Community-TEP-Guideline-July 2014
advertisement

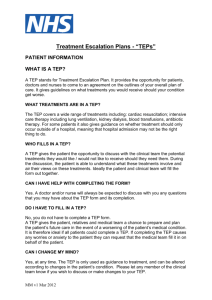
Treatment Escalation Plans (TEPs) and Resuscitation Decision Records July 2014 SCOPE This guideline relates to care of the adult patient It applies across the health sector from the Acute Trust to the Community Hospital, to the Nursing Home, to the Hospice and into the patient’s own home. GUIDELINE STATEMENT It is always a Health Professional’s duty to act in a patient’s best interests. All treatment and care that is appropriate for a patient will be offered. For the vast majority of patients the over-riding aim is to return them to their pre-illness level of health, or as near to it as possible. Nevertheless, it is not an appropriate goal of medicine to prolong life at all costs with no regard to its quality or the burdens of treatment on the patient. Moreover, to begin a therapeutic intervention that the patient will clearly not survive is not in their best interests. This implies that not all treatment modalities are appropriate for every patient. Clearly, there will be instances when a clinical decision has been made that a patient is dying, and will go on to die within hours or days. It now becomes paramount to ensure the comfort of the patient, and to be sure that the patient understands what is happening and plans for their future treatment. For all patients we must ensure that appropriate resuscitation policies which respect patients' rights are in place, understood by all relevant staff, and accessible to those who need them. Moreover, all patients should have a clear and explicit resuscitation plan. The General Medical Council guidance, Treatment and care towards the end of life: good practice in decision making (1), acknowledges that the most difficult and sensitive decisions in end of life care are often those around starting, or stopping, potentially life-prolonging treatments such as CPR (CardioPulmonary Resuscitation). However, such decision making remains MM Aug 2014 important, the results of which could be recorded as part of advance care planning. Engaging patients in advance care planning, where they are willing, puts them back at the centre of their care. The importance of such an approach is recognised in the Royal College of Physicians 2009 guide to Advance care planning (2), which states “At the core of current health and social care are efforts to promote patientcentred care, offer choice and the right to consent to or refuse treatment and care offered……… Advance care planning may help…”. The NHS End of Life Care Strategy stipulates that all people approaching the end of life need to have their needs assessed, their wishes and preferences discussed and an agreed set of actions reflecting the choices they make about their care recorded in a care plan (3). This guideline is two fold in its remit. Firstly outlining the Treatment Escalation Plan (TEP) and, secondly through application of the TEP across all health sectors in Devon to ensure continuity across the health community. The TEP is where all appropriate treatment options for the patient are laid out with a note made of those modalities which may be inappropriate. This will be discussed with the patient early in their illness as some may deteriorate and as such may not have capacity to make specific decisions about future life sustaining treatments. It will also be reviewed and updated as circumstances change. The TEP should be initiated and completed in any of the possible healthcare settings (acute or community). Implicit is the need for anticipation by clinical staff to identify those patients that despite active medical treatment have the potential to deteriorate to the point of needing resuscitative interventions. If the patient lacks capacity to participate in decision making, a Lasting Power of Attorney (where one exists) and the family and next of kin should be engaged. PROCEDURE When is it appropriate to consider making a TEP? This will vary according to local policy. Some Acute Trusts already have a policy of inclusion of all patients. However, as a minimum if a patient is at foreseeable risk of clinical deterioration and/or cardiac or respiratory arrest TEP documentation needs to be considered. It is these patients that have the potential to deteriorate to the point of potentially needing resuscitative interventions. By resuscitative interventions we mean treatment modalities such as antibiotics, intravenous fluids, blood transfusions, ventilatory support, inotropy/vasopressor therapy, renal replacement therapy and CPR. The TEP will be the form which will be the documentation of those resuscitative interventions which are and are not appropriate for the individual patient. One way of identifying this group of patients is by the use of the surprise question, “Would you be surprised if this patient died within the next 6–12 months?” For those where the answer is ”no” the TEP should be completed MM Aug 2014 for patients across