Lit Review - Regis University: Academic Web Server for Faculty
advertisement

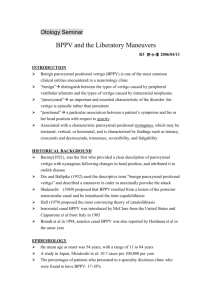
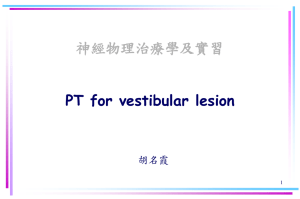
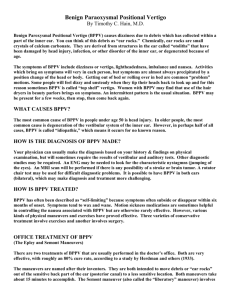
Literature Review Supporting a Minimum Data Set for the Diagnosis and Treatment of Benign Paroxysmal Positional Vertigo Nicole Miranda, PT, MPT Faculty Advisors: Amy Stone Hammerich, PT, DPT Julie Whitman, PT, DScPT Regis University Advanced Clinical Decision Making DPT 740 June 10, 2008 Background Information Benign Paroxysmal Positional Vertigo (BPPV) is a syndrome characterized by brief episodes of a spinning or vertiginous sensation which is often precipitated by head motion in the vertical or horizontal planes. Each episode is described as an ‘attack’ where a combination of vertigo, dizziness, unsteadiness and/or nausea can last for days to months with the possibility of recovering as spontaneously as it began. BPPV is frequently seen in emergency departments, with high cost for unnecessary diagnostic testing and interventions due to poor identification of signs and symptoms as the average BPPV patient reportedly consults with four physicians and incurs costs of up to $2000 with no positive findings or resolution of symptoms.1,2 The prevalence of BPPV is relatively unknown due to the lack of recognition by primary care providers and epidemiology studies which have been largely conducted in specialized care settings.3 A population-based study performed at the Mayo Clinic in Minnesota indicated a .06% incidence of BPPV, with a 38% increase incidence with each decade of life.4 Other population-based questionnaires have found that 20-30% of adults report a rotational dizziness as a primary medical complaint.5 The increased prevalence of BPPV in women than men (2:1) may be associated with higher prevalence of migraine in women.3 The syndrome is characterized by an ‘active phase’, during which spontaneous vertigo attacks typically occur for days or weeks, or even months in chronic conditions. The subsequent ‘inactive phase’ ranges from no symptoms to a persistent sense of mild to moderate insecurity or abnormal sensations associated with instability.6 The mechanism of action in BPPV continues to be debated. Schuknecht7 initially proposed the concept of cupulolithiasis, where otolithic particles are released from the utricle and become lodged on the cupula of the posterior semicircular canal. The weight of the otoconia causes deflection of the cupula in response to change in gravitational pull with altered head position, which results in nystagmus. An alternative theory of canalithiasis postulates that free-floating otolithic debris moves within the endolymphatic fluid of the semicircular canals in response to changes in head position and the force of gravity.8 2 BPPV is idiopathic in approximately 50% of cases, with secondary BPPV being associated with head trauma, and inner ear disorders such as vestibular neuritis, labyrinthitis, vestibular migraine and Meniere’s Disease.3 Recurrence of BPPV has been found to be higher in cases associated with head trauma and in females.9,10 The highest recurrence rate has been found in the first year, at 80%; while recurrence rates are less than 5% after 5 years.10 Variant Forms of BPPV The posterior/inferior semicircular canal is affected in approximately 96% of cases of benign paroxysmal positional vertigo.11 The posterior canal is the most often affected canal as it is the most dependent organ in both supine and upright positions, which allows the otlithic debris to move through the canal with respect to gravity.12 Failure to resolve BPPV with standard repositioning maneuvers has led to further studies investigating variant forms of BPPV which occur in both the lateral/horizontal and anterior/superior canals. Pictorial diagram of otoconia displaced in the posterior semicircular canal.13 Horizontal canal variant of BPPV affects 2-15% of those with BPPV.14,15 Individuals suffering from horizontal canal BPPV frequently complain of symptoms with rolling over in bed and have increased reports of nausea and vomiting associated with vertigo. White, 3 et al.14 reported that Dix-Hallpike testing alone does not adequately identify BPPV of the horizontal canal, clarifying the need for supine testing for assessment of persons with BPPV. The anterior canals are the least often affected canals due to their superior position and the relative inability of the otolithic debris to travel against gravity. Schratzenstaller, et al.12 reviewed 3 case studies using