Reading - Diagnostic Knee Scope
advertisement

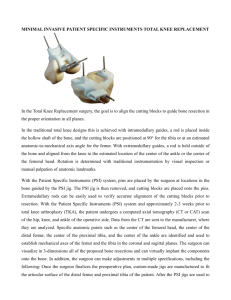
Hello and welcome to my course on a 'method of routine diagnostic arthroscopy'. This is an important subject. Why? Well, during my years as a knee surgeon, I had a great many patients come to see me because they were not improved after previous arthroscopic surgery. I was surprised in many cases to find that their previous surgeon had failed to locate the obvious source of their symptoms, and I realised that this was because the surgeon had simply not performed a thorough and systematic examination during the arthroscopy. For over twenty years now and together with a number of dedicated colleagues, I have been trying to spread the use of a systematic method to the hundreds of young surgeons who attend our skills workshops at The Knee Foundation. This course is aimed at an 'intermediate' level, and may be of interest to both patients, junior doctors and operating theatre staff. This is what we are going to cover during the course: Firstly, I am going to take you through some steps the surgeon needs to take on the day surgery is decided. Then we will skip to the short period before surgery, when the patient still has a chance for last minute interaction with the surgical team. There will be a brief discussion of the anaesthetic choices, and the preparation of the patient before the first portal (cut) is made. I will run over the anatomy with you. I will explain the limitations of some of the instrumentation an arthroscopic surgeon is obliged to use. After this I will explain why it is very important that the surgeon should follow a routine in fully examining the knee. I will use pictures and videos to illustrate this section. Then a round-up of some of the conditions most likely to be missed by failing to use a systematic approach. Note that, except for a brief overview in the final lesson, we are not going to talk about the surgical procedures which a surgeon might perform during an arthroscopy - this is the stuff of more complex courses. The purpose of this current course is to show how important method is in arthroscopy - and how one can miss the diagnosis by using faulty method. Informed Consent Something I want to impress on you is that the surgical routine does not start when the surgeon puts the knife to the patient's skin. It starts when the surgeon and patient agree that surgery will be undertaken. Time taken here to explain the procedure to the patient will save much of the anxiety patients may suffer in the build up to the actual procedure. In my practice, I have a really useful three-dimensional model of the knee, and I take every patient through their procedure using this model. It is made by Adam Rouilly and I have found it over the years to be virtually indestructible. This little model is so useful that I give one to each of my departing knee fellows (trainees) when they head off back to their own countries to set up practices there! The model allows a discussion of various knee cap problems such as tilt and maltracking; it helps to demonstrate the effect of procedures to improve the mechanics of the knee cap; the common sites of arthritis can be identified and relevant procedures for arthritis can be discussed; the cruciate ligaments are easily identified, and the procedures for reconstruction can be explained. And so on. I think that this model is much more useful than pictures, as the two-dimensional nature of an illustration may cause the patient some confusion - whereas the model allows for a much more sophisticated level of dialogue altogether. The term 'informed consent' should not mean that the surgeon has informed the patient what surgery he is going to undertake. It should mean that the patient should be an informed patient. The patient must understand why the arthroscopy is deemed necessary what the procedure entails what options the surgeon has should something be found which was not expected by the investigations prior to surgery what the patient can expect post op what rehabilitation entails what reduction of symptoms is likely as a result of the surgery Procedures just before the anaesthesia The period just before the patient receives the anaesthetic is an important time, and again here a surgeon can miss an important opportunity to reassure the patient that it is he who will be doing the procedure, not another doctor the patient does not know check that relevant x-rays have arrived, together with the patient notes confirm the procedure which has been signed for, and that the symptoms are still the same make sure the SURGEON HIMSELF, under the watchful eye of the awake patient, marks the correct knee with a thick surgical marking pen which won't wash off Picking up that last point, how easy do you think it is to do an arthroscopy on the wrong knee? Yes. Terrifyingly easy. Firstly, because the two knees might both look perfectly normal at the time, as there may be no swelling or external sign of anything wrong with the knee. The patient is asleep when the surgeon is scrubbing. Also the nurse is draping the knee while the surgeon scrubs, and the surgeon generally accepts that the nurse won't made a mistake! But a big black arrow on the bad knee, put there by the surgeon himself before the patient is put to sleep, ensures that such a disaster does not happen. I won't go into detail about the anaesthetic, or discuss whether one should have this or that anaesthetic, but I would just like to tell you about one or two steps which I believe make a great difference to the patient. I had the good fortune to work closely with a team of anaesthetists (anaesthesiologists) who were expert at doing what is known as 'regional blocks'. A regional block is a nerve block with local anaesthetic, which blocks the nerve in its lower distribution, in contrast with a local block, which paralyses the nerve structures just around the injection itself. Some anaesthetists (anaesthesiologists) are good at this and are able to produce complete loss of sensation in the knee. For ordinary arthroscopic procedures we