congenital angular limb deformity of the carpus in a foal
advertisement

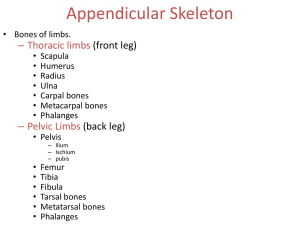
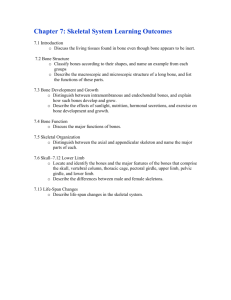
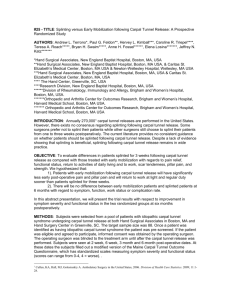
ISRAEL JOURNAL OF VETERINARY MEDICINE VOLUME 55 (2) 2000 CONGENITAL ANGULAR LIMB DEFORMITY OF THE CARPUS IN A FOAL: A REPORT OF A COMPLICATED CASE AND REVIEW OF LITERATURE A. Steinman1, G. Klemer1, O. Levi1, G. Avni1 and E. R. Singer2 1. Koret School of Veterinary Medicine, The Hebrew University of Jerusalem P.O.B. 12, 76100 Rehovot, Israel. 2. Division of Equine Studies, University of Liverpool, Leahurst, Chester High Road, Neston, South Wirral L64 7TE, UK Abstract Successful treatment of a severe and complicated case of angular limb deformity in a foal is reported. The diagnosis, treatment and prognosis of angular limb deformities of the carpal joint are discussed. Introduction Angular limb deformities (ALDs) are commonly observed in foals (1). The most common location of ALDs is the carpal joint, where valgus deformities predominate (2-4). ALDs cause abnormal biomechanical loading of joints that may lead to secondary deformities of the affected or the adjacent joints (5). Early diagnosis and treatment of ALDs is essential to prevent these secondary changes and maximise the potential for correct conformation. During the last few years the equine industry in Israel has gone through marked development with a dramatic increase in the population of sport horses. Whereas limb angulation and deviation in breeds used for pleasure riding is tolerable, the same deformities are not accepted in horses intended for high level competitions (6). The requirement for good conformation will make the diagnosis and treatment of ALDs more important in Israel in the near future. Case Report A 9 day old Quarter Horse colt was referred to the Koret School of Veterinary Medicine, Veterinary Teaching Hospital (KSVM-VTH) for evaluation of a severe angular limb deformity. The foal had been born 20 days before the expected foaling date with a bilateral carpal valgus deformity. The foal had been treated with stall rest without any improvement in the condition. On admission, severe valgus deformity was noticed in both carpal joints. Diagnosis The left carpal joint was mildly unstable and was affected more severly. Radiographs were taken of both carpal joints, which revealed incomplete ossification of the carpal bones. The left carpal joint had a deviation angle of 200 with the point of intersection at the distal epiphysis, almost in the radiocarpal joint. The cuboidal bones of the carpus appeared rounded with large radiolucent spaces between, indicating a lack of mineralisation of the cartilage template of these bones. This abnormality was particularly evident in the ulnar, second and fourth carpal bones. The proximal extent of MCII and MCIV appeared hypoplastic (Fig 1). The right carpal joint had a deviation of 4 . 0 Figure 1. A dorsopalmar radiograph of the left carpus at 8 days. Angle of deviation is 200. The cuboidal bones of the carpus appear rounded with large radiolucent spaces between, indicating a lack of mineralization of these structures, particularly the ulnar and second and fourth carpal bones. The proximal extent of the MCII and MCIV also appear hypoplastic The more severely affected left fore carpal joint was splinted using well-padded polyvinyl chloride splints that were replaced every 48 hours in order to prevent pressure sores. The right fore carpus was more stable and straight than the left and was not splinted. When the foal was 2 weeks old, superficial digital flexor tendon contraction developed with a flexural deformity of the metacarpophalangeal (MC-P) joint of the right leg. Three grams of oxytetracycline were administered intravenously once; however, this did not seem to improve the condition. Short hand walks were started which improved the condition after a week. However, a few days later, tendon laxity of the left fore leg developed and a wedge pad was used in order to raise the heels. Additional radiographs of both carpal joints were taken following two weeks of stall rest, when the foal was 3 weeks old. Minimal improvement of the left carpal joint deviation was noticed with the angle of deviation measuring 170, a decrease of 30. There was increased mineralisation of the carpal bones that appeared less round and less immature (Fig 2). At 4 weeks, due to lack of improvement of deviation angle with conservative treatment, a hemicircumferential periosteal transection and periosteal elevation was performed on the lateral aspect of the radius, just proximal to the distal radial physis. One week after the surgery, radiographs were taken which revealed some improvement in the angle of deviation of the left carpal joint. At the same time varus deformity of the right fetlock joint was noticed, and a shoe with a lateral extension was put on that leg in order to evenly distribute the forces on the limb. The foal was discharged from the clinic with instructions for stall rest and corrective trimming and shoeing. The foal was examined again at the KSVM-VTH when he was 3 months old, 8 