Thoracic Evaluation Form | Physical Therapy Assessment
advertisement

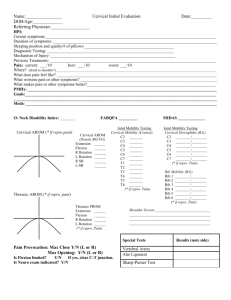
THORACIC EVALUATION FORM Patient Name Physician Therapist Eval Date DOB Next MD visit PERSONAL DATA 1. BP (sitting): _________/__________ 2. Heart Rate: __________bpm 3. Resp. Rate ______ per min Pt History of Pain/Symptoms 4. Age: 6. Onset of Sx’s Gradual 7. Pain Location 8. Pain Level 9. Pain Type Aching Dull 10. Radiating pain Yes No 11. What relieves pain/Sxs? 5. Sudden Occupation: If sudden, was there a specific event/injury? Current pain ____/10 Worst pain _____/10 Tingling Stabbing Burning Best pain Nauseating _____/10 Other: If yes, where to? (postures, movements meds, modalities) 12. What makes pain/Sxs worse? (postures,, movements, activities) 13. Does pain occurs with: Inspiration 14. Difficulty breathing? Yes Expiration Both No 15. Is the pain affected by coughing, sneezing, or straining? Yes 16. Is the condition Improving Getting worse 17. Any paresthesia or abnormal sensation? 18. Any problems with digestion? Yes 19. Any skin abnormalities in thorax area? Yes No Yes No Staying the same No If yes, where? If yes, what kind? No If yes, what kind? Other: Patient’s Goals: Observations Round back Hump back Flat back Kyphosis Razorback spine Dowager’s hump Funnel chest Barrel chest Pigeon chest Forward head Rounded shoulders Scoliosis 20. Breathing pattern: 21. Quality of respiration: 22. Effort required to inhale/exhale: 23. Coughing/Noisy/Abnormal breathing patterns?: Thoracic AROM/PROM: L L Reproduction of Symptoms: Shoulder ROM Screen L (With overpressure) Flex Flexion _____________________ Extension ___________________ R SB _______________________ L SB _______________________ R Rot ______________________ L Rot ______________________ R Flex Ext IR ER ABD HADD R ________ ________ ________ ________ ________ ________ ________ ________ ________ ________ ________ ________ Cervical ROM (i.e. full and pain-free) Flex_________________ Ext_________________ R SB________________ L SB________________ R Rot________________ L Rot________________ Ext Palpation/Soft Tissue Assessment: Thoracic Spring Testing (note if Normal, Hyper, or Hypo) T1 T2 T3 T4 T5 T6 T7 T8 T9 T10 T11 T12 Central _______ _______ _______ _______ _______ _______ _______ _______ _______ _______ _______ _______ R Unilateral _______ _______ _______ _______ _______ _______ _______ _______ _______ _______ _______ _______ L Unilateral _______ _______ _______ _______ _______ _______ _______ _______ _______ _______ _______ _______ Scapulo-Humeral Rhythm: Manual Muscle Tests Finger ABD (T1) ___________________ Abdominals _______________________ Paraspinals ________________________ Neck Extensors ____________________ Neck Lat Flexors ___________________ R Rib _______ _______ _______ _______ _______ _______ _______ _______ _______ _______ _______ _______ L Rib _______ _______ _______ _______ _______ _______ _______ _______ _______ _______ _______ _______ Cervical C1 _______ C2 _______ C3 _______ C4 _______ C5 _______ C6 _______ C7 _______ Lumbar L1 _______ L2 _______ L3 _______ L4 _______ L5 _______ Special Tests (Neurodynamic): Slump Test: _______________ T1 Nerve Root Stretch: ____________ Kernig’s Sign: _____________ Ulnar Nerve Testing: _____________ SLR: ____________________ Beevor Sign:____________________ Other: ___________________ Scapular Manual Muscle Tests Upper Trap: R________ L________ Middle Trap: R________ L________ Lower Trap: R________ L________ Rhomboids: R________ L________ Serratus Ant: R________ L________ Thoracic General Dermatomes: • T1: Medial Forearm • T2: Medial Arm • T4-6: Pain around Nipple • T7-T8: Pain in epigastriac area • T9-T11: Pain in umbilical area • T12: Pain in the groin Thoracic Manipulation Indications: • Assymetric Thoracic/Rib motion restriction (passive & active) • Point tenderness • Pain with inhalation • Acute Complaints – not long standing • Muscle guarding upon palpation • Shoulder girdle pain, but Shoulder ROM not limited • No Rib or Thoracic Spine fracture • No Manip Contraindications (Paget’s, RA, Osteomyelitis, CA, Ankylosing Spondylitis, Cord/Cauda Equina Syndrome, Vertebral Artery involved) Use Clinical Judgement to determine if Manip is Indicated (check which perfomed): • Thoracic (wedge) Manip • Rib (screw-home) Manipulation • Upper Thoracic Manipulation (Seated, hands behind neck) Audible Pop? • Yes • No Symptoms Post-Manip? _______________________ ___________________________________________ ______________________________________________ *If Manip performed, complete f/u Thoracic stretching Cervicothoracic Manipulation for Neck Pain • Symptoms <30 days • No symptoms distal to the shoulder • Looking up doesn’t aggravate symptoms • FABQ-PA <12 • Diminished upper thoracic kyphosis • Cervical Extension ROM < 30º Liklihood Manip Success: +5 or 6 = 100% +4 = 93% +3 = 86% +2 = 71% +1 = 58% CT Manip Performed? • Yes • No (seated, hands behind neck) Audible Pop? • Yes • No Symptoms Post-Manip? ___________ _______________________________ Other Possible Thoracic Issues: • Osteoporotic Wedge Fracture • Thoracic Outlet Sydrome (must have symptom recreation for positive test) • Roos Test • Adson Maneuver • Halstead Maneuver Dowager’s Hump Scheuermann’s Disease Kyphosis • Scoliosis: Convexity: ________ Levels: ____________________ • Long Thoracic Nerve Palsy • Costochondritis: most common ages 10-21, no PT Rx • T4 Syndrome: treat with T4 region mob/manip pain with deep breathing pain brought on by exercise chest pain (esp ribs 4-6) costochondral TTP UE symptoms • pain Non-dermatomal distribution Lack of hard neuro signs Headaches • yes • yes • yes • yes • no • no • no • no • parasthesia • yes • yes • yes • none • no • no • no ASSESSMENT: SHORT TERM GOALS: 1. 2. 3. LONG TERM GOALS: 1. 2. 3. PLAN: Signature___________________________________________________________ Date__________________________