SPT techniques hand-out DLL WAC 2011

Skin prick testing Techniques
Désirée Larenas Linnemann,
Pediatric allergist, Hospital Médica Sur, Mexico City
Chair Immunotherapy, Allergen Standardization and Allergy Diagnostics committee
Skin testing techniques and variability
In the allergist’s office, skin testing remains the central way to confirm allergic response.
Although anecdotal data suggest widely varying practices in skin testing by allergists, the diversity and relative frequency of these practices have only been documented in certain countries.
2 3
One of these countries has been Finland where it was noted that diagnostic practices vary greatly between different testing centers in the country. In Finland a successful national asthma program had been installed at the end of the 90ies. Building on the experiences gained with this program, in 2008 is was decided to launch a National Allergy Program (2008-2018) aimed at a reduction of the burden of allergy on the community as a whole. The plan states that allergy testing with allergens (skin prick tests, patch tests, challenge tests) will be centralized in large hospitals and in those private units which fulfill the quality requirements and in which an allergist is responsible for testing.
3 As such, this plan recognizes the importance of the standardization of allergy diagnosis.
As skin prick testing is a biologic response procedure, multiple factors can influence its outcome and interpretation. Here below we shall review some of these factors grouped under
‘Which allergens’ and ‘Which device’. However, it should be taken into account that the exact interpretation might even vary in different parts of the world, as it not only depends on the extracts and devices, but also on the genetic background of the population tested and the natural exposure. Referring once more back to the National Allergy Program in Finland, in the program includes reading keys of skin prick testing, which might be taken as an example of how to unify criteria for other countries. (Fig.1)
Proficiency testing of the personnel that applies the skin testing might be a first step to improve quality control in one’s office. The last part of this hand-out contains a proficiency test published some years back by Dr Oppenheimer 1 which could be applied for this goal. This test was used in the National Skin Test Sensitivity study in Mexico. During the workshop willing participants shall be invited to practice such a proficiency test on spot. (see addendum 1)
Which allergens to use: (see also talk Dr. Weber)
Manufacturer: potency 4-5
All are 50% glycerinated
Cross reactivity: only chose one representative of highly cross-reactive pollen families 6-8
Be aware of cross-reactivity that can be caused by phylogenetically long conserved proteins, that cause cross-reactivity between species of different plant families (profilins, 9-
11 Lipid Transfer Protein 12 )
Add local allergens 13
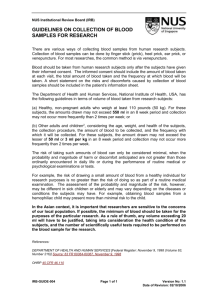
Figure 1.
Reading keys from skin testing in Finland
Legend: Examples of the reading keys of skin prick tests. The wheal diameter is illustrated on the X -axis, and the percentage of subjects suffering from actual symptoms on the Y -axis.
Allergen preparations; birch, ALK-Abello´ SQ 10 HEP (ALK-Abello´ A/S, Hørsholm, Denmark); dog, ALK-Abello´ SQ 10 HEP; peanut, in-house extract; soya bean, in-house extract. A positive skin prick test result does not equal to clinically significant allergy, it is a sign of exposure and
IgE-associated sensitization, but must be related to symptoms history. The test does not make the patient allergic, e.g. foods should not be eliminated from the diet on the basis of the test result only.
Which device
For the selection of the ideal device to be used for skin prick testing several issues have to be taken into account and materials shall be available during the workshop to get more acquainted with them. There exist a number of sharp instruments that may be used for prick/puncture tests, that can be divided .
Single prick device: lancet with or without bifurcated tip, hypodermic needle, solid bore needle
Multiple-head devices (e.g Multitest)
A comparison study of several of the mostly used devices, done by some members of the
Immunotherapy Committee of the AAAAI (Carr, et al) 14 showed statistically significant differences among all devices tested and they concluded that providers should consider this data when choosing a device that suits their practice setting Moreover it is important for the allergist to ensure that the technicians doing the skin testing are sufficiently trained on the correct use of the device.
In this study Multiple-head devices tended to give larger wheal on the lateral testing sites versus the central sites that gave smaller readings.