weeks following the periosteal elevation. The left front carpus appeared almost straight, with an angle of deviation of 40. Mineralisation of the carpal bones appears to be proceeding normally with a more cuboidal appearance (Fig 3). The right fore fetlock joint still had a varus deformity with lateral-medial laxity of the joint. This deformity was treated with a hemicircumferencial periosteal transection and periosteal elevation on the distal medial right fore third metacarpal bone. This joint was splinted for one week following surgery, using well-padded polyvinyl chloride splints in order to provide stability. The splints were then replaced by a heavy bandage in order to allow more weight bearing to prevent flexural deformity. About 4 weeks after the second surgery, the fetlock joint of the right leg appeared stable. The bandages were taken off and the amount of exercise was increased gradually. When the foal was 5 months old his fore limbs were almost straight. However, he was stiff and was not moving freely, with enlargement of the distal metacarpal and metatarsal bones at the level of the physis. Based on these clinical findings and additional radiographs, physitis was diagnosed. Treatment included restricted exercise, low doses of phenylbutazone and a decrease in the amount of concentrated feed the foal received. Four months later, when the foal was 9 months old his legs were straight and he was moving freely without lameness. Figure 2. Figure 3. A dorsopalmar radiograph of the left carpus at A dorsopalmar radiograph of the left carpus at 3 months. Angle of deviation is 40. 3 weeks. Angle of deviation is 17 . The cuboidal bones of the carpus appear less Mineralization of the carpal bones rounded indicating an increase in the degree of appears to be normal mineralization. 0 Literature Review Etiology The etiology of angular limb deformity of the carpal joints appears to be complex and multifactorial. Several etiologies have been suggested including intra-uterine malposition, overnutrition of the mare, joint laxity, defective endochondral ossification (hypoplasia) of the cuboidal bones, or abnormal development of the second and fourth metacarpal bones (7). Ingestion of toxins by pregnant mares, and endocrine or metabolic imbalances such as hypothyroidism (8), have also been suggested (9). Diagnosis Although angular limb deformity of the carpal joints is usually evident on physical examination, the exact location of the deformity should be determined by radiographs. Premature or dysmature foals will be more likely to have joint laxity and/or hypoplastic cuboidal bones than a foal carried to term. A term foal is more likely to develop an ALD as a result of abnormal growth. The progression of the angular deformity will influence the decision regarding therapy. The deformity may have been present at birth with either improvement or deterioration in the following weeks to months. The presence of lameness in the affected leg or in the opposite leg may provide information about the etiology. The foal should be examined in motion to evaluate the change in the degree of angular deformity with weight bearing and to observe any signs of lameness. Palpation for heat, pain, swelling and laxity should be performed (7). In order to select the correct therapy and to determine the prognosis, dorso-palmar and lateral-medial radiographs are required. Two methods of assessment of radiographs are available. Assessment of ALD based on determination of the pivot point has long been an accepted method of determining the center of the deviation of the limb. The pivot point is the intersection point of lines drawn to bisect the radius and third metacarpal bone. The angle at which these lines intersect is the degree of angulation (10). Brauer et al. (1999) suggest that this method may not be reliable if there is more than one site of deviation in the carpus. These authors suggest a second method of assessing carpal valgus by measuring the angle of deviation at the physis and at each of the individual carpal joints. This has the advantage of dividing the total deviation into its component parts and allows a quantitative comparison of the angles of deviation at each level (4). This is done by drawing a horizontal line through each joint space and the distal radial physis. In a straight leg all lines should be perpendicular to the longitudinal axis of the third metacarpal bone (9). Treatment The treatment selected depends on the severity and the location of the deformity, as well as the age of the foal (9). In many cases, foals born with mild ALDs correct spontaneously in the first few days to weeks of life. This is attributable to improved muscle tone and coordination with strengthening of ligamentous laxity (9). In mild-to-moderate cases (less than 10 degrees) with normal ossification of carpal bones, stall confinement with periods of controlled exercise is recommended (11). Regardless of additional treatments, regular corrective trimming is important (9). Simply balancing and leveling of the foot on a biweekly basis is recommended. More aggressive hoof manipulation that causes excessive