used this for some time, but found that many patients were frustrated that they could not use their quadriceps muscles for sometimes several days afterwards.We now use local anaesthetic in the skin at the sites of the portals before the operation starts and also leave some local anaesthetic in the joint at the end of the procedure. Here you can see the bulge in the skin where the local anaesthetic is being injected. Don't worry about those pen marks. You will understand what they are when you get to a later section of the course. Use of a tourniquet A tourniquet is an inflateable wrap, which goes around the top of the thigh and gets pumped up to stop the blood flowing to the limb. Probably the majority of knee surgeons apply and inflate a tourniquet before commencing the arthroscopy, and in addition the scrub nurse usually first exsanguinates the leg (squeezes the blood out using an elastic bandage). This offers the surgeon an advantage in there being virtually no bleeding during the procedure, but I believe this to be a two-edged sword for the following reasons: little blood vessels (even small pumping arteries) may continue to bleed after the operation, when any swelling is hidden by the bandages and any pain due to the swelling is attributed to the surgery itself there is an increased risk of suffering a clot in the leg after surgery if a tourniquet is used (deep vein thrombosis) For a routine arthroscopy I do not even apply a tourniquet! Instead I make a point of controlling bleeding during the arthroscopy by these methods: I carefully control the inflow and outflow of fluid into the joint using an irrigation pump, which is ideal. I find this important because any excessive outflow of the irrigation fluid will cause a drop in the fluid pressure inside the joint and will result in immediate bleeding. I usually set the irrigation pump pressure at 50 mm Hg (mercury pressure) and increase this up to 70 if necessary. The inflow of fluid into the joint needs to be unimpeded. This means that the diameter of the arthroscope must be large enough to allow a quick flow of fluid if one is going to pass the fluid into the joint via the arthroscope itself. (We'll discuss the arthroscope later.) Most arthroscope suppliers these days provide diagnostic and operative instruments. The operative one allows a sufficiently high flow of fluid into the joint to maintain pressure whilst doing most arthroscopic procedures. The diagnostic one is slimmer, but is not adequate if one is going one to use power instrumentation (like a rotating burr) during any subsequent arthroscopic surgical procedure. The alternative is to use in inflow cannula - a separate wide-bore needle just for fluid inflow. I also use adrenaline (epinephrine) in my irrigation fluid in a concentration of 1 part per two million (1:2 000 000). This constricts the smaller blood vessels (capillaries) and is effective in reducing capillary bleeding. If there is any arterial bleeding during the procedure, I control this with diathermy (cautery), burning the bleeding vessels to seal them. For beginners in this technique of arthroscopy it may be practical to apply a tourniquet but not inflate it. It can then be used if necessary. I started this way and graduated to the position of no tourniquet after a period of three or four years. OK. This is the end of Part 1. In Part 2 I will discuss the basic instrumentation and its limitations. In this lesson I will tell you a bit about the instrumentation an arthroscopic surgeon uses and how the instrumentation imposes limits on what can and cannot be done. As I mentioned before, I have run skills workshops for many years, and during these workshops I insist on making the delegates take their equipment apart and reassemble it again several times over. It is surprising how few, even quite experienced, surgeons are unable to easily do this, relying on the scrub nurse to do it for them. Why do I make the trainee surgeons do this? Well, arthroscopy is a difficult discipline. Think of it. One is shining a tiny beam of light into the knee through a set of optic fibres attached to a series of rod lenses that magnify the image about forty times as well as directing the image at 25 or 30 degrees away from the direction of the scope itself. All of this is contained within a narrow gauge tubular instrument about 5 mm in diameter. This is not like a conventional telescope or pair of binoculars which look straight ahead. It is like looking through a telescope at night with a prism on the end that directs both your vision and a light source 30 degrees to one side. The advantage of this angulation is, of course, the fact that by rotating the scope you can see a much wider field of vision without moving the telescope from side to side. The image is then relayed onto a video screen about two metres away from the surgeon. It is like a video game. By looking at the screen the surgeon may be looking at the anatomy of the knee, diverted 30 degrees to one side. When the surgeon rotates the arthroscope (but not the camera which is attached to the eyepiece of the scope) by 180 degrees, he finds that the field of vision changes from 30 degrees to the left, to 30 degrees to the right. Without moving the scope from one side to the other, the surgeon can access a fairly wide field of vision. The surgeon is on the left, the assistant on the right. In addition to the technical issues we have already discussed, the surgeon has to operate with his hands apart, but with the instrument tips close together. A bit like trying to knit while holding the far ends of the knitting needles instead of the tips! The surgeon's eyes are on the video screen, not the knee. Not easy!! It takes a lot of practice. Note the illumination of the knee visible from the outside - it gives an idea of the brightness of the light beam. Take another look at the surgeon's hands. He is holding an arthroscope in his left hand and an instrument, probably a 'grasper' in his right hand. Let's look at the former in more detail .... The surgeon frequently has to change portals to look at