Transfusion Medicine - UCSF Departments of Pathology and

Pearl Toy, MD
Transfusion Medicine
Transfusion support plays an increasingly prominent role in modern medical care. Blood transfusions are essential not only to save the lives of bleeding trauma victims, but also to the successful outcome of many complex treatments offered at tertiary care centers such as UCSF.
In the not-so-distant past, transfusion medicine was a relatively uncomplicated subject. “A few decades ago, there were only three kinds of blood products routinely available — red blood cells, fresh frozen plasma, and platelets,” said Pearl Toy, MD, chief of the Blood Bank in the UCSF Department of Laboratory Medicine. Now there are more than 40 different blood products to choose from, and tremendous progress has been made in the safe and effective collection, testing and storage of human blood. It is now possible to detect, and thus almost completely keep out of the blood supply, viral pathogens such as HIV, hepatitis and HTLV. Indeed, the myriad changes in how blood is processed and transfused are reflected in the fact that transfusion medicine recently became a certified medical specialty.
Leader in NIH Funding for Research
Despite these advances, however, there remains much to be learned about the biology of blood and its best clinical uses. UCSF is a leader in transfusion medicine research funding from the National Institutes of Health, with Department of Laboratory Medicine faculty serving as principal investigators on grants that each year provide millions of dollars. These awards, and a number of others, place the campus among the leading centers for transfusion-related research.
Transfusion Medicine SCCOR Grant
UCSF is one of only two medical centers in the country to have received a five-year
Specialized Center of Clinically Oriented Research (SCCOR) grant in Transfusion
Biology and Medicine from the National Heart, Lung and Blood Institute, NIH. Under the supervision of director Pearl Toy, MD, the SCCOR funds enable UCSF faculty to pursue basic and clinical research on transfusion-related acute lung injury (TRALI), currently the uncommon but leading cause of transfusion-associated mortality.
SCCOR grant project leaders include (1) Pearl Toy, MD, Department of Laboratory
Medicine, who is studying the incidence and risk factors associated with TRALI, (2)
Michael Gropper MD, PhD, Department of Anesthesia, who is mild lung injury associated with transfusion, (3) Michael Matthay MD and Mark Looney MD, Department of Medicine, who are studying TRALI in a mouse model, and (4) Clifford Lowell, MD,
PhD, Department of Laboratory Medicine chair, who is studying basic mechanisms of neutrophil activation. In addition, there are important collaborations with Mayo Clinic, the Blood Centers of Pacific, the American Red Cross, and the Harvard School of Public
Health.
Blood Systems Research Institute (BSRI)
In addition to the SCCOR grant, several research studies conducted under the leadership of Michael Busch MD, PhD at the Blood Systems Research Institute on Masonic Ave in
San Francisco are contributing important insights into transfusion biology and safety.
These include studies related to microchimerism, HTLV, HCV, and TRALI.
Microchimerism
Microchimerism is the existence of cells or tissues from one individual within another.
While this has been known to happen with cell and organ transplantation, and with pregnancy, investigators at BSRI, UC Davis and UCSF are among the first to define this phenomenon as it occurs following blood transfusion. The research team, headed by Dr.
Michael P. Busch MD, PhD at BSRI, has recently reported the occurrence of high-level transfusion-associated microchimerism (TA-MC) in patients receiving transfusion for severe traumatic injury. About half of these patients have detectable chimerism when they are discharged from the hospital and, while most loose the chimeric population of donor cells from their peripheral blood over the following months, about 1 in 5 has an expansion in the donor cell population to the point where the cells from a single blood donor comprise as much as 2-3% of all the trauma victim’s circulating leukocytes. This happens at a similar prevalence whether or not the transfused products were leukoreduced. The donor cells include various lymphocyte phenotypes (CD-4, CD-8,
CD-19, and CD-15) and appear to be less reactive toward the recipient than control lymphocytes. The investigators have not yet documented TA-MC in clinical populations other than trauma patients and the reasons the phenomenon occurs in trauma patients is under intensive investigation. Current thinking is that the immune perturbations associated with severe injury are necessary but not sufficient for TA-MC to occur.