unbalancing of the foot may worsen the problem (8). Foals with incomplete ossification of the cuboidal bones should be stall rested for 14-21 days or until ossification is complete. Repeat radiographs are essential to determine if ossification is progressing normally. In most foals, mineralization is complete within 2 weeks of birth (5). If the angle of deviation of the joint is more than 10 degrees with accompanying incomplete ossification of the carpal bones the leg should be supported externally with a splint or a tube cast. The external support used for the carpus should extend from elbow to the distal metacarpus, but not beyond the fetlock (11). More aggressive therapy is indicated if the degree of deformity is severe, not improving or worsening (5). Two surgical procedures can be used to correct ALDs, either a hemicircumferential periosteal transection and elevation or transphyseal bridging. A hemicircumferential periosteal transection and elevation stimulates bone growth and is performed on the concave, or shorter side of the limb. A transphyseal bridge is a growth retardation surgery performed on the convex, or longer side of the limb (5). Description of the surgical techniques is beyond the scope of this article and the reader is referred to other sources (2,3,8). Surgical treatment is based on a natural growth correction mechanism. Cells of the physis that are loaded more heavily grow faster and those loaded less heavily, grow more slowly within physiologic limits. Accelerated growth of the more heavily loaded cells is stimulated only during dynamic loading where the pressure is applied intermittently. Static loading retards growth. Reduction of static compression allows cells to accelerate their growth and is the principle behind hemicircumferential periosteal transection. Release of the periosteum is thought to decrese the compression of the area. An increase in static compression retards growth because the cells are compressed above their pathological limit. This is the principle behind the transphyseal bridging (6). Surgical treatment of carpal ALDs should be performed when the foal is between 6 weeks and 4 months of age. This is recommended, because the most rapid rate of longitudinal growth occurs in the first 3-4 months. In comparison, the rapid rate of longitudinal growth of the distal metacarpus/metatarsus is complete by 5-6 weeks, necessitating earlier surgical intervention. Continual asymmetric loading of the carpal and fetlock joints can lead to osteoarthritic changes in the long term (3). Prognosis Predicting an accurate prognosis may be difficult and requires repeated radiographs of the affected leg. The prognosis for foals with incomplete ossification of the cuboidal bones depends on the degree of changes in the joint. If no permanent change has occurred, such as crushed carpal bones, the prognosis is good. If radiographic changes are already visible in the carpal joints, the prognosis for athletic use is guarded (12). Athletic performance was reduced in foals treated surgically at 2 or more anatomic sites, compared with foals treated at only the distal part of metacarpal/metatarsal bone III or the radius (13). Generally, the greater the number of abnormalities observed distal to the distal radial physis and the more distal the pivot point, the poorer the prognosis (7). Discussion The diagnosis in the case described in this article was of incomplete ossification of the cuboidal bones, accompanied by carpal valgus. Incomplete ossification of the cuboidal bones is usually identified in premature or dysmature foals (5). Carpal valgus is the most commonly observed deformity associated with this pathology (12). A few days after birth, when restricted exercise did not seem to improve the carpal valgus and laxity, splints were used on the more severely affected left fore leg because collateral ligament laxity was present (11). The splint which was used was placed to stabilise the carpal joint while allowing the foot to continue bearing weight. This allowed for strengthening of the collateral ligaments without creating tendon laxity (11). Splints should be used with care since they are known to cause complications such as development of decubitus sores, potential worsening of the joint laxity and increased flexor tendon laxity (8). Indeed, several tendon problems occured during treatment which were attributed to restriction of exercise, uneven weight-bearing, and rapid rate of growth. Superficial digital flexor tendon (SDFT) contraction did not respond to treatment with oxytetracycline which is proported to chelate calcium ions rendering them unavailable for use for striated muscle contraction (14). A gradual increase in exercise improved the condition. Flexor tendon laxity that developed 2 weeks later was treated by raising the heels to increase the load on the SDFT. Treatment of the tendon laxity may have been unnecessary, since it is usually a self-limiting problem (5). Carpal valgus of the right leg responded well to conservative treatment of stall rest. This can be attributed to improved muscle tone and coordination, with strengthening of