high resolution 3D MRI and concluded that canalithiasis of the anterior canal can occur if structural changes have occurred in the lumen of the anterior canal, creating an adhesive endothelium, and if there is a filling defect visible on HR-3D-MRI due to a solid structure in the anterior canal. Proper diagnosis and determination of which semicircular canal(s) are involved is imperative for selection of intervention techniques. Failure to resolve BPPV with customary repositioning maneuvers often indicates a chronic or persistent case of vertigo, and may be an indication for further medical management. Statement of Purpose South Valley Physical Therapy, P.C. has implemented a protocol for treatment of persons with BPPV in an effort to determine success and failure in the resolution of BPPV via physical therapy intervention, and to facilitate a team approach with physicians who manage complicating factors associated with vertigo. According to this protocol, failure to clear the BPPV through the use of repositioning maneuvers after 3 physical therapy visits results in notification of the referring physician of a case of ‘persistent BPPV’ and to indicate the possible need for further medical work-up. Referral back to the MD may lead to alterations in medications or diagnostic testing such as MRI to rule out a neuroma or structural abnormality within the semicircular canals. If a patient returns to physical therapy with no positive findings or changes in medication, ductolithiasis may be suspected and the patient begins a 4-week program of cranial oscillation. Ductolithiasis has been described by Zappia and Becvarovski16 as a build up of particles causing blockage of the endolyphatic duct, which causes reduced flow of 4 endolymphatic fluid and hydrops. Following four weeks of cranial oscillation the BPPV episode is either cleared by resumed flow of endolymphatic fluid and opening of the duct, or further consultation with the MD is indicated. Cases involving failure to cure the BPPV episode require further differential diagnosis, which makes a team approach and effective communication imperative to allow one to return to previous life activities. The purpose of this project is to create a Minimum Data Set (MDS) and data collection form to clinically analyze whether the above described protocol provides effective management and resolution of BPPV. The data will be collected and assessed according to the canal(s) involved and whether intervention includes repositioning maneuvers, habituation exercises, sleeping precautions, cranial oscillation and /or medical intervention. The length of time to resolve BPPV and whether or not further vestibular rehabilitation is indicated will also be recorded for assessment of clinical outcomes. Diagnosis The Dix-Hallpike Test is the ‘gold standard’ for diagnosis of BPPV.17,18 The test consists of moving a person from long sitting to supine with the head turned 45 degrees to one side and the neck extended 20-30 degrees. The supine position, with neck rotated and extended, is maintained for 30-60 seconds to observe any nystagmus. A positive test results when paroxysmal positional nystagmus is observed. Right Dix-Hallpike Test13 5 The direction of the nystagmus and the side to which the head is rotated indicate the canal involvement in BPPV. In posterior canal BPPV, during a right Hallpike test nystagmus occurs in a clockwise direction; whereas during a left Hallpike test posterior canal involvement is indicated when the nystagmus is appreciated in a counterclockwise direction. Anterior canal BPPV can be detected on Dix-Hallpike testing with the presence of counterclockwise nystagmus during right Hallpike testing or clockwise nystagmus on left Hallpike testing.19 BPPV associated with cupulolithiasis reportedly causes symptoms when the head is hanging below the horizon, which causes deflection of the cupula of the posterior canal.19 Vertigo symptoms and nystagmus should occur immediately upon placing a person in the provocative position and should persist the entire time the position is maintained, as the cupula remains deflected in the dependent position. Canalithiasis is suspected if there is a latency period of 1-40 seconds after moving into the provoking position followed by an increase and subsequent decrease in both nystagmus and vertigo sensation that extinguishes within 60 seconds.19 A Roll Test is commonly used to diagnose horizontal canal involvement in BPPV.19 During the Roll Test the person is brought back in to a supine position with the