“Post Operative Pain Management in the Chronic Pain or Opioid
advertisement

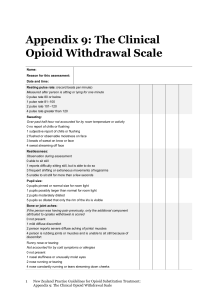
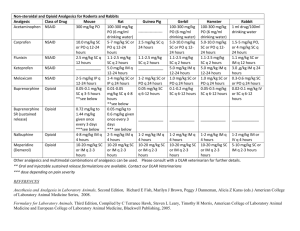
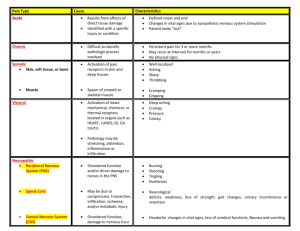
“Post Operative Pain Management in the Chronic Pain or Opioid Dependent Patient” What is Pain? -an unpleasant sensory and emotional experience -associated with actual or potential tissue damage Why is it important to control post operative pain? - Patient satisfaction; humane treatment - Myocardial infarction or ischemia; tachycardia and dysrhythmia - Atelectasis; thromboembolic events; - Wound healing; peripheral vasoconstriction; and metabolic acidosis Why is post operative pain more difficult to manage in opioid dependent patients? - sensitization of the CNS to pain - tolerance, receptor down regulation - fear and anxiety - withdrawal (hypertension, tachycardia, lacrimation, rhinorrhea, papillary dilation, piloerection, sweating, diarrhea, fever, insomnia, nausea, vomiting, aches, yawning, dysphoria) How much opioid should we give? - no magic number but may need to be increased by 30 to 100% in comparison to requirements in opioid naïve patients - because of stigma, many patients underreport home narcotic requirements - preoperative administration of daily maintenance or baseline opioid dose or equivalent dose may be given intraoperatively if missed What are some adjuvant therapies we might try to further control pain? - Centrally acting Alpha-2 Agonists Clonidine (opioid sparing, treats sympathetic response to withdrawal, sedating, hypotension) Dexmedetomidine (easy arousability, analgesia, no respiratory depression, limited or no hypotension) - Muscle Relaxants - mild to moderate sedation, skeletal muscle spasm and cramping Robaxin Tizanidine (alpha 2 agonist) Baclofen (GABA analog, trigeminal neuralgia) - Benzodiazepines - anxiolitic, sedating, muscle relaxant - NMDA Antagonists (receptor involved in modulating chronic pain and opioid mechanisms) Ketamine (dissociative anesthetic, profound analgesia, may help modify opioid tolerance and withdrawal, 0.05mg/kg) Dextrmethorphan (antitussive), Amantadine (antiviral), Memantine (Alzheimer’s) - Membrane stabilizers - neuropathic pain Gabapentin (preop?) Magnesium Sulfate IV - NSAIDs: Ketorolac (caution in pt with impaired renal, GI, platelets) - Tylenol: PR? IV formulation on the horizon - Coriticosteroids: Decadron (can also improve nausea, malaise) - Local, regional, and neuraxial anesthesia