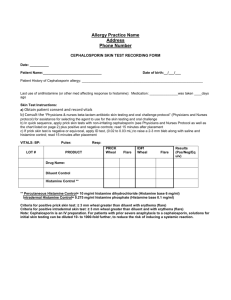
Trauma that each device produces defines the negative control wheal. It is preferably not to use devices that produce a wheal with the negative control of 4-5 mm. In the Practice parameters on Diagnostic testing a table is inserted on this subject: 15 (table 1)
Table 1. Size of Wheals That Are Larger Than 99% of the Wheals With Saline, Using the Same
Device on Subject’s Back by the Same Operator
Abbreviations: HS, Hollister Steir; Greer, Greer Laboratories; ALO, Allergy Labs of Ohio; Lincoln,
Lincoln Diagnostics; ALK, ALK America.
Devices 1 are those for which a 3-mm wheal would be significant. Devices 2 are those for which a more than 3-mm wheal should be used as significant.
References that might be useful
1. Oppenheimer J, Nelson HS. Skin testing. Ann Allergy Asthma Immunol. 2006 Feb;96(2
Suppl 1):S6-12.
2. Oppenheimer J, Nelson HS. Skin testing: a survey of allergists. Ann Allergy Asthma
Immunol. 2006 Jan;96(1):19-23.
3. Haahtela T, von Hertzen L, Makela M, Hannuksela M. Finnish Allergy Programme 2008-
2018--time to act and change the course. Allergy. 2008 Jun;63(6):634-45.
4. Larenas-Linnemann D, Esch RE, Guidos-Fogelbach G, Rodriguez-Perez N. A comparison of in vitro potency between European and Mexican allergen extracts and US (CBER/FDA) reference extracts. Allergol Immunopathol (Madr). 2010 Mar 23.
5. Larenas-Linnemann D, Matta JJ, Shah-Hosseini K, Michels A, Mosges R. Skin prick test evaluation of Dermatophagoides pteronyssinus diagnostic extracts from Europe, Mexico, and the United States. Ann Allergy Asthma Immunol. 2010 May;104(5):420-5.
6. Weber RW. Cross-reactivity of pollen allergens: impact on allergen immunotherapy.
Ann Allergy Asthma Immunol. 2007 Sep;99(3):203-11; quiz 12-3, 31.
7. Weber RW. Guidelines for using pollen cross-reactivity in formulating allergen immunotherapy. J Allergy Clin Immunol. 2008 Jul;122(1):219-21.
8.
9.
Esch RE. Grass pollen allergens. Clin Allergy Immunol. 2008;21:107-26.
Asero R, Monsalve R, Barber D. Profilin sensitization detected in the office by skin prick test: a study of prevalence and clinical relevance of profilin as a plant food allergen. Clin Exp
Allergy. 2008 Jun;38(6):1033-7.
10. Fernandez-Rivas M, Garrido Fernandez S, Nadal JA, Diaz de Durana MD, Garcia BE,
Gonzalez-Mancebo E, et al. Randomized double-blind, placebo-controlled trial of sublingual immunotherapy with a Pru p 3 quantified peach extract. Allergy. 2009 Jun;64(6):876-83.
11. Barber D, de la Torre F, Lombardero M, Antepara I, Colas C, Davila I, et al. Componentresolved diagnosis of pollen allergy based on skin testing with profilin, polcalcin and lipid transfer protein pan-allergens. Clin Exp Allergy. 2009 Nov;39(11):1764-73.
12. Schulten V, Radakovics A, Hartz C, Mari A, Vazquez-Cortes S, Fernandez-Rivas M, et al.
Characterization of the allergic T-cell response to Pru p 3, the nonspecific lipid transfer protein in peach. J Allergy Clin Immunol. 2009 Jul;124(1):100-7.
13. Arbes SJ, Jr., Gergen PJ, Elliott L, Zeldin DC. Prevalences of positive skin test responses to 10 common allergens in the US population: results from the third National Health and
Nutrition Examination Survey. J Allergy Clin Immunol. 2005 Aug;116(2):377-83.
14. Carr WW, Martin B, Howard RS, Cox L, Borish L. Comparison of test devices for skin prick testing. J Allergy Clin Immunol. 2005 Aug;116(2):341-6.
