swaziland - the United Nations
advertisement

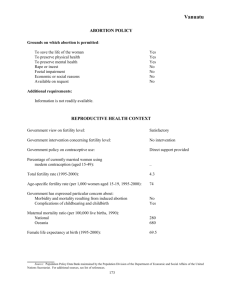
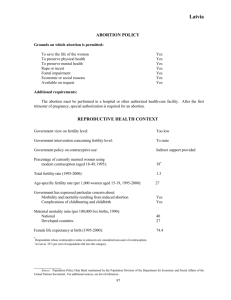
Swaziland ABORTION POLICY Grounds on which abortion is permitted: To save the life of the woman To preserve physical health To preserve mental health Rape or incest Foetal impairment Economic or social reasons Available on request Yes No No No No No No Additional requirements: Although there are no legal provisions specifying by whom or where a legal abortion must be performed or the gestational limits to be observed, practice suggests that legal abortions are performed by registered physicians in government hospitals, private clinics or other approved institutions and may be performed up to 20 weeks of gestation. REPRODUCTIVE HEALTH CONTEXT Government view on fertility level: Too high Government intervention concerning fertility level: To lower Government policy on contraceptive use: Direct support provided Percentage of currently married women using modern contraception (aged 15-49,* 1988): 17 Total fertility rate (1995-2000): 4.7 Age-specific fertility rate (per 1,000 women aged 15-19, 1995-2000): 90 Government has expressed particular concern about: Morbidity and mortality resulting from induced abortion Complications of childbearing and childbirth No Yes Maternal mortality ratio (per 100,000 live births, 1990): National Southern Africa 560 260 Female life expectancy at birth (1995-2000): 62.5 * Including never-married women who have a child. Source: Population Policy Data Bank maintained by the Population Division of the Department of Economic and Social Affairs of the United Nations Secretariat. For additional sources, see list of references. 111 Swaziland BACKGROUND There is no statutory law in Swaziland governing the performance of abortions. Instead, abortion is a matter of common law, which is patterned after Roman-Dutch common law. Under this law, which was also in effect in South Africa prior to the enactment of its Abortion and Sterilization Act (1975), abortion is prohibited except in cases of necessity. There is some disagreement, however, as to what constitutes a case of necessity. The majority position of commentators is that a case of necessity exists only when an abortion is performed to save the life of the pregnant woman. However, it is possible that a case of necessity need not be so serious and that an abortion could be performed in cases of serious threat to both physical and mental health, foetal defect and rape. There is no case law on this issue in Swaziland. Because there is no statutory law on abortion in Swaziland, there are no legal provisions dealing with the professional qualifications required to perform an abortion, the place where the procedure must be performed or the period during pregnancy when an abortion can be performed. Abortions are reportedly usually performed by a registered physician in a government hospital or other approved institution and may be performed within 20 weeks of pregnancy. Swazi physicians generally seek permission from the Ministry of Health prior to performing an abortion. Although this permission is not a legal requirement, it is a precaution that physicians have chosen to take in order to protect themselves and to prove their good faith. In practice, the person performing the abortion must usually be satisfied that the woman’s physical or mental health is endangered by the birth and must act in good faith for therapeutic purposes only. There are no data concerning the number of legally induced abortions, but it is believed that the numbers are small. The high incidence of illegal abortion is a growing concern in Swaziland. Induced abortion is a particularly significant problem among teenage girls. Faced with the prospect of an unwanted pregnancy, many teenage girls resort to abortion to avoid expulsion from school. Unmarried teenage women are more likely to have unwanted pregnancies because of the barriers they face in obtaining contraceptives. For example, it is reported that health workers often require proof of the husband’s authorization before dispersing contraceptives, even though this is not a legal requirement. Swaziland had a total fertility rate of 4.7 children per woman and a population growth rate of 2.9 per cent for 1995-2000. The Government recognizes that the current levels of population growth and fertility are too high and its goal is to reduce the level of fertility in order to improve family well-being and maternal and child health. Contraceptives are provided at all government health-care centres. The national family planning programme, which was launched in 1973, provides family planning services at all its service delivery centres and mobile units. The family planning programme has achieved a certain measure of success. By 1988 more than 80 per cent of women knew at least one effective contraceptive method, and 17 per cent of all women reported use of a modern contraceptive method, up from about 5 per cent in 1985. Following the International Conference on Population and Development, held in Cairo in 1994, Swaziland launched the National Population Council in 1998. Both a national population policy and a comprehensive reproductive health programme were reported under formulation in 2000. Source: Population Policy Data Bank maintained by the Population Division of the Department of Economic and Social Affairs of the United Nations Secretariat. For additional sources, see list of references. 112