893
advertisement

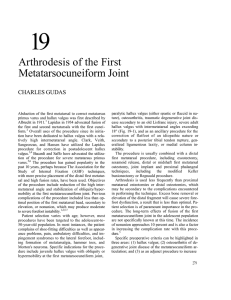
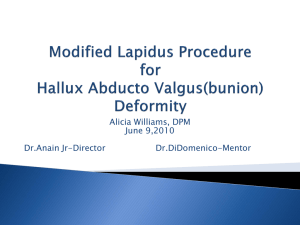
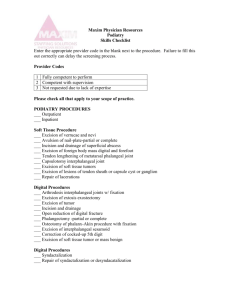
EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 Abd El-Fattah MODERATE TO SEVERE HALLUX VALGUS DEFORMITY: CORRECTION WITH PROXIMAL MEDIAL CLOSED WEDGE METATARSAL OSTEOTOMY AND DISTAL SOFT-TISSUE RELEASE By Ahmed Saleh Abdel-Fattah Department of Orthopedic Surgery and Traumatology Minia Faculty of Medicine ABSTRACT: Purpose: The purpose of this study was to evaluate the management of hallux valgus with a wedge osteotomy of the proximal metatarsal combined with a distal soft tissue procedure. Material and methods: In this study, 15 feet in 12 patients managed by closed wedge osteotomy and distal soft tissue release. Ten patients were female, and two was male. The average age at the time of surgery was 26 years (range, 18 to 39 years). Results: The mean follow-up period was 18 months (ranged 12 to 30 months). The mean intermetatarsal angle was 16° preoperatively, and 5° postoperatively while the mean hallux valgus angle was 39° preoperatively, and 15° postoperatively. Patients noted an average preoperative AOFAS score of 53 points compared with 91 points postoperative. Conclusion: Correction of hallux valgus deformity by proximal medial closed wedge metatarsal osteotomy and distal soft-tissue release may be preferable in terms of ease, low complication rate and patient satisfaction. KEYWORDS: Hallux valgus Proximal osteotomy. In an attempt to reliably control the sagittal position of the first metatarsal, an increasing number of surgeons have employed the proximal chevron and modified Ludloff osteotomies, both of which are performed through a medial approach as opposed to the dorsal approach used for the crescentic osteotomy 4,9,10. INTRODUCTION: Symptomatic hallux valgus associated with a first intermetatarsal angle of 15° is typically corrected with a proximal first metatarsal osteotomy combined with a distal softtissue procedure when nonoperative treatment fails 1, 2. While the crescentic proximal first metatarsal osteotomy has been associated with acceptable clinical outcomes3-6, concern about dorsiflexion malunion (which has been noted in association with as many as 28% of procedures performed with that 3,4,7,8 technique has prompted the development of surgical alternatives. The purpose of this study was to evaluate the management of hallux valgus with a wedge osteotomy of the proximal metatarsal combined with a distal soft tissue procedure. MATERIAL AND METHODS: Between January 2003 and January 2006 fifteen feet of 12 233 EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 Abd El-Fattah patients, with three being bilateral, underwent surgery by proximal medial closed wedge metatarsal osteotomy and distal soft-tissue for the treatment of symptomatic hallux valgus. An American Orthopaedic Foot and Ankle Society (AOFAS) halluxinterphalangeal score that evaluate pain, function and alignment was obtained both preoperatively and at the time of the most recent follow-up visit. The indication for surgery was chronic pain and deformity. Radiographic criteria included a hallux valgus angle of >30°, a first-second intermetatarsal angle of >15°, and lateral subluxation of the sesamoids. 11 Anteroposterior and lateral radiographs were taken preoperatively, post-operatively and at final follow-up with the patient standing. The hallux valgus angle (HVA) and the angle between the first and second metatarsals (IMA) were measured. Ten patients were female, and two was male. The average age at the time of surgery was 26 years (range, 18 to 39 years). In addition tibial sesamoid position, according to the description by Hardy et al 12, was recorded to evaluate if the intraoperative rotation of the great toe into supination was sufficient to correct the preoperative pronation (fig.: 1). The contraindications to the procedure were osteoarthritis of the first metatarsophalangeal joint and severe instability of the first tarsometatarsal joint. Fig. 1:The position of the tibial sesamoid as described by Hardy et al., 12 Supination of the great toe is performed in order to correct the preoperative pronation and is checked by the degree of reduction of the tibial sesamoid into a more anatomical position under the medial part of the 1st metatarsal head (M : medial, L : lateral). 