head flexed 20 degrees. Upon reaching the supine position, the head is rotated quickly toward one side with observation for the presence or absence of nystagmus. The head is then brought back to midline and quickly turned to the opposite side. A positive test results with the presence of nystagmus in the geotropic (toward the ground) or ageotrophic (away from the ground) direction. Geotrophic nystagmus will typically fatigue and indicates canalithiasis, while ageotrophic nystagmus will be persistent due to suspected cupulolithiasis.19 Treatment Interventions and Efficacy Intervention for BPPV consists of habituation exercises and repositioning maneuvers that were developed in an effort to return the otoconia to the utricle. The Semont, or ‘liberatory’ maneuver is characterized by a brisk movement from one sidelying position 6 to the opposing sidelying position, with the head turned 45 degrees out of the plane of the body with either nose up or nose down depending on the canal involved. The brisk motion is thought to dislodge the debris from the cupula in cases of cupulolithiasis for either anterior or posterior canal BPPV. The Epley20 maneuver, often referred to as the canalith repositioning procedure (CRP), was designed to move particles from the semicircular canal back to the utricle by moving a person through a series of positions to push the debris through the affected posterior or anterior canal. The original Epley maneuver involved use of mastoid oscillation and premedication with vestibular suppressants. Modified versions of the Epley (CRP) are now performed with exclusion of mastoid oscillation due to lack of evidence to support vibration or medication usage assisting in resolution of BPPV.21,22,23 Many retrospective and prospective RCTs as well as meta-analyses of these studies have been conducted to investigate the efficacy of repositioning techniques. The Epley Maneuver13 White et al.24 conducted a meta-analysis to asses the efficacy of repositioning maneuvers in the treatment of posterior canal BPPV as compared to untreated controls. Nine RCTs with a total of 505 patients were reviewed. The risk of persistent BPPV without treatment reduced from 69% to 28% after a single canalith repositioning maneuver, with an absolute risk reduction of 41%. The number needed to treat (NNT) was 2.38 to achieve a favorable outcome using repositioning maneuvers to treat posterior canal 7 BPPV. Tusa and Herdman25 similarly reviewed RCTs and found a 67-89% response rate to the Epley or liberatory maneuvers as compared to a 0-48% response rate with no treatment or sham treatment. They also reported 8-14% of patients who had ongoing imbalance after resolution of BPPV, requiring further intervention. Complications associated with failure to resolve BPPV of the posterior canal include conversion to the horizontal canal or anterior canal as described by Herdman and Tusa.26 Recommendations were published more recently to reduce conversion of posterior canal BPPV to other semicircular canals.25 The recommendations include: 1) performing repositioning maneuvers on a tilt table that ensure head tilt of at least 20 degrees into extension, 2) instruction in horizontal head motion a few times every hour while awake to avoid cervical stiffness, and 3) to sit still for at least 2 minutes after treatment and for 10 minutes prior to leaving the clinic to avoid nausea and emesis associated with severe vertigo. BPPV affecting the horizontal canal requires repositioning maneuvers in the plane of the horizontal canal. The technique most often used is the Lempert or Barbecue rotation of 360 degrees. The patient begins in sitting with the head turned to the affected side. The patient is moved to supine, maintaining the 90 degree head rotation. The person is then slowly rolled in 90 degree segments until 360 degrees have been completed. Each position is typically held 15-30 seconds, and then the person returns to sitting avoiding any cervical extension. A recently published retrospective study determined the efficacy of the Barbecue maneuver to cure horizontal canal 74% following one maneuver, and 85% after a maximum of 3 rotations.27 While an objective finding of nystagmus is the hallmark for a positive test, subjective complaint of vertiginous symptoms or nausea during Dix-Hallpike testing without visualization of nystagmus is not uncommon. This would be considered a positive test with ‘non-classic’ presentation due to the lack of objective findings of nystagmus, and is often termed ‘subjective vertigo’. Despite