an area from a different angle, and all this may require that the instruments are removed and disassembled several times, and then reassembled and reinserted. Dexterity speeds things up. To make things more complicated, the 'seeing' is done entirely electronically. This means that if the television screen shows the anatomy of the knee correctly orientated, you know that the camera (which is attached to the eyepiece of the scope) is the right way up. This is like an observer standing normally upright and looking at a scene. When the camera is upside down, which is easily done as it is very small and light, the image on the screen is turned upside down, like when you look at a view by standing on your head or bending down and looking between your legs. Finally, like a conventional telescope the arthroscope has manual focusing which is done by a rotating mechanism on the video camera. It goes without saying that if the end of the arthroscope is too close to any structure within the knee it is difficult for the surgeon to recognise what he is looking at. It is like coming too close to an object with a telescope - you cannot recognise an object without being far enough away to see some details of its shape. Two things are important for the surgeon in this respect. Firstly the knee must be fully distended with saline to allow enough space, and secondly he must pull the scope back within the available space to clearly visualise (and photograph) the object. The surgeon, therefore, has to introduce the arthroscope, turn on the irrigation to inflate the knee with saline, look at the screen, recognise the anatomy and orientate the camera correctly. He then may need to focus the image and at last by rotating the arthroscope and pulling it back if necessary he can get a reasonably broad view of the structures within the immediate surrounding of the end of his arthroscope. Arthroscopy Setup The setup for performing a diagnostic arthroscopy consists of: a fibre-optic arthroscope, with an eyepiece and a system for bending and focusing the light beam (inserted into the knee) a light source - with its light beam shining down the arthroscope into the knee a source of 'irrigation' fluid under pressure - again connected to the arthroscope a suction machine to remove the irrigation fluid - again connected to the arthroscope a tiny video camera attached to the eyepiece of the arthroscope a monitor screen to display the video image a recording device for storing images and videos during the procedure a blunt probe, held in the other hand from the arthroscope, for feeling the structures inside the knee The arthroscope The key instrument in an arthroscopy is the arthroscope. The word 'arthro' means 'joint' and the 'scope' means 'looking' - so this is an instrument for looking into the joint. We used to do just this - peering down the eyepiece into the joint - but nowadays the image is relayed via a camera onto a large TV-type screen (monitor). The stem of the arthroscope is a rigid fibreoptic tube or 'sheath' 5mm wide and the length of your forearm, in which can be slid a blunt 'obturator' to close off the tube while it is being inserted into the knee (both to protect the joint and prevent the arthroscope being blocked by anything). At the head end of the arthroscope is located: the eyepiece, which would normally accommodate a small video camera mounting a side inlet for the fibre-optic light source an inlet and outlet for the irrigation fluid, each of which has a little tap for controlling the fluid flow The rigid arthroscope, being a straight rigid cylindrical tube with a narrow bore, has certain limitations: the image relayed to the TV screen is always a circular one only a small part of the joint can be seen at any one time if the surgeons pushes the arthroscope in too close, he may lose his way, and need to pull it a bit further out to get a wider field of vision the arthroscope cannot go around corners - although the light beam is bent usually to 30°, the surgeon frequently needs to 'change portals' to get a view around an object The Blunt Probe The next vital piece of equipment is the blunt probe, which is used for feeling and pulling structure s within the knee joint. The first part of any arthroscopy should involve only the arthroscope and the blunt probe. Too many surgeons fail to fully explore the joint with the probe before dealing with any abnormality found inside. On the left, you can see the probe being used to explore under the meniscus. On my skills workshops we sometimes have a 'desert island' quiz - "If you were stuck on a desert island and could only take three instruments with you to do your arthroscopies, which three would you take?" It's a bit of a daft question, as you would also need an anaesthetist, anaesthetic drugs, electricity etcetera - but it usually results in enthusiastic discussion, and makes the delegates really look at their instruments critically. Needless to say, the blunt probe is always one of the three. The other two are usually a sharp cutting tool and a toothed 'grasper'. But an arthroscope and blunt probe are all that are needed to perform a competent diagnostic arthroscopy. Expanding the knee cavity The space inside the knee joint is larger than one might expect, due to an extension of the joint cavity a handsbreadth above and behind the knee cap (the black space where the arrow is pointing). During arthroscopy, clear fluid is pumped under pressure into the joint cavity to blow it up and make more space for the surgeon to see all the internal structures. The fluid is led into the knee through the inlet valve on the arthroscope itself, and the pressure is supplied either by a pressure pump or by elevating the bag containing this irrigation fluid on a high drip stand. I talked earlier about the possibility of a separate inflow cannula to ensure sufficient fluid pressure, and this is my usual practice. One of the important roles of the surgeon is to ensure that sufficient fluid pressure is maintained via the inlet while at the same time the cloudy fluid is allowed to drain out via the