the health community. If the answer is “yes” then a TEP may still be appropriate although the expectation would be that the answer would be “yes” to most or all treatment modalities outlined on the form. The patient’s physical location should not be a bar to this process. One crucial question to be addressed in the TEP is: “Is admission to an acute hospital appropriate?” The Second Annual Report of the End of Life Care Strategy suggests that many people are still needlessly sent to hospital to die simply because care home staff do not know what else to do. We should be making every effort to decrease that figure (5). Discussions with patients and relatives/carers/friends Discussions will usually be between an appropriate doctor and the patient and/or family/next-of-kin. It may be that senior nursing staff will also be able to undertake such discussions. The names and relationships of those involved in the discussions must be noted. More detailed description of such discussion should be recorded in the clinical notes where appropriate. Where competent patients are at foreseeable risk of clinical deterioration (including cardiorespiratory arrest) attending clinical staff will undertake sensitive discussions regarding their treatment plan. The Tracey ruling (6) stipulates this. The only reason not to have these discussions is if in doing so the patient will suffer harm. If patients indicate that they do not wish to discuss these issues then this should be respected. Where a TEP is completed and there has been no discussion with the patient because he or she has indicated a clear desire to avoid such discussion, this must be documented in the health records. The onus is upon clinical staff to inform patients regarding the likely survivability following commencement of any particular resuscitative intervention, and what the burdens and benefits of intervention entail. The TEP form is designed to be the template for a positive discussion beginning with the less invasive treatment modalities that will be offered but perhaps concluding with those more invasive treatment measures that would not be in the patient’s best interests, and therefore not offered. The emphasis is on those treatments that will be offered. The National End of Life Care Programme Route To Success (7) asks us to ensure that there is a communication system in place to keep all members of the multidisciplinary team across all sectors fully informed of decisions relating to TEP. The aim is that the TEP will travel with the patient and is therefore available wherever the patient may be in the health community. Where is the TEP form to be filed? The completed form must travel with the patient no matter where they are in the health community. A copy of the original must be kept in the relevant clinical notes. MM Aug 2014 The current development of centralised computer databases (such as End of Life Registers) will allow appropriate filing of the TEP in these databases allowing access for Healthcare professionals working across all sectors of the health community. Incapacitated adults, TEP, ACP, PPC and ADRT If the patient is incapacitated then their nearest relative or carer should be involved in any decision with regard to resuscitation as they may be able to give pointers as to what the patient would have wanted. Failing this an Independent Mental Capacity Advocate (IMCA) must be consulted under the terms of the Mental Capacity Act 2005 (8). Alternatively, the patient may have already indicated their wishes in an Advance Care Plan (ACP), Preferred Priorities of Care (PPC) form or Advance Decision to Refuse Treatment (ADRT). An ACP or PPC form outlines the patient’s wishes in case of clinical deterioration. They are not legally binding and are advisory to the actual care given. This is distinct from an ADRT. If valid and applicable, and signed by the patient, the ADRT is legally binding. Moreover, under the terms of the Mental Capacity Act (8), if the patient has made a Lasting Power of Attorney for health and welfare to make healthrelated decisions on their behalf, that person must be consulted. A Welfare Attorney may be able to refuse life-sustaining treatment on behalf of the patient if this power is included in the original Lasting Power of Attorney. In England, people close to patients are not legally entitled to give consent to medical treatment on behalf of an adult who lacks decision making capacity, nor can they insist on treatment or non-treatment. Doctors have authority to act in their patients’ best interests where consent is unavailable. The TEP (like previous DNR (Do-Not-Resuscitate) forms) is not legally binding. It is a signpost to the care to be given – clinical judgement will still take precedence. In decision making, relatives and others close to the patient should be involved and their views on what the patient would want taken into account. They should be made aware that although they are contributing information to