lack of objective test findings, Haynes et al.28 reported a response rate of 86% to an average 1.13 liberatory maneuvers to treat vertigo 8 without nystagmus. This is consistent with findings of Weider et al.29 and Tirellia et al.30, who found 76% and 93% response to repositioning procedures respectively for subjective vertigo. Patients are typically advised to sleep with the head slightly elevated by using one 1-2 extra pillows, to avoid lying on the affected side and to limit head movement for 24-48 hours following repositioning maneuvers. These sleep and activity precautions are recommended to allow the canalith debris to settle into the utricle and to keep the particles out of the semicircular canals. However, activity restrictions and sleep precautions have not been shown to alter the effectiveness of CRP maneuvers.31 Cranial oscillation is a newer intervention that is not well researched and has only been introduced in the literature by Zappia and Becvarovsk.16 The technique was developed to mimic the vibration induced during endolymphatic sac surgery based on a hypothesis that otolithic particles were causing an obstruction of the endolymphatic duct, termed ductolithiasis. The authors performed cranial oscillation on 10 patients and studied the short-term effects on vertigo, imbalance, hearing, aural pressure and tinnitus. Vertigo was resolved in all patients who had vertigo symptoms, and 80% remained clear at the 3 month follow-up.31 While no further clinical trials have been published to date, the ZBMOP technique has been used successfully in the protocol presented in this paper. The most recent review of practice parameters performed by the Quality Standards Subcommittee of the American Academy of Neurology32 assigned Level A recommendations for use of the CRP in treatment of posterior canal BPPV, based on two Class I and three Class II studies that reported resolution of symptoms using the CRP with NNT between 1.43 and 3.7. The Semont maneuver was given a Level C recommendation based on only one Class II study. Only Class IV studies have been conducted regarding treatment of horizontal canal and anterior canal BPPV, with a Level U recommendation, or no specific recommendation, regarding specific selection of repositioning techniques. Fife, et al.32 further determined:1) there was insufficient evidence available to determine the efficacy of post-treatment restrictions with use of 9 CRP, 2) use of mastoid oscillation in the treatment of posterior canal BPPV was determined not to influence response to CRP with Level C recommendations, 3) CRP was more effective than use of Brandt-Daroff exercises for treatment of posterior canal BPPV (Level C recommendation), and 4) there is no available evidence supporting the use of medication to treat BPPV. Outcome Measures Multiple outcome measures have been studied in vestibular rehabilitation to determine balance and fall risk as well as gait stability. The following section discusses the rationale behind the selection of the 5-item subscale of the Dizziness Handicap Inventory, the Timed Up & Go and the Dynamic Gait Index as outcome tools for the BPPV MDS. These outcomes tools will be analyzed alongside the subjective report of perceived dizziness and nausea via analog scales and the report of falls. Resolution of BPPV will be determined with negative Dix-Hallpike and Roll Tests, while the below described outcome measures should help identify those in need of further intervention to reduce imbalance following BPPV. Dizziness Handicap Inventory The Dizziness Handicap Inventory (DHI) was developed by Jacobson and Newman in order to quantify the perceived handicap in persons with vestibular disorders.33 The questionnaire contains 25 items divided into nine functional, seven physical and nine emotional categories, with possible responses of “yes” (4 points), “sometimes” (2 points) and “no” (0 points). Higher scores reflect increased perceived dizziness, with a possible total score of 100 points. Test-retest reliability was found to be high, r=0.97, by Jacobson and Newman. They determined an 18 point change would be significant to indicate an effect from intervention with a 95% confidence interval that was not specifically revealed in their publication. The DHI has been used to study the efficacy of vestibular rehabilitation and the impact of dizziness on one’s quality of life.34,35,36 The DHI is frequently utilized in the clinical setting to assess response to treatment in vestibular rehabilitation.37 10 A more recent study has