During late 2006, Busch’s team received a grant from the National Heart Lung and Blood
Institute to expand studies of TA-MC. The goals of the new research include determining whether TA-MC represents a clinically harmful consequence of blood transfusion, whether other clinical populations (such as elective surgical patients or burn patients) may also be affected by TA-MC. The investigators are also working to identify the immunologic mechanisms that permit the establishment and maintenance of TA-MC and whether TA-MC represents true hematopoietic engraftment, or some lesser form of cellular expansion and persistence. Dr. Busch’s team is also beginning important
collaborations with the military where the use of very fresh blood in severely injured soldiers may predispose to TA-MC and perhaps to previously unrecognized related complications of transfusion among injured soldiers such as transfusion-associated graft versus host disease.
HTLV Outcomes Study (HOST)
HOST is a multi-center prospective cohort study led by Dr. Edward Murphy and studies the health outcomes of chronic infection with HTLV-1 and HTLV-2. A total of
151 HTLV-1 and 387 HTLV-2 infected humans were recruited from seropositive blood donors in 1988 through 1992. A group of 799 seronegative controls, matched on age, sex, race/ethnicity, blood center and donation type was recruited at the same time to allow comparison of health outcomes with an appropriate control group. Every two years, subjects are seen by nurse/counselors who perform a health interview, a screening physical examination, and phlebotomy for complete blood count and repository specimens for research testing.
Recent published findings from the cohort include an increased incidence of pneumonia, bronchitis, urinary tract infections and asthma among HTLV-2 infected subjects, and arthritis in both HTLV-1 and HTLV-2 infected subjects. After a median follow-up of 10.4 years through Visit 6, there have been 71 deaths in the cohort, and we have reported significantly increased mortality among HTLV-2 subjects (Hazard ratio =
2.4, 95% CI 1.4-4.1), and non-significantly increased mortality among HTLV-1 subjects, both compared to the seronegative control group.
REDS-2
The Retrovirus Epidemiology Donor Study (REDS) is a multi-center epidemiological study of blood safety funded by research contracts from the National
Heart, Lung and Blood Institute. Dr. Edward Murphy and Dr. Michael Busch have been involved in the first period of this study (REDS-1) since its inception in 1989. In 2004,
NHLBI announced a request for proposals for a second study, referred to as REDS-2, and
UCSF/BSRI was awarded one of six clinical center contracts effective September 2004
To date, proposal development for several REDS-2 research projects has included: studies of HLA and WBC antibodies in donors, iron and hemoglobin metabolism in donors (Cable), molecular surveillance of Transfusion Transmitted Infections, and a survey of donor knowledge, attitudes and behavior regarding Transfusion Transmitted
Infections.
HCV Mortality Study
The HCV Mortality Study is retrospective cohort study funded by a R01 Grant to
Drs. Michael Busch and Edward Murphy. Approximately 10,000 HCV seropositive blood donors identified within the Blood Systems network from 1991 through 2001 were matched with an equal number of HCV seronegative blood donors according to age, gender, blood center and zip code. The entire database of about 20,000 blood donors, was forwarded to the U.S. Public Health Service National Death Index (NDI). NDI matched these data against their national death certificate database to determine vital status of all participants, and cause of death for subjects who are deceased. Data analysis compared overall mortality, as well as cause specific mortality, between the HCV and control groups. Finally, a questionnaire survey of living cohort members will compare morbidity (liver and other diseases) medical care and treatment, and risk behaviors between the HCV+ and HCV- subjects.
HCV Case Control Study
This project is funded by the same NIH R01 grant above. It represents a case control study to analyze the epidemiologic and immunologic associations with clearance of HCV viremia. Cases are 150 HCV seropositives who are negative in nucleic acid testing, recruited from the 15% to 20% blood donors with these screening lab results at the time of blood donation. Controls (N=300) are both seropositive and nucleic acid positive for HCV, and are matched on age and sex to the cases. Viral load, immunologic response and host genetics will be compared between cases and controls.
Clinical Care
Without life-sustaining transfusion support, many technically challenging treatments and surgical procedures would not be possible. Patients who undergo orthopedic surgery, bone marrow or organ transplantation, or cardiothoracic surgery frequently use large amounts of blood products. It is not unusual, for example, for patients undergoing complex spine surgery to require replacement of an entire blood volume (approximately
10 units in an adult).
UCSF transfusion medicine specialists oversee all aspects of the use of blood products, from donor screening to managing transfusion reactions. Because blood transfusion has such a high public profile, the collection, testing and infusion of blood is closely regulated by governmental and professional organizations. Every procedure in the technical preparation of a blood product is regulated by agencies such as the Food and
Drug Administration (FDA), the State of California Health and Welfare Agency, the Joint
Commission on Accreditation of Hospitals Organization (JCAHO), and the American
Association of Blood Banks (AABB).