234 EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 Surgical technique: (Fig. 2): A dorsal 3-cm longitudinal incision is made over the first web space. The lateral joint capsule and the metatarsosesamoid ligament are divided immediately superior to the lateral sesamoid. The transverse and oblique tendons of the adductor hallucis are released. The lateral capsule is fenestrated at the first metatarsophalangeal joint, and a varus stress is applied to the hallux to complete the lateral release. The transverse intermetatarsal ligament is not routinely divided. Abd El-Fattah planter based closing wedge osteotomy was made using oscillating saw to correct varus and dorsal angulation (if present). Lateral rotation (supination) of the distal fragment was done to correct pronation, then the distal fragment was fixed by two 1.6 K-wires from first to second metatarsal, and a third wire from the plantar aspect of proximal phalanx to first metatarsal crossing the osteotomy site. Immediately after surgery, a removable posterior slap was used to maintain the surgically corrected position. Once the surgical wound was stabilized, a plaster cast was applied as soon as the swelling subsided, patients were allowed to initiate weight-bearing walk. A longitudinal incision is centered over the medial eminence about 3 cm, through which bunionectomy and double breasting of the medial capsule were done. A third dorsomedial incision, 3 cm in length, over the proximal part of the first metatarsal was done. It is deepened along the medial aspect of the extensor hallucis longus tendon to the bone. The periosteum is reflected 1.5 cm distal to the metatarsocuneiform joint where a medial and Kirschner wires were removed 6 to 8 weeks after surgery following radiographic confirmation of bone union. 235 EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 (A) (B) Abd El-Fattah (C) (D) (E) Figure ( 2) Operative technique: A)Preoperative photography, B) The three incsions, C)The osteotomy site, D) Application of the three K wires, E) Final appearance. Aftercare: Provided that satisfactory fixation of the osteotomy site is achieved intraoperatively, the patient is permitted to walk immediately in a postoperative shoe, bearing weight on the heel only. In the rare instance in which fixation is not optimal, we recommend the use of a short leg walking cast for six weeks. Once there is radiographic evidence of healing at the osteotomy site, transfer of weight to the forefoot in a regular shoe is advanced, typically at six weeks. When osseous callus formation is noted at the osteotomy site on the six-week radiographs, we recommend delaying transfer of weight-bearing onto the forefoot to eight to ten weeks. RESULTS: The mean follow-up period was 18 months (ranged 12 to 30 months). Objective evaluations included the hallux valgus angle, the intermetatarsal angle. The mean intermetatarsal angle was 16° preoperatively, and 5° postoperatively while the mean hallux valgus angle was 39° preoperatively, and 15° postoperatively. Subjective evaluation was made with the use of AOFAS score preoperatively and postoperatively. Patients noted an average preoperative AOFAS score of 53 points compared with 91 points postoperative. 236 EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 Abd El-Fattah Twelve feet had complete pain relief, or only minor complaints. 2 feet had moderate complaints, and 1 foot demonstrated no pain relief. position 4 of Hardy) in all feet. Postoperatively it was located centrally or medially (better than position 3 of Hardy) in 14 feet.12 The overall patient satisfaction was excellent in 8 cases, good in 4 cases, fair in 2 cases and poor in 1 case who had diffuse complaints in the whole foot without a specific site or joint as the cause. Complications and subsequent procedures: Three patients had either paresthesia or hyposthesia near the incsion. Superficial wound infection, which was controlled by oral antibiotics in two patients. Shortening of the first metatarsal with an average of 3 mm was observed in two patients. Preoperatively the tibial sesamoid was