identified specific items of the DHI which indicate an increased likelihood of a diagnosis of BPPV.38 A 5-item BPPV subscale of the DHI was created as a tool to assist physicians in the diagnosis of BPPV. The subscale items include looking up, difficulty getting out of bed, quick head movements, rolling over in bed and bending. A response of “yes” on all 5 items, with a total score of 20 points produced a likelihood ratio of 2.29.38 The specificity of a subscore of ≥ 18 was 93.8% and the sensitivity of a subscore of 0 was 97.6%.7 The estimated OR for the BPPV subscore was 1.07 (95% CI, 1.02-1.13; p<0.01), with odds in favor of BPPV of 0.13 with a subscore of 0, and an increase in OR by approximately 15% with each two-point increase in the subscore.7 Further analysis by Whitney et al. revealed a two-item subscale, consisting of getting out of bed and rolling over in bed, which produced a LR of 2.61 with a score of 8 on the two items.38 Because the DHI has specific items correlated with the diagnosis of BPPV, the DHI will be used to assess perceived handicap and reduced participation in life activities. In an effort to reduce the length of time needed to complete the full DHI at each visit, the 5-item subscale will be used to specifically track items associated with BPPV. Timed Up and Go The Timed Up and Go (TUG) is a gait assessment tool developed to assess fall risk in the elderly population with multiple co-morbidities.39 The test consists of rising from a chair, walking forward 3 meters, turning 180 degrees and returning to sit in the chair at a comfortable walking speed. Scores of ≥ 13.5 seconds have been related to risk of falls in the elderly population.40 In studies using the TUG, the chair seat to floor height and armrest height are standardized. Whitney et al. looked at the sensitivity and specificity of the TUG and DGI for selfreported falls in 93 subjects with vestibular disorders.41 The specificity of the TUG at 11.1 seconds was 56%, with a PPV of 46% and NPV of 85%. The OR in favor of falling with a TUG of >11.1 seconds was 5.0 (95%CI 1.80-13.91). The time of 11.1 seconds was selected as the best cut-off to identify risk for falling in persons with vestibular 11 disorders due to the higher sensitivity that was found previously at a cut-off of 13.5 seconds. The TUG is an ideal test in the clinic for assessing gait speed in conjunction with rising from a chair, where the head may tip forward or backward, and incorporates a change in direction via 180 degree turn. Persons with BPPV typically refrain from movements that cause fluid to move within the semicircular canals, which would likely cause an increase in TUG score. While there is ongoing research being done to assess the psychometric properties of various measures for gait stability and fall risk, the Timed Up & Go appears to have the best ability to identify risk of falls in persons with vestibular disorders, and is a standard measure by which to compare outcome measures in current literature. Dynamic Gait Index The dynamic gait index (DGI) was originally developed by Shumway-Cook42 to assess postural stability during gait in adults over 60 years of age at risk of falling. The DGI consists of 8 gait activities, such as walking with head motion, which are rated on a 4point ordinal scale with a lower score indicating increased impairment. A score of <19 has been identified as the cut off for identifying risk of falls in older adults.43 In a study looking at the reliability of clinical measures used in vestibular rehabilitation, Hall and Herdman17 determined excellent inter-rater reliability of the DGI in persons with peripheral vestibular disorders at k= 0.64 and ICC of 0.86. Whitney et al.44 investigated the correlation between self-reported falls in 6 months and the DGI with an odds ratio of 2.58 (95% CI 1.47-4.53) in favor of falls with a DGI score of <19. Further analysis revealed an OR of 2.38 (95%CI 1.53-5.26) in favor of falls in subjects with vestibular dysfunction who were >65 years of age, and an OR of 3.55 (95% CI1.43-8.87) for those 65 or younger. In 2004 Whitney et al.41 related the TUG and DGI to self-reported falls, as cited above. The sensitivity of the DGI score of <19 was 71% and the specificity was 53%. The PPV was 39% and the NPV 81% for a score of <19. The odds ratio in favor of falling with a DGI score of <19 was 2.66 (95% CI 1.08-6.57). 