripheral neuropathies during pregnancy. Clin Obstet Gynecol 48(1): 57–66. Moghtaderi AR, Moghtaderi N, Loghmani A (2011) Evaluating the effectiveness of local dexamethasone injection in pregnant women with carpal tunnel syndrome. J Res Med Sci 16(15): 687–90. Mondelli M, Rossi S, Monti E et al (2007) Prospective study of positive factors for improvement of carpal tunnel syndrome in pregnant women. Muscle Nerve 36: 778–83. Niempoog S, Sanguanjit P, Waitayawinyu T et al (2007) Local injection of dexamethasone for the treatment of carpal tunnel syndrome in pregnancy. J Med Assoc Thailand 90(12): 2669–76. Padua L, Pasquale A, Pazzaglia C et al (2010) Systematic review of pregnancy-related carpal tunnel syndrome. Muscle Nerve 42(5): 697–702. Palmer K, Harris C, Coggon D (2007) Carpal tunnel syndrome and its relation to occupation: a systematic literature review. Occupat Med 57(1): 57–66. Pazzaglia C, Caliandro P, Aprile I et al (2005) Multicenter study on carpal tunnel syndrome and pregnancy incidence and natural course. Acta Neurochirurgica (Suppl) 92: 35–39. Shaafi S, Naimian S, Iromlou H et al (2006) Prevalence and severity of carpal tunnel syndrome (CTS) during pregnancy based on electrophysiologic studies. Shiraz E-Medical J 7(3): 1–6.