outlet. One of the key reasons for novice surgeons failing to find problems inside the knee is simply that they do not know how to keep the joint clean an the fluid under pressure, allowing them to direct the light source to a clear field of vision. They struggle away in the darkness and can not only miss things, but they can do damage, too. This is one of the main reasons why I include an animal model in our skills workshops, to make the surgery as realistic as possible. This is the end of Part 2. In Part 3 I will show you around the inside of the knee. The inside of the knee joint is dominated by the two femoral condyles, the shiny rounded ends of the femur bone (thighbone). If you imagine that the arthroscope has been inserted into the antero-lateral portal, it will shine initially into the gap between the two condyles. This area is called the 'intercondylar notch'because it intervenes between the two femoral condyles . The notch houses the very important cruciate ligaments. Let's look at this anatomy in a bit more depth. The lower end of the femur, including the rounded femoral condyles, is covered with shiny white gristle, called hyaline cartilage or articular cartilage. The full extent of this cartilage is only evident when the knee is bent, although in the image above the artist has taken a bit of artistic liberty showing it in a straightened knee. During flexion and extension of the knee (bending and straightening) the condyles are rolled over the flattened tibial plateau, at the top of the tibia. Integrity of the hyaline cartilage is critical for the smooth functioning of the knee, and damaged cartilage gives rise to pain and subsequent arthritis. Between the two bones, acting as space fillers and shock absorbers are the flattish wedgeshaped menisci (semilunar cartilages), looking rather like flattened orange segments. Composed of a tough spongy material, they are also critical to smooth joint functioning, cushioning the irregular space between the rounded condyles of the femur and the flattened tibial plateau. I'm going to go into the anatomy in more detail, but before I do I want to mention something about terminology. The menisci, the wedge-shaped shock absorbers of the knee, are shaped like a half-moon. For this reason they used to be called 'semi-lunar' cartilages. But confusion arose because doctors also used this word 'cartilage' to mean the white joint covering (gristle) at the ends of bones. So doctors dropped 'semi-lunar cartilages' and called the shock absorbers 'menisci'. That seems straight-forward, but unfortunately the confusion didn't go away, as patients got used to talking about 'the cartilages' when they were meaning the shock-absorbers. So if I am talking about the shock absorbers, I will call them 'menisci' - OK? Menisci Here is a photo of a real set of menisci taken from a cadaver for use in a meniscal transpant operation. What do you think that fleshy stuff is in the middle between the two menisci? Yes - the cruciate ligaments. They have been cut off to free the graft from the femur. The meniscus on the outer aspect of the knee is the lateral meniscus, and that on the inner side is the medial meniscus. The inner edge is flattened, while the outer edge is thicker. At the front (anterior) and back (posterior) the pointed ends are called the 'horns' of the meniscus. Hence each meniscus has an anterior horn and a posterior horn - and both can be difficult to reach during arthroscopy. You will see that the two menisci are a bit different in shape. The medial meniscus is more 'Cshaped' while the lateral meniscus is more 'O-shaped'. The C-shaped medial meniscus is fixed to the joint capsule all around its edge, and there is very little mobility. The O-shaped lateral one, on the other hand is very mobile. Which one do you think is more prone to tear? Yes, the medial meniscus. Because it cannot move much, a shearing force may tear it as it cannot absorb this strain. Cruciate Ligaments The cruciate ligaments connect tibia to femur in the middle of the joint space. The word 'cruciate' means 'crossed' - and the two ligaments cross over one another. They are very important for the stability of the knee. The mechanism by which the cruciates maintain optimal stability is beyond the scope of this course. For our purposes I just want to point out a few key features when it comes to assessing their integrity: they actually lie outside the joint cavity, and what you can see from the inside is the shiny joint lining covering them this covering may confuse the amateur, as it may give the appearance of the cruciates being intact, when in fact they may be completely ruptured. Or they may have pulled off from their bony attachment. Collateral Ligaments Those of you with collateral ligament injuries may be wondering why I have not shown the collateral ligaments. Actually, the collateral ligaments cannot be seen from within the joint, as they are outside the waterproof capsule of the joint. On the other hand, the undersurface of the patella bone (kneecap) CAN be seen from within the joint, but the position of the arthroscope has to be changed to view this properly. In the big image above if has been peeled to one side to show you what it looks like, but we will be getting back to this later. Patella Now I am going to go back to the bones and talk a bit about the patella - the kneecap. Here is an MRI scan, looking at the knee bones from the side, and where contrast has been reversed so that the bones are dark. You can recognise the rounded ends of the femur and the flattened top of the tibia. The patella (red arrow) is quite peculiar. It is located right in the middle of the tendon of the quadriceps muscle, the muscle which forms most of your 'lap'- the tendon being the bit at the lower end where the muscle attaches to the tibia. From inside the joint only the undersurface of the patella is visible. The tendon above and below lies ouside the joint lining and cannot be seen. The arrow shows you the undersurface of the patella. You can see how it only its undersurface projects into the joint cavity (white). Any idea what that triangular grey mass is which is projecting into the knee joint below the patella? Did you get it? If so, well done. It is the fat pad. Fat Pad The fat pad can be the bane of an arthroscopist's life, as it is bright yellow in colour and can often cover the end of the arthroscope and obscure the view. Some years ago, a knee surgeon would have thought little about cutting away the offending bit, but now it is recognised, not only that it plays an important protective role, but also that scarring can be crippling to the patient. Synovium Well, we have walked around most of the structures in the knee cavity now, but we have not talked much about the cavity itself and the important joint lining, or synovium. The synovium is a glistening membrane which lines the walls of the cavity, and which secretes 'synovial fluid' to luricate the inside of the joint. From the point of view of arthroscopy, it is important to know that the joint cavity extends upwards, a handsbreadth above the patella, into a pocket called the 'suprapatellar pouch' - literally 'the pouch above the patella'. You can see this pocket in these MRI scans (white colour in this view). Surgeons often fail to fully examine this area, particularly with the arthroscope above the patella, and problems can be missed. Actually, on either side of the tibia, too, there are similar depressions called the 'parapatellar gutters' - literally 'the gutters alongside the patella'. Although these are not so deep as the suprapatellar pouch, they are important because gravity may allow lttle bits of material to slip down and hide there, most often 'loose bodies'. Loose bodies are bits of joint cartilage which have broken off into the joint, but which can then be nourished by it and grow quite big. Periodically they cause nasty symptoms by getting caught between the bones, but when the surgeon looks for them they may slip quietly into the parapatellar gutters to the sides and back - and need to be looked for. Similarly, at the back of the knee behind the cruciates loose bodies may lurk in a fold of synovium and be hard to detect. Synovial Plicae A plica is a fold of synovium inside the knee cavity, stretching across the joint. They may exist normally in three anatomical places: above the patella (SPP=suprapatellar plica) along the rounded edge of the femur, to the side of the patella (MPP=medial patellar plica) in the notch of the femur below the patella (IPP=ifrapatellar plica) When plicae are soft and stretchy they cause little trouble in the knee. But little episodes of direct trauma (bangs and bumps) may cause them to become inflamed, to thicken up with scar tissue and interfere with the smooth working of the joint. We'll look at them again later in the course. Well, that is a fairly through overview of the anatomy we might see during a routine diagnostic arthroscopy. I'm going to end the lesson there, I just want to round up by saying that to see all of the anatomy within the joint, a surgeon must be able to easily change portals, putting the scope and camera in from different angles. This is because the femoral condyles dominate the field of view and one has to be able to see below, above and around them. Or things will be missed. I will try to remind you of the anatomy as we go along to save you having to refer back too often to this section. Could you imagine waking up from an arthroscopy with your knee peppered with 'keyholes' because the surgeon couldn't decide where they should go? For a 'diagnostic' arthroscopy, usually three portals (keyholes) suffice to examine the knee fully. For arthroscopic surgery itself, sometimes a fourth may be necessary to deal with some particularly tricky problem. What do I mean when I talk of a 'diagnostic arthroscopy'? Well, in the early days of arthroscopy, when experience was hard to come by and arthroscopic instrumentation was less sophisticated, orthopaedic surgeons frequently used to look around the joint with the arthroscope to see if they could figure out the problem inside the knee. They did not actually perform any procedure. Depending on their findings, they then either opened the knee themself and dealt with the problem (for example, if there was a simple meniscal tear), or they would terminate the surgery and refer the patient to someone more skilled (for example, if there was a torn cruciate ligament). This first 'looking around' became known as a 'diagnostic' arthroscopy. I am, however, using the term in a different sense. I am referring to the first part of an arthroscopic procedure, when the surgeon follows a routine of examination EVEN THOUGH HE SHOULD ALREADY HAVE A GOOD IDEA OF WHAT THE PROBLEM IS AND BE ABLE TO DEAL WITH IT. There may be more than one thing wrong. He may need a good look around to plan his second and subsequent portals. I believe there is very little place for using the arthroscopy as part of a two-stage procedure, and absolutely no place for the beginner to look around if he is not competent to deal with any problem that he may find. The issue is that such an inexperienced surgeon is just the one who will miss locating the problem in the first place. If a surgeon needs experience, the place for it is at the side of a more experienced surgeon. Have you ever had an arthroscopy and then been referred to another surgeon to actually carry out the surgical procedure? This used to be very common. I believe that there is no longer any place for this. An arthroscopy, even if nothing else is done to the knee, is still a surgical 'insult' to the knee and the patient runs the risks inherent in any knee surgery - such as infection, deep vein thrombosis, an anaesthetic complication, reflex sympathetic dystrophy. Why then force the person into a second procedure? If the surgeon is not competent enough to deal with the pathology (that is, the problems inside the knee), then he should not be doing the arthroscopy in the first place. Why is the first portal so important? Well, because it is done 'blind' - until the arthroscope, with its fibre-optic light beam and camera, has been inserted the surgeon can only see the outside of the knee. So if this is badly placed: the sharp scalpel could slice a bit of cartilage off the condyles the menisci or cruciate ligaments could be cut accidentally and last, but not least, if this first portal is poorly placed the whole arthroscopy could become incredibly difficult. I teach my students and knee fellows a simple method of marking the skin prior to the surgery, so that the patella and safe portal positions are easy to locate, even after the knee has been inflated with fluid and the landmarks distorted. Here you can see the knee is draped with sterile drapes, and a sterile marking pen is being used to mark the knee. The drape has a collection system, as you can see, as a lot of irrigation fluid leaks out during the surgery, and without this special drape it can go all over the surgeon's legs and onto the floor!. I will take you through the method of knee marking in detail. Marking the portals Here is how I mark my portals: With a special surgical marking pen, I mark around the edge of the patella. Then I mark the position of the tibial tubercle, the bony bump you can feel several fingersbreadth below the undersurface of the patella. Straight lines are then drawn on both sides from the edge of the tibial tubercle and along the edge of the patellar circle, to end two fingersbreadth above the patella. Horizontal lines are then drawn just below the patellar, and two fingersbreadth above it. At the points where the lines cross, I mark my main portals - two circles below the patella (antero-medial and antero-lateral) (can also be called infero-medial and inferolateral), and two circles above the patella (medial supra-patellar and lateral supraatellar portals). Very occasionally I might choose to use two other portals - one just below the patella in the midline, and one to the side of the patella. Here is a view of me using the rubber knee model which we developed for teaching surgical skills at the Knee Foundation. It is an excellent teaching aid and is waterproof, with superb internal anatomical detail. On the left ois a closeup photo of the notch area taken during arthroscopy. The cruciates are just entering the picture at the bottom. On the model on the right, the circles represent the portals: supero-lateral supero-medial mid-patellar portal of Patel antero-lateral mid patellar-tendon anteromedial If this is a right knee, have a guess and tell me which portal is the arthroscope being introduced into? Answer: It is the antero-lateral (infero-lateral portal). I usually use start with the antero-lateral portal. The lateral side of the knee is the outer side - where you would slap your thighs. Now, getting back to the point I made earlier- that the first portal is made blind. The surgeon needs to appreciate the underlying anatomy so that he does not damage the knee when inserting the scalpel blade for the first portal. Also, these simple systems will help to prevent damage to the internal structures: marking the portals, as we have discussed filling the joint via a needle with at least 300 millilitres of irrigation fluid before starting with the surgery making the incision with the knee straight, in which position the kneecap is up and out of the way angling the scalpel toward the femoral notch (we will learn about this in the anatomy section) feeling the way with a thin hypodermic needle before following this line with the scalpel using one’s index finger as a stop on the scalpel blade to prevent deep penetration remembering to put the blunt trocar (oburator) into the stem of the arthroscope before inserting it It sounds simple, but I cannot tell you how often I have seen on the soft joint cartilage the tell tale scrapes of previous blunders by surgeons with careless method. Identifying the notch So, just a little recap. The portals are marked. Some local anaesthetic with adrenaline has been injected into the skin around the portal. The knee is pre-inflated via a needle attached to a drip containing irrigation fluid. The antero-lateral portal has been chosen and a thin needle inserted to make sure that the scalpel will not hit any of the structures inside the knee. The surgeon takes the scalpel, with his fingers protecting it from going in too deeply, and cuts the first portal in the direction he now knows to be safe. The scalpel is removed. The arthroscope, containing a blunt trocar to protect its sharp edge, is inserted in the same direction into the knee. The blunt trocar is removed and the light source turned up. An image appears on the TV screen. Here again you see the notch between the two condyles, this time with the cruciate ligament labelled for you. You are looking from an angle, remember, and looking towards the medial femoral condyle on the right, while you can see on the left just an edge of the lateral femoral condyle. The image is round. Why? Because it is being relayed to the camera via the round arthroscope. We've got to the end of this fourth lesson, now. I'll just run over a few key points so far: The skin markings help the surgeon relate the underlying anatomy to what he can see on the outside, and especially to the portals The first portal is performed 'blind', and the inside structures can be damaged by faulty technique here. I always start with the anterolateral portal, and the arthroscope, with its end bluntened by the trocar, arrives neatly in the notch between the condyles. The trocar is removed and the image relayed to the screen. From now on the rest of the procedure should be done under direct vision. Poor positioning of the portals will make the surgery a nightmare, and the problem inside may be missed. Visibility is maintained by maintaining correct irrigation fluid pressure, by irrigating the knee should the view become cloudy, and by carefully stopping any bleeding. In Part 5 I will show you how careful placement of the second portals optimises the positioning of the instrumentation and allows the surgeon to continue without any problem. Once the arthroscope is in safely in the knee one is able to continue to work under direct vision. But surgeons often forget that they can use direct vision to determine exactly where to make their subsequent portals. Remember that the arthroscopy started with the arthroscope in the antero-lateral portal, looking into the notch (blue circle) ... From here, it is possible to see the main features of the anatomy inside the knee cavity. Moving the arthroscope over to the medial side (the right on the drawing) the surgeon can see the rounded end of the femur bone - the femoral condyle, which is normally covered with glistening white hyaline cartilage (red circle). Below this is the flat upper surface of the tibia bone - the tibial plateau. Sandwiched between condyle and tibial plateau is the flattened semi-circular (semi-lunar) meniscus, with its free edge on the inner aspect. I'll just move the arthroscope over further to the outer edge of the meniscus. Here you can see that the meniscus is attached along its outer (lateral) edge to the joint capsule, which looks in this picture like a silk curtain over to the right. Remember I mentioned that surgeons often forget that they can use direct vision to determine exactly where to make their subsequent portals? Well, this part of the capsule, now under direct vision, is the area where a needle is passed from the outside to locate the right position for the portal. The needle makes very little damage, so it is OK to try two or three positions before committing oneself. I'll show you what I mean. The light source itself shines from the inside to illuminate the skin, identifying roughly the position where the needle should go. Carefully a thin hypodermic needed can be pushed through from the skin into the joint, and it is easy to adjust its position to ensure that the next portal is made without damage to any of the structures. The scalpel then follows in the same position as the needle, to make the second portal under direct vision. Following this I introduce a small pair of artery forceps or the blunt end of a pair of dissecting scissors. I open these a little to stretch the portal and make it easier to introduce the probe, and the probe is introduced. I'm going to show you a video of this sequence now. Don't be put off by the video showing the instruments being inserted on the opposite side of the knee - it is the priniciple I want to demonstrate. Then needle has already been inserted to located the right position, and then removed, but you will see the scalpel following its track, and finally the probe is inserted. You will then see how the probe is used as a tactile instrument to hunt for damaged or softened areas in both the meniscus and the bony cartilagenous covering. The screen below may appear black - click the little arrow to get it to play. There is no sound recorded. Because the probe has been placed under direct vision, it is exactly in the best position to examine the meniscus and joint surfaces. From here, it is easy to slip the blunt end ender the meniscus, and examine it along its length for any hidden tears, and to feel the consistency of the joint surfaces. Now the surgeon really needs to have good tactile skills, because of something we call 'triangulation'. The left hand - holding the arthroscope scope and camera - locates the area to be examined. The scope may need to be rotated, so that the light beam, which as I mentioned before is bent at the end, sweeps around to give a wide viewpoint. The camera may also need to be rotated so that anatomy is seen on the screen 'the right way up'. A good assistant is a godsend. Once the area to be examined is located, the left hand needs to hold very still, so that the surgeon does not become disoriented. The right hand is at the stage the 'tactile' hand, and the surgeon has to learn to assess the consistency of the tissue below as he examines them with the probe. Carefully, each anatomical part is examined, then arthroscope and probe are moved to a new area, around all the bends and twists of condyle, notch and meniscus. I am going to start this section by explaining what can happen if the first portal is wrongly positioned. If it is placed too close to the patellar tendon, one might lose one's way in the body of the fat pad, which lies just under the tendon. All the surgeon will see is a bright yellow colour, and not the shiny white surfaces you are starting to recognise. Removing the obstructing fat can be traumatic, and the patient can be left with a scarred and painful fat pad, and even the serious complication of 'infrapatellar contracture syndrome'. If the first portal is too low, then it will be below the meniscus and tibial plateau, and it will be difficult to navigate the arthroscope to the other side. Continue to the next bit to see the kind of mess an amateur finds himself in .... Click the arrow under the play to start the video. If you cannot get the player to work don't worry - I will also show some still images to demonstrate the principle. Please note that there is no sound. This is an example of how NOT to do an arthroscopy. The surgeon is lost in this knee - he is desperately hunting around to find a landmark he can recognise. Here are a couple of stills from the video, which just showed a swirling mass of undefinable tissue - This could be the fat pad - who knows? A beginner can spend hours trying to orientate himself when the image looks like this! To make sure my students are confident about the first portal, I turn again to my trusty Adam Rouilly model to show them where they should expect the scope to be positioned once they enter the joint. Compare the amateur's view with this crisp image ... Need I say more? The view should be crystal clear. Failure to see the anatomy clearly may be because the arthroscope scope is in the wrong position, and the tip caught up in fat pad or capsular tissue the joint has not been properly pre-inflated with irrigation fluid the fluid pressure is too low the irrigation fluid is mucky and needs flushing through some tissue is caught at the end of the arthroscope I mentioned before the possibility of using a