12 The DHI, TUG and DGI will be used in this clinical analysis alongside the patients’ perceived dizziness and nausea as rated on a visual analog scale. Additionally, individuals will report the number of falls between visits and during the 6 months prior to initial evaluation. The Tinetti definition for falls will be use for consistency with the definition used by the Medicare Fall Prevention Act, which states that a fall is “a sudden, unintentional change in position causing an individual to land at a lower level, on an object, the floor, or the ground, other than as a consequence of sudden onset of paralysis, epileptic seizure, or overwhelming external force.”45 The combination of self-report scales and outcome measures should reflect the impact of BPPV on one’s ability to function independently without loss of balance or instability of gait as well as measure the ability to perform routine life activities. Conclusion Current literature supports the use of repositioning maneuvers to effectively treat benign paroxysmal position vertigo, especially related to the more common posterior canal involvement. Proper identification of the canal involved greatly affects selection of repositioning maneuvers and ultimately success in clearing BPPV. Failure to respond to repositioning within three physical therapy sessions has been hypothesized as an indicator for an atypical case of BPPV that may require alternative intervention via either cranial oscillation or medical work-up. A Minimum Data Set for physical therapy intervention in cases of BPPV would both guide practitioners in utilizing the current best evidence to treat BPPV and determine the number of maneuvers and number of sessions needed to clear specific types of vertigo. An MDS would also identify individuals with resistance to repositioning maneuvers and cases of persistent vertigo that may require further medical diagnosis and/or intervention. Utilization of the proposed MDS for BPPV in the clinical setting will allow analysis of current clinical practice and modification of the proposed protocol for treatment of BPPV. 13 1 Chang AK, Schoeman G, Hill MA. A randomized clinical trial to assess the efficacy of the epley maneuver In the treatment of acute benign positional vertigo. Academic Emergency Medicine. 2004;11:918-924. 2 Li JC, LiDJ, Epley J, Weinberg. Cost-effective management of benign positional vertigo using canalith repositioning. Otolaryngol Head Neck Surg. 2000;122:334-339. 3 Neuhauser HK, Epidemioloty of vertigo. Curr Opinion Neurol. 2007;20:40-46. 4 Froehling DA, Silverstein MD, Mohr DN, Beatty CW, Oxford KP, Ballard DJ. Benign positional vertigo: incidence and prognosis in a population-based study in Olmsted County, Minnesota, Mayo Clin Proc. 1991;66:596-601. 5 Kroenke K, Price RK. Symtpoms in the community. Prevalence, classification and psychiatric comorbidity. Arch Intern Med. 1993;153:2474-2480. 6 Giannoni G, Vannucchi P, Pagnini. Definition and classification of paroxysmal positional vertigo. Audiological Medicine. 2005;3:4-6. 7 Schuknecht HF. Cululolithiasis. Arch Otolaryngol. 1969;90:113-126. 8 Hall SF, Ruby RRF, McClure JA. The mechanics of benign paroxysmal positional vertigo. J Otolaryngol. 1979;8:151-158. 9 Gordon, CR, Levite R, Joffe V, Gadoth N. Is posttraumatic benign Paroxysmal positional vertigo different from the idiopathic form? Arch Neurol. 2004;61:1590-1593. 10 Brandt T, Huppert D, Hecht J, et al. Benigh paroxysmal positional vertigo: a long-term follow-up (6-17 years) of 125 patients. Acta Otolaryngol. 2006;126:160-163. 11 Honrubia V, Baloh RW, Harris MR, et al. Paroxysmal positional vertigo syndrome. Am J Otol. 1999;20:465-470. 12 Schratzenstaller B, Wagner-Manslau C, Strasser G, Arnold W. Canalolithiasis of the superior semicircular canal: an anomaly in benign paryoxysmal vertigo. Acta Oto-Laryongologica. 2005;125:10551062. 13 Hain TC. Benign Paroxysmal Positional Vertigo Available at: http://www.dizziness-andbalance.com/disorders/bppv/bppv.html. Accessed on May 23, 2008. 14 White JA, Coale KD, Catalano PJ, Oas JG. Diagnosis and management of lateral semicircular canal benign paroxysmal positional vertigo. Orolaryngol Head Neck Surg. 2005;133:278-284. 15 Escher A, Ruffieux C, Maire R. Efficacy of the barbecue manoeuvre in benign paroxysmal positional vertigo. Eur Arch Otorhinolaryngol. 2007;264:1239-1241. 16 Becvarovski Z, Zappia J, The ZB mastoid oscillation protocol (ZBMOP) in meniere’s disease and ductolithiasis. Otolaryngol Head Neck Surg. 2002;127:491-492. 17 Hall CD, Herdman SJ, Reliability of clinical measures used to assess patients with peripheral vestibular disorders. J of Neurol Phys Ther. 2006;30:74-81. 