the collateral ligament laxity (9). Improvement of the left carpal valgus was not sufficient with conservative therapy, and a decision for surgical correction was made. Although the origin of the deviation was located in the carpal joint rather than the distal radial physis, the foal underwent hemicircumferencial periosteal transection and periosteal stripping of the distal lateral radius. This procedure has been shown to result in correction of carpal valgus even when the deviation is at multiple sites within the joint (4). The explanation may be that by compensating at the level of physis, axial compressive forces realign throughout the joint, thereby stimulating remodeling and more normal growth of the carpal bones (10). The varus deformity of the opposite fetlock joint that developed after surgery, is thought to have resulted from excessive weight-bearing on this limb. Treatment with lateral shoe extension was performed to redistribute axial stresses by encouraging the foot to land flat, thereby minimizing the asymmetric loading that can cause restricted physeal growth (15). Since little improvement was noted at 3 months of age, a hemicircumferencial periosteal transection and periosteal stripping was performed at the distal medial right fore third metacarpal bone. Although transphyseal bridging would have been the treatment of choice in a foal of this age, the presence of an adjacent open wound increased the risk for infection of the stainless steel implants that are placed to retard the growth at the physis. The carpal deviation of 40 that remained at 3 months of age is considered to be within the normal limits of 5-70 of total angle of deviation. This degree of deviation may remain until 8-10 months when the limb undergoes another growth spurt (4). Epiphysitis or dysplasia of the growth plates that developed at 5 months of age in this case, often affects all legs in rapidly growing young foals. As in the case reported here, epiphysitis is often seen in conjunction with other orthopedic conditions including ALDs. Quarter horses seem to be particularly susceptible. The exact etiology is unknown, but is thought to be similar to other types of Developmental Orthopedic Diseases (DOD), such as over or imbalanced nutrition, rapid growth rate, genetic predisposition and trauma. The condition of epiphysitis is usually self-limiting, resolving as the growth plates mature, as was seen in this case (16). The severe deviation seen in this case (200) was corrected with a combination of conservative and surgical treatment. This case report illustrates that satisfactory correction can be achieved in such cases, through careful attention to the nature, location, and degree of the deformity. The majority of cases of ALD are less severe, and respond well to treatment and have a good prognosis. References 1. Gaughan, E. M.: Angular limb deformities in horses. Compend. Contin. Educ. Pract. Vet. 20: 944-955, 1998. 2. Auer, J. A., Martens, R. J. and Williams, E. H.: Periosteal transection for correction of angular limb deformities in foals. J. Am. Vet. Med. Assoc. 181: 459-466, 1982. 3. McIlwraith, C. W. and Robertsone, J. T.: Equine surgery, advanced techniques. 2nd edn. Williams & Wilkins, Baltimore, 1998. 4. Brauer, T. S., Booth, T. S. and Riedesel, E.: Physeal growth retardation leads to correction of intracarpal angular deviations as well as physeal valgus deformity. Equine Vet. J. 31: 193196, 1999. 5. Mitten, L. A. and Bertone, A. L.: Angular limb deformities in foals. J. Am. Vet. Med. Assoc. 204: 717-720, 1994. 6. Bramlage, L. R.: The science and art of angular limb deformity correction. Equine Vet. J. 31: 182-183, 1999. 7. Stashak, T. S.: The carpus: angular limb deformities associated with the carpus. In: Stashak, T. S. (Ed.): Adams' lameness in horses. 4th edn. Lea & Febiger, Philadelphia, pp. 624-641, 1987. 8. Hunt, R. J.: Angular limb deviations. In: White, N. A. and Moore, J. N. (Eds.): Current techniqes in equine surgery and lameness. 2nd edn. W. B. Saunders, Philadelphia, pp. 323326, 1998. 9. Adams, R.: Noninfectious orthopedic problems. In: Koterba, A. M., Drummond, W. H. and Kosch, P. C. (Eds.): Equine clinical neonatology. pp. 333-366, 1992. 10. Bertone, A. L., Park, R. D. and Turner, A. S.: Periosteal transection and stripping for treatment of angular limb deformities in foals: radiographic observations. J. Am. Vet. Med. Assoc. 187: 153-156, 1985. 11. Watkins, J. P.: Angular limb deformities. In: Smith, B. P. (Ed.): Large animal internal medicine. 2nd edn. Mosby, St. Louis, pp. 1264-1271, 1996. 12. Sedrish, S. A. and Moore, R. M.: Diagnosis and management of incomplete ossification of the cuboidal bones in foals. Equine Pract. 19: 16-21, 1997. 13. Mitten, L. A., Bramlage, L. R. and Embertson, R. M.: Racing performance after hemicircumferential periosteal transection for angular limb deformities in Thoroughbreds: 199 cases (1987-1989). J. Am. Vet. Med. Assoc. 207: 746-750, 1995. <p class="MsoNormal" style="text-align: justify; text-indent: 0; line-height: 100%; mso-line-height-rule: exactly; mso-pagination: none; mso-layout-grid-align: none; text-autospace: none;