The flow of blood products through the institution is outlined below.
The robot "Madonna" reduces cost for the
Blood Bank by delivering blood for nonemergency transfusion. “She” pushes elevator buttons electronically, gets in and out of elevators, and delivers blood to the wards at the UCSF Medical Center.
Donor Center
Approximately 80% of the blood used at UCSF comes from the Blood Centers of the
Pacific (formerly Irwin Memorial Blood Bank). The remaining 20% of blood used at
UCSF is obtained from UCSF Moffitt-Long Donor Center. Donors have their vital signs checked and complete an extensive, confidential questionnaire to determine whether they are suitable donors. The actual donation process is quite quick—approximately 10 minutes for a whole blood one-unit donation, or 1.5 hours for a platelet pheresis. Blood center staff provide a psychological oasis as well as technical expertise. Giving blood through a directed donation to a critically ill loved one can provide great comfort and satisfaction to family and friends who may otherwise feel there is little they can do to help the patient.
Processing Laboratory
After collection in the UCSF or UCSF/Mount Zion donor center, blood is delivered to the blood bank processing laboratory at China Basin. Whole blood units are leukoreduced
(white cells are removed) and processed into red blood cells and fresh frozen plasma.
Concurrently, blood samples are sent to the testing laboratories.
Testing Laboratories
Samples of all donated blood go to the blood bank and Blood Systems Laboratory. Over a two-day period, the blood is tested for blood group and Rh type, as well as for infectious diseases such as HIV, hepatitis B and C, HTLV, syphilis, and Chaga’s disease. If test results are negative, blood is labeled and stored in the blood bank’s freezers, refrigerators or in room-temperature holding tanks for subsequent use. Although much of blood preparation uses time-tested tools — pipettes, microscopes and centrifuges — there are some highly mechanized aspects. The modern equipment can automatically perform
ABO Rh testing and antibody screening on large batches of blood samples. In addition, the blood bank has its own robot, “Madonna,” which delivers blood products to the clinical floors.
Selecting a Blood Product
Because blood products are a limited resource, their use must be carefully managed.
Transfusion medicine specialists help medical staff and housestaff select blood products to use in particular situations. Special requirements for blood products have moved far beyond ABO blood type and Rh status. Blood must, for example, be CMV-safe, or irradiated for certain immunosuppressed recipients.
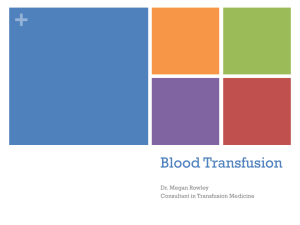
Units transfused in 2006 from blood banks at the UCSF/Mt. Zion Medical
Center, under the direction of Pearl
Toy, MD, Ashok Nambiar, MD and
Andrew Leavitt, MD; SFGHMC, under the direction of Eberhard Fiebig, MD; and the SFVAMC, under the direction of Elizabeth St, Lezin MD.
UCSF 43,052
Mt. Zion 2,272
SFGHMC 13,200
SFVAMC 4,848
TOTAL 63,372
Monitoring Recipient Reactions
Although serious complications are quite rare, transfusion medicine specialists are called upon on a daily basis to provide clinical advice for patients who have experienced reactions to blood products.
Teaching Transfusion Medicine
Because transfusion medicine is a relatively new specialty (25 yrs), there is a need to provide training opportunities for clinical care and research. Transfusion medicine is an essential part of resident and medical student training. The laboratory medicine residents rotate through the blood banks and donor centers at the UCSF Medical Center, SF
General Hospital Medical Center and the SF Veterans Affairs Medical Center, where they are exposed to all aspects of transfusion medicine, ranging from clinical issues such as obtaining a blood product for an alloimmunized recipient, to deciding whether a prospective donor’s use of a prescription medication should prevent her from giving blood.
Since 2000, UCSF has offered a one-year clinical fellowship in transfusion medicine.
During this year, the fellow participates for six months in activities in the Blood Donor and Transfusion Center, designed to develop skills in determining donor acceptability, donor testing and counseling, and in the use of various blood bank products. The remaining six months are spent at Moffitt-Long Hospital, where the fellow is exposed to a range of transfusion service related consults and operational issues. The Fellow serves as an educational resource to laboratory medicine residents and technologists, and interacts with the physicians and nurses on the clinical services. After the clinical year, fellows may design a research program.