disclosure and consent - Methodist Health System
advertisement

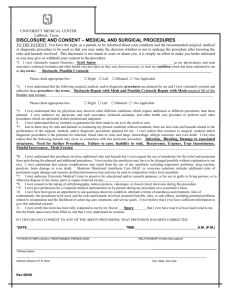
DISCLOSURE AND CONSENT Medical, Surgical and Diagnostic Procedures TO THE PATIENT: YOU HAVE THE RIGHT, AS A PATIENT, TO BE INFORMED ABOUT YOUR CONDITION, THE MEDICAL, SURGICAL, OR DIAGNOSTIC PROCEDURE(S) RECOMMENDED, AS WELL AS THE RISKS AND HAZARDS INVOLVED, SO THAT YOU CAN MAKE AN INFORMED DECISION WHETHER OR NOT TO UNDERGO THE PROCEDURE(S). THIS DISCLOSURE IS NOT MEANT TO SCARE OR ALARM YOU; IT IS SIMPLY AN EFFORT TO MAKE YOU BETTER INFORMED SO YOU MAY GIVE OR WITHHOLD YOUR CONSENT TO THE PROCEDURE(S). 1. VOLUNTARY REQUEST FOR TREATMENT: I (we) voluntarily request Dr.______________________________ as my physician, and such associates, technical assistants, and other health care providers as they may deem necessary, to treat my condition which has been explained to me as: I also grant permission for physicians in post-graduate medical education training, personnel/students of medical, nursing and other clinical training programs affiliated with Methodist Health System to participate in the procedure(s) described below. 2. PLANNED PROCEDURES: I (we) understand that the following surgical, medical and/or diagnostic procedure(s) are planned for me and I (we) voluntarily consent to and authorize these procedures: 3. 4. DISCOVERY OF OTHER CONDITIONS: I (we) understand that my physician may discover other or different conditions which require additional or different procedures than those planned. I (we) authorize my physician and such associates, technical assistants and other health care providers to perform such other procedures which are advisable in their professional judgment. 4. BLOOD TRANSFUSION: I (we) (do) (do not) consent to the use of blood and blood products as deemed necessary for this hospitalization. While blood transfusions are not risk free, the blood supply is safer today than it ever has been. I (we) also understand that the following risks and hazards may occur in connection with transfusion of blood and blood products and that the risks of transfusion may be immediate or delayed: (i) bruising or swelling at the site where the needle is inserted into the vein; (ii) fever; (iii) allergic reaction; (iv) transfusion reaction which may include kidney failure or anemia or even death; (v) heart failure; (vi) hepatitis; (vii) AIDS (acquired immune deficiency syndrome) or HIV transmission; and (viii) other infections. My physician has explained the possible use of alternative treatments, if applicable. 5. RISKS OF TREATMENT: NO WARRANTY/GUARANTEE OF RESULT OR CURE: I (we) understand that no warranty or guarantee has been made to me as to result or cure. Just as there may be risks and hazards in continuing my present condition without treatment, there are also risks and hazards related to the surgical, medical, and/or diagnostic procedure(s) planned for me. I (we) realize that common to surgical, medical and/or diagnostic procedures is the potential for infection, blood clots in veins and lungs, excessive bleeding, allergic reactions, and even death. I (we) also realize that the risks and hazards disclosed in the attached Addendum or listed below may occur in connection with this particular procedure: 6. SPECIFIC POINTS OF DISCUSSION WITH MY PHYSICIAN: The following items have been explained to Initials 03745 (12/05) Disclosure and Consent Medical, Surgical and Diagnostic Procedures 7. 8. 9. Initials 10. Initials 11. 12. me (us) by the physician. a. The nature of the proposed care, treatment, services, medications, interventions, or procedures. b. Potential benefits, risks, or side effects, including potential problems related to recuperation. c. The likelihood of achieving care, treatment, and service goals. d. Reasonable alternatives to the proposed care, treatment, and service. e. The relevant risks, benefits, and side effects related to alternatives, including the possible results of not receiving care, treatment, and services. f. When indicated, any limitations on the confidentiality of information learned from or about the patient. g. Assistants needed in the procedure to perform delegated tasks under my supervision. DISPOSAL OF REMOVED TISSUE: I (we) authorize the Hospital to use its discretion to retain or dispose of any tissue(s) removed during any operation or procedure. OBSERVATION OF PROCEDURE: I (we) consent to the admittance of observers during the operation or procedure for the purpose of medical and allied health education. PHOTOGRAPHING OR VIDEOTAPING OF PROCEDURE: I (we) (do) (do not) consent to the photographing or videotaping of the operations or procedures to be performed, including appropriate portions of my body, and the inclusion of such pictures in my medical record. In addition, I (we) consent to the use of such pictures for medical, scientific, or educational purposes, providing my identity is not revealed by the pictures or descriptive texts accompanying the pictures. ANESTHESIA RISKS: I (we) understand that anesthesia involves additional risks and hazards but I (we) request the use of anesthetics for the relief and protection from pain during the planned and additional procedures. I (we) realize the anesthesia may have to be changed possibly without explanation to me (us). I (we) voluntarily consent to use of anesthetic agents. I (we) understand that certain complications may result from the use of any anesthetic including cardiac or respiratory problems, aspiration, decreased blood pressure, nausea and vomiting, drug reactions, paralysis, nerve or brain damage or even death. Other risks and hazards, which may result from the use of general anesthetics, range from minor discomfort to injury to vocal cords, lips, teeth or eyes. I (we) understand that other risks and hazards resulting from spinal or epidural anesthetics include high block, headache, hematoma or blood clot formation, spinal cord injury, seizures, infection at the site of placement, meningitis, neck or back discomfort and chronic pain. For pregnant women, additional risks and hazards include prolonged labor, decreased fetal heart rate, fetal distress and fetal death. Alternative types of anesthesia, if applicable, have been explained to me by my physician. I (we) understand that moderate or conscious sedation may progress to deep sedation or general anesthesia. I (we) understand that anesthesia may include placement of invasive monitors with risks and hazards including bleeding, infection, lung collapse, irregular heart beat, artery or major vessel injuries, decreased blood flow, perforation of the heart or esophagus and the need for additional procedures. OPPORTUNITY TO ASK QUESTIONS: I (we) have been given an opportunity to ask questions about my condition, alternative forms of anesthesia, treatment, risks of non-treatment, the procedures to be used, and the risks and hazards involved; I (we) believe that I (we) have sufficient information to give this informed consent. CERTIFICATION – UNDERSTANDING OF CONSENT FORM: I (we) certify this form has been fully explained to me (us), that I (we) have read it or have had it read to me (us), that the blank spaces have been filled in, and that I (we) understand its contents and accept the risks and hazards. I (we) further understand and accept that additional risks and hazards may be involved. Signed Date Time Patient's Signature Signed Signed Other Legally Responsible Person's Signature Witness Signature ___ Printed Name of Other Legally Responsible Person/Relationship Printed Name of Witness _____________________________________________________________________________ Reason why patient cannot sign I certify that the patient/parent/guardian/or other legally responsible person has been provided information on the risks and hazards, benefits and alternatives to treatment as outlined above, had questions within my area of expertise answered and has given consent. ________________________________ __________________________________________ Signature of Physician performing procedure Signature of Anesthesiologist/Anesthetist administering Anesthesia/sedation Translation of document (if applicable) provided by: _____ Printed Name of Translator Agency/Department for Contacting Translator