inform the decision making process, they are not responsible for the decisions made. Responsibility The responsibility for completion of the TEP rests with the most senior clinician currently in charge of the patient’s care, although they may delegate the task to another person who is competent to carry it out. Wherever possible, a decision should be agreed with the whole healthcare team. MM Aug 2014 If there is genuine doubt or disagreement about the contents of the form further senior clinical opinion(s) should be sought (9). In the acute Trust the critical care team may be invaluable in such discussions. Consensus amongst all those involved in the decision making process is the aim. Where agreement on anticipatory treatment decisions cannot be reached, a note should be made of the reasons. Documenting discussions and factors to consider can be helpful in the event of clinical deterioration where no firm advance decision or TEP has been made. The Dying Patient Clearly, there will be instances when a medical decision has been made that a patient is dying, and will go on to die within hours or days. At this stage the need for interventions such as analgesia, relief of distress, hydration, nutrition and other medications will need to be reviewed. An appropriate TEP should now be completed, as well as consideration of initiating your local end-of-life pathway (for example the Liverpool Care of the Dying Pathway). Organ donation It may be appropriate that patient and family wishes regarding organ / tissue donation after death are ascertained and documented. Staff need to establish if the patient has previously expressed the wish to be a donor; and if the patient is on the NHS Organ Donor register or carries a Donor Card. Please refer to your organisation’s guidelines relating to organ donation. Written information regarding TEP available to patients Written information should be available for patients and their families. Patients should be encouraged to see such information as a routine part of their care planning to cover all contingencies rather than an intimation of particular risks to themselves. Information should reassure patients of their central role in the decision making processes involved in relation to the completion of a TEP. It should make clear that for many patients the question of acting on the decisions documented may not arise. Patients requiring further information should be supported to access this via members of the multidisciplinary healthcare team or their local patient advice and liaison services. MM Aug 2014 Review of the TEP Decisions concerning TEP must be reviewed in the light of any changes in: the patient’s clinical condition their expressed wishes Similarly, decisions concerning TEP may need to be reaffirmed: whenever the patient is transferred from one healthcare setting to another whenever the patient is admitted from home or discharged home. To cancel a TEP form cross it through diagonally stating: • Cancelled • Date • Clinician’s Name and Signature Raising staff awareness of the TEP Staff will have access to educational resources on the use of the TEP which is aimed at outlining their appropriate use. See www.tepdevon.co.uk Review and development This guideline will be regularly reviewed as a result of patient feedback and NHS Directive. Local audit and evaluation will be undertaken. Appendix – TEP FORM MM Aug 2014 References 1. General Medical Council. Treatment and care towards the end of life: good practice in decision making. May 2010. 2. Royal College of Physicians of London. Advance care planning. Concise Guidance to Good Practice series, No 12. February 2009. http://www.rcplondon.ac.uk/pubs/contents/9c95f6ea-c57e-4db8-bd98fc12ba31c8fe.pdf Accessed 28th June 2009. 3. NHS End of Life Care Strategy. Promoting high quality care for all adults at the end of life. Department of Health, London. July 2008; Page 12, section 14. 4. http://www.southcentral.nhs.uk/wp-content/uploads/2010/09/ElectronicDNACPR-Form.pdf Accessed 25th August 2011. 5. The Second Annual Report of the End of Life Care Strategy, Department of Health. London, August 2010. National End of Life Care Programme. The route to success. Department of Health. London, 2010. 6. http://www.bailii.org/cgibin/markup.cgi?doc=/ew/cases/EWCA/Civ/2014/822.html&query=Tracey+and+v+an d+Cambridge&method=boolean#disp32 7. National End of Life Care Programme. Improving end of life care. The route to success in end of life care – achieving quality in acute hospitals. Department of Health. London, 2010. 8. Mental Capacity Act 2005. http://www.dca.gov.uk/menincap/legis.htm. Accessed 19th June 2009. 9. British Medical Association, Resuscitation Council UK, Royal College of Nursing. Decisions relating to cardiopulmonary resuscitation: a joint statement from the British Medical Association, the Resuscitation Council (UK) and the Royal College of Nursing. 2007. www.resus.org.uk/pages/DNAR.htm. Accessed 19th June 2009. MM Aug 2014