18 Dix MR, Hallpike CS. The pathology, symptoms and diagnosis of certain common disorders of the vestibular system. Ann Otol Rhinol Laryngol. 1952:61:987-1016. 19 Herdman SJ, Tusa RJ. Benign Paroxysmal Positional Vertigo. In: Herdman SJ, ed. Vestibular Rehabilitation. Second Edition. Philadelphia, PA. FA Davis Co., 2000:451-470. 20 Epley JM. The canalith repositioning procedure: For treatment of benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg. 1992;107:399-404. 21 Hain TC, Jelminshi JO, Reis IL, et al. Vibration does not improve results of the canalith repositioning procedure. Arch Otolaryngol Head Neck Surg. 2000;126:617-622. 22 Macias JD, Ellensohn A, Massingate S, Gerkin R. Vibration with the canalith repositioning maneuver: a prospective randomized study to determine efficacy. Laryngoscope. 2004;114:1011-1014. 23 McClure JA, Willett JM. Lorazepam and diazepam in the treatment of benign paroxysmal vertigo. Journal Otolaryngol. 1980;9:472-477. 24 White J, Savvides P, Cherian N, Oas J. Canalith repositioning for benign paroxysmal positional vertigo. Otology & Neurology. 2005;26:704-710. 25 Tusa RJ, Herdman SJ. BPPV: Controlled trials, contraindications, post-maneuver instructions, complications, imbalance. Audiological Med. 2005;3:57-62. 26 Herdman SJ, Tusa RJ. Complications of the canalith repositioning procedure. Arch Otolaryngol Head Neck Surg. 1996;122:281-286. 27 Escher A, Ruffieux C, Maire R. Efficacy of the barbecue manoeuvre in benign paroxysmal vertigo of the horizontal canal. Eur Arch Otorhinolaryngol. 2007;264:1239-1241. 14 28 Haynes DS, Resser JR, Labadie FR et al. Treatment of benign positional vertigo using the semont maneuver: efficacy in patients presenting without nystagmus. Laryngoscope. 2002;112:796-801. 29 Weider DJ, Ryder DJ, Stram JR. Benign paroxysmal positional vertigo; analysis of 44 cases treated by the canalith respositioning procedure of Epley. Am J Otol. 1994;15:321-326. 30 Tirelli G, D’Orlandao E, Giacomarra V, Russolo M. Benign positional vertigo without detectable nystagmus. Laryngoscope. 2001;111:1053-1056. 31 Massoud EA, Ireland DJ. Posttreatment of benign paroxysmal positional vertigo: no need for postmaneuver restrictions. J Otolaryngol. 1996;25:121-125. 32 Fife TD, Iverson DJ, Lempert T, Furman JM, Baloh RW, TUsa RJ, Hain TC, Herdman S, Morrow JM, Gronseth GS. Practice parameters: Therapies for benign paroxysmal positional vertigo (an evidence-based review). Neurol. 2008;70:2067-2074. 33 Jacobson GP and Newman DW. The development of the dizziness handicap inventory. Arch Otolarygol Head Neck Surg. 1990;116:424-427. 34 Cowand JL, Wrisley DM, Walker M, Strasnick B, Jacobson JT, Efficacy of vestibular rehabilitation. Otolaryngol Head Neck Surg. 1998;118:49-54. 35 Lopez-Escamez JA, Gamiz MJ, Fernandez-Perez A, Gomez-Finata M, Sanchez-Canet I. Impact of treatment on health-related quality of life in patients with posterior canal benign paroxysmal positional vertigo. Otol Neurotol. 2003;24:637-641. 36 Gamiz J, Lopez-Escamez. Health-related quality of life in patients over sixty years old with benign paroxysmal positional vertigo. Gerontology. 2004;50:82-86. 37 Fielder H, Denholm SW, Lyons RA, Fielder CP. Measurement of health status in patients with vertigo. Clin Otolaryngol. 1996;21:124-126. 38 Whitney SL, Marchetti GF, Morris LO. Usefulness of the dizziness handicap inventory in the screening for benign paroxysmal positional vertigo. Otology & Neurology. 2005;26:1027-1033. 39 Podsiadlo D, Richardson S. The timed up and go: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;671;387-389. 40 Shumwas-Cook A, Brauer S, Woollacott M. Predicting the probability of falls in the communitydwelling older adults using the timed up & go test. Phys Ther. 2000;80: 79-84. 41 Whitney SL, Marchetti GF, Schade A, Wrisley DM. The sensitivity and specificity of the timed “up & go” and the dynamic gait index for self-reported falls in persons with vestibular disorders, J Vestib Research. 2004;14:397-409. 42 Shumway-Cook A, Woollacott M. Motor Control Theory and Applications. Williams and Wilkins Baltimore, 1995. 43 Shumway-Cook A, Bladwin M, POlissar NL, Bruber W, Predicting the probability for falls in community-dwelling older adults. Phys Ther. 1997;77:812-819. 44 Whitney SL, Hudak MT, Marchetti GF. The dynamic gait index relates to self-reported fall history in individuals with vestibular dysfunction. J Vest Research. 2000;10:99-105. 45 Tinetti ME, Speechley M, Ginter SF. Risk factors for falls among elderly persons living in the community. N Eng J Med. 1998;319:1701-1707. 15