15. Bernstein IL, Li JT, Bernstein DI, Hamilton R, Spector SL, Tan R, et al. Allergy diagnostic testing: an updated practice parameter. Ann Allergy Asthma Immunol. 2008 Mar;100(3 Suppl
3):S1-148.
Addendum 1. Proficiency test for skin prick testing
The technician who will be in charge of applying the skin prick test will undergo a proficiency test for the skin prick test with histamine dihydrocloride 10mg/mL, saline and the device that will be used for the skin prick tests. The proficiency test consists of the application in an alternate pattern of histamine and saline on the forearm of a test-subject. Both, histamine and saline will be applied ten times and the mean wheal diameter will be used to calculate the coefficient of variation. This must not be greater than 20%, as calculated based on the mean diameter of the wheal.
1
The concentration of histamine used normally gives a wheal diameter of about 6mm (Range 4-
8mm acceptable). The test will be repeated until the technician passes the test. Results of each proficiency test for the skin prick test will be recorded on the proficiency test form.
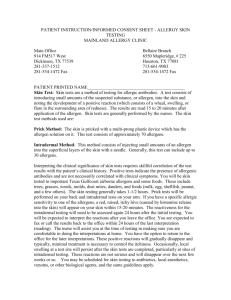
Prueba de proficiencia y control de calidad Técnica para aplicación de SPT 1
Usa la lanceta con la cual hará las pruebas, aplica control (+) (histamine 1-10) y control negativo (salina 1-10) alternando en la espalda de la persona a probar.
Anota los resultos de histamina a los 8minutos dibujando con plumón negro del estudio el contorno de la roncha.
Anota los resultados de salina a los 15 min dibujando con plumón negro del estudio el contorno de la roncha.
Usa cinta transparente para transferir las ronchas dibujadas a la parte posterior de la hoja de reporte de la prueba de proficiencia (pag.26).
Calcula el promedio de diámetro de CADA roncha X = (D + d)/2;
D = diámetro mayor y d = diámetro perpendicular a la mitad de D.
Histamina
Calcula el promedio y la desviación estándar de todos los promedios individuales X.
Determina el coeficiente de variación = desviación estándar / promedio total
El estándar de calidad es un coeficiente menor del 30%. (idealmente menor del 20%)
Salina
Todos los controles negativos tiene que ser < 3mm (roncha) y < 10mm (eritema).
Desviación estándar
Donde Σ = suma de
X = Individual mean of major and perpendicular diameter of each wheal: (D + d)/2
M = Mean of all these 10 individual means
N = Sample size (10)
Website that automatically calculates Σ: http://www.easycalculation.com/statistics/standard-deviation.php
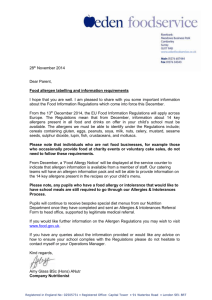
Documentation sheet for skin prick testing proficiency test
Person who applied:_______________________________ Date: __________
Device used: (dd / mm / yyyy)
Saline Histamine:
D: ____ mm d: _____mm
D = major diameter d = diameter perpendicular to major diameter
Mean of the 2:
Saline Histamine:
D: ____ mm d: _____mm
Mean of the 2:
Saline Histamine:
D: ____ mm d: _____mm
Mean of the 2:
Saline Histamine:
D: ____ mm d: _____mm
Mean of the 2:
Saline: Histamine:
D: ____ mm d: _____mm
Mean of the 2:
Saline Histamine:
D: ____ mm d: _____mm
Mean of the 2:
Saline Histamine:
D: ____ mm d: _____mm
Mean of the 2:
Saline
Histamine:
D: ____ mm d: _____mm
Mean of the 2:
Saline
Histamine:
D: ____ mm d: _____mm
Mean of the 2:
Saline MEAN
HISTAMINE
Histamine:
D: ____ mm d: _____mm
Mean of the 2:
HISTAMINE:
All Diameters
4-8mm
SALINE:
All
< 3mm
Diameters
Coeficient of variation for histamine wheals: Standard deviation / mean =
Coefficiente less than 20%:
No
Yes
; Test passed
: