Combined nerve palsy
advertisement

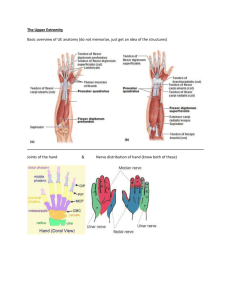
COMBINED NERVE PALSIES Seen most commonly in leprosy and trauma Low Median-Ulnar palsy Most common combined nerve palsy Characterised by 1. complete loss of palmar sensibility 2. intrinsic paralysis (intrinsic negative) hand . Priorities 1. Improve key pinch – restore adduction 2. Restore thumb abduction for opposition – grasp 3. stronger tip pinch –thumb to index 4. improved power flexion of fingers with MP/IPJ flexion coordination 5. restore metacarpal transverse arch and correct little finger abduction 6. restore sensibility for key or tip pinch Treatment very similar to ulnar nerve only lesions except thumb is very weak as it only has FPL, EPL and EPB/APL Before doing any transfer need at least: 1. protective sensation, 2. good passive range. Radial motors and long finger/wrist extrinsics are available. Office workers need only opposition whereas labourers need opposition and strength. Opposition: EIP opponensplasty around the ulnar border to the thumb. If scarring is excessive then pass EIP through the FPL tunnel. Alternatives: ECU with graft, PL Pinch: Fuse the thumb IP joint to overcome the positive Froment’s. EPB or EIP or APL to 1st DI for pinch. Clawing: For clawing one can use ECRL/BR (ie, leaving the centrally acting ECRB) + graft (toe extensor or plantaris) through the lumbrical canal to the lateral band of the extensor mechanism to act as an IPJ extensor. Sensation Sensation may be restored by transferring the superficial radial nerve into the median nerve Summary Low median/ulnar (my approach) 1. improve abduction and opposition a. EIP transfer ulnar border in manual worker b. EIP through interosseous membrane 2. improve finger flexion integration (optional) a. ECRB + 4 tail graft in manual worker b. Zancolli 4 tail FDS MF in older patient High Median/Ulnar Nerve Palsy Biggest problem is total loss of volar sensibility If other hand is normal, best to achieve key pinch and simple grasp Transfers 1. Finger flexion: ECRL FDP 2. Thumb flexion: BR FPL a. disadvantage is that it crosses 2 joints and weakens with elbow flexion 3. Opposition: EIP Thumb a. Consider 1st MCPJ arthrodesis if tip pinch unstable 4. Clawing a. Static procedures – Zancolli capsulodesis High Ulnar/Radial Nerve Palsy Surgery need to be staged as flexors and extensors affected o Stage 1 – wrist and finger extension with thumb abduction o Stage 2 – finger flexion Wrist Extension Pronator Teres to ERCB FDP LF/RF End to side to FDP MF Clawed fingers FDS MF Zancolli Finger extension FDS IF to EDC Thumb extension PL to EPL High Median/Radial Nerve Palsy Intrinsics mostly intact, but sensation only in ulnar distribution. Wrist extension wrist drop is the main problem. Problem is that all wrist motors are lost except FCU, and can only be addressed in 2 ways: 1. radiocarpal fusion 2. Free innervated muscle transfer With wrist fusion, loss of tenodesis effect, thus total range of motion will be limited Finger flexion FDP sutured end to side Finger and thumb extension 1) FCU EDC and EPL (if wrist fusion done) 2) With a free muscle transfer, the tenodesis effect that occurs with extension will allow some degree of finger and Th flexion. Thumb flexion FPB intact FPL is tenodesed across IPJ Thumb Opposition Generally not attempted until wrist is stabilised and there is adequate adduction of thumb 1. Huber transfer 2. de Vecchi operation – transfer adductor pollicis insertion from adductor to abductor tubercle. Triple Nerve Palsy from leprosy Triple nerve palsy occurs in 1% of leprosy patients classical deformities in triple nerve paralysis are flexion of the wrist, extension of the metacarpophalangeal joints of the fingers, clawing of the fingers and a simian thumb. Extension contracture of the metacarpophalangeal joints, flexion contracture of the wrist and interphalangeal joints, and web contracture of the thumb may be seen when the paralysis is of long standing.. results in loss of extension of the wrist, loss of extension of the fingers and thumb, and loss of intrinsic muscle action in the fingers and thumb. The overall functional loss in most cases is almost total ; the hand is scarcely used at all and contractures at all joints are liable to develop early. Surgery In the common combination of high ulnar with high radial and low median palsy in leprosy, the muscles supplied by the median nerve in the forearm are normally available for transfer. These are pronator teres, flexor carpi radialis, flexor digitorum sublimis (superficialis), palmaris longus, flexor pollicis longus, flexor digitorum profundus and pronator quadratus. Of these the first four have been used for various reconstructive procedures. When paralysis was partial, no transfer was considered if the power of the affected muscle was already over Grade 3. Staged: 1. Restoration of active extension of wrist, fingers and thumb a. Wrist extension: PT to ECRB b. Finger extension: FCR to EDC c. Thumb extension: PL to EPL / FCR to EPL 2. Restoration of intrinsics and opponensplasty a. Intrinsics: Zancolli capsulodesis b. Opponensplasty: FDS MF CONCLUSIONS Brand offers the following tips for multiple nerve and severe deficits: 1. Don’t wait too long before embarking on tendon transfers 2. Aim for one good function rather than multiple poor functions. 3. Aim for one good type of prehension: grasp or key pinch. 4. Often it is best to use the strongest muscle as a wrist extensor. 5. It is best to use 2 muscles for one movement: one to move and one to oppose, rather than to rely on the effect of gravity to balance the hand.