wide-bore inflow cannula to ensure optimal pressure using a pressure pump. Here is a picture of this cannula. Now I am going to take you through a more expert diagnostic arthroscopy, step by step. If you cannot view the videos, there will be an opportunity each time to see stills. I am going to show first video again. This time you will appreciate how clear the image is. Note: how the surgeon explores both above and below the meniscus how he is feeling the integrity of meniscal and bony surfaces with the tip and the side of the probe how he pulls on the outer edge of the meniscus how he checks the posterior horn of the meniscus. The anterior horn is more difficult to see from the original antero-lateral portal, and he needs to change portals, as I will discuss later Click the video arrow button to start the video... See how after fully examining the meniscus and joint surfaces on the medial side, the surgeon swings the probe over into the notch to explore the cruciate ligaments ... On the right are still images for those of you unable to play the video. I have labelled the important landmarks for you. The rounded white condyles are important in orientating yourself. To the right the tibial plateau is being examined. The hyaline cartilage covering the bone here looks a bit thin and pink coloured. Here the probe has located a damaged area of the tibial plateau. In this next video the probe is in the notch. The surgeon is trying to examine the cruciate ligaments. At first glance looks as if they are fine. But when the surgeon tries to pull on them with the probe, he discovers that what he is seeing is not the cruciates at all - but a filmy infrapatellar plica masquerading as a cruciate! Such plicae are not always present. After 'hoovering' away the plica, the real cruciate is revealed below. Now pulling on it tests its true integrity. From this position, still with the scope in the original portal, the surgeon can slip the probe round the back of the cruciate and test the posterior horn of the lateral meniscus, the body of the meniscus and the joint surfaces as before. I'll show you the stills again here. To the novice, the cruciate seems to be filling the notch, and looks normal. The probe, however, can slip easily into the filmy material - and the experienced surgeon identifies this as an infrapatellar plica covering the real cruciate ligaments. A high speed rotating instrument is used to quickly cut and suck away the filmy plica, with the teeth pointing upwards to avoid harming the underlying cruciates. Now the surgeon can confidently test the integrity of the cruciates, by pulling on them firmly. Now a surgeon, and especially an arthroscopic surgeon, has to train himself to be ambidextrous. If he finds it hard to see a part of anatomy, he needs to remove the instruments and swop their positions around, coming in from the other side, or maybe even a third or fourth portal. This can cause the novice a problem, as it is often hard to locate the portal again, as the tissues are in layers and the gap can appear invisible. I teach the use of what I call a 'switching stick', to allow a quick and easy changeover, without losing the portal. Failure to do this can result in long delays in the operating room, and the surgeon may need to start all over making the portal again! And while I am talking about problems, I just want to mention again the issue of bleeding. It is quite easy to see when you have cut a bleeder. I make sure than any bleeders are cauterised. Keyword (tags): arthroscopy infrapatellar plica As we continue on this arthroscopy voyage together, I just want to touch upon the subject of plicae. We mentioned them in the anatomy section as folds of joint lining left over from the embryonic stage of knee development and I will go into more detail in the next part of the course. For the moment I want to show you three illustrations to keep the topic started. The commonest problematic plica is the medial plica. In the left image it is seen draped like a curtain over the medial condyle, attaching at the bottom to the fat pad, at the top to the wall of the supra-patellar pouch and on the outer aspect to the rest of the joint lining. This last is not appreciated easily from an illustration. In the next two images, you will see how the plicae can get irritated or damaged when the knee is bent, particularly if they have recently taken a bump and become swollen or thickened. I'm not going to go into any further details about plicae, as this is not the purpose of this course. The issue is that many knee surgeons dismiss them as unimportant, because from below it is hard to appreciate the mechanism by which they cause symptoms, simply because the scope is in the wrong position and you should be able to appreciate this from the illustrations. I will show you in Part 8 how I examine them. But getting back now to my system of examination ... Before swinging the arthroscope up and around the condyles, noting any plicae as we go, the 'gutters' to the side of the joint cavity must be examined. These are often forgotten by the novice, but are notorious for hiding 'loose bodies' - bits of joint surface which have detached and which grow bigger in the joint cavity. After examining the lateral gutters, the arthroscope is brought up and around the condyle to view the trochlea and the undersurface of the patella - the region known as the patello-femoral joint. Again, this will be dealt with in the next lesson, when we view this region from a new portal. We are nearly finished this lesson now. I'll just show you a video of this region being examined with the probe. You will notice some abnormal softness of the joint surfaces. The red circle in the left hand image explains where the probe is probing. Just ignore the arthroscope in the picture - I need to edit the image. In the right image the probe has reached underneath the patella, where the cartilage is not normal. The probe is able to make a dimple (this softening is called 'chondromalacia'). You can see the fluid inlet in the distance. This is the end of this lesson now.