an elevated triglyceride:hdl-c ratio is strongly associated with
advertisement

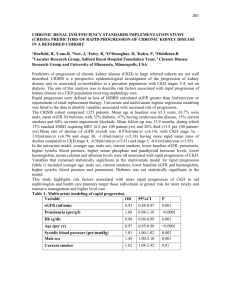
P124 AN ELEVATED TRIGLYCERIDE:HDL-C RATIO IS STRONGLY ASSOCIATED WITH CHRONIC KIDNEY DAMAGE - PROTEINURIA AND AN EGFR < 60 ML/MIN/1.73 M2. Davies, J1, Goldsmith, D2, Crook, M2, Wierzbicki, A2 1 King’s College London, 2Guy’s and St Thomas’ Hospitals, London INTRODUCTION: The prevalence of chronic kidney disease (CKD) stages 3-5, defined as eGFR < 60 ml/min/1.73 m2 is 8%1,2. Reduced GFR, and proteinuria are associated with accelerated renal dysfunction. There are several well established risk factors for the development and progression of CKD, however whether dyslipidaemia is a significant contributory factor is not clear. It is known that the triglyceride / HDL-C ratio (TG:HDL-C) is an accurate predictor of future CVD and of the insulin resistant state. We investigated the incidence of raised TG:HDL-C in patients with proteinuria and an eGFR < 60 ml/min/1.73 m2 measured on one occasion at our large tertiary referral lipid clinic in 2008. METHODS: 1283 patients attended the clinic in 2008, of which 1029 had complete serum lipid and renal profiles. eGFR was calculated for these patients using the 4 variable MDRD formula 2. We compared the incidence of an elevated TG:HDL-C defined as values ≥ 1.55 (derived from National Cholesterol Education Program guidelines3) between those with an eGFR < 60 ml/min/1.73 m2 (CKD stage 3-5) and ≥ 60 ml/min/1.73 m2 and between proteinuric (albumin creatinine ratio > 2.4 mg/mmol or urinary protein level > 0.06 g/l) and non proteinuric patients. Nephrotic range proteinuria was found in only 11 subjects. We also compared those with a combination of both CKD (stage 3 to 5) and proteinuria with “healthy” individuals suffering from neither. The incidence of ACEi ± ARB and statin treatment was calculated for each group. P values were calculated using the chi squared test. RESULTS: The prevalences of CKD and proteinuria were 11.18% and 19.42% respectively; 4.76% had both. The incidence of a TG:HDL-C ratio ≥ 1.55 was 47.83% and 34.91% in low (n=115) vs. normal (n=914) eGFR groups (p = 0.0066) and 50.50% in proteinuric (n=200) vs. 32.93% in non proteinuric (n=829) groups (p < 0.0001). In patients with both low eGFR and proteinuria (n=49), 65.31% of which were treated with ACEi ± ARBs, 51.02% had a TG:HDL-C ≥ 1.55 vs. 31.85% among. “healthy” (n=763) individuals (p = 0.0057), 36.96% of which were ACEi ± ARB treated (p = 0.0001). There was a uniform incidence of statin treatment across all groups (between 63.48% and 66.50%). CONCLUSION: Using a large patient database of 1,029 patients from a tertiary referral lipid clinic it is clear that CKD and proteinuria are common. The TG:HDL-C ratio is strongly associated with key renal functional parameters, and thus may be a target for future therapeutic intervention. SHARP-2 will help define the rationale for intervention with statins. References: 1. National Collaborating Centre for Chronic Conditions. Chronic kidney disease. Early identification and management of chronic kidney disease in adults in primary care and secondary care. Nice clinical guideline 73(2008). 2. Coresh J, Stevens L, Levey A. Chronic kidney disease is common: What do we do next? Nephrology Dialysis Transplantation (2008) 23: 1122–1125. 3. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) Final Report. Circulation (2002) 106: 3143.


![Risk Adjustment Factor [RAF]](http://s2.studylib.net/store/data/005748329_1-97f04b2983127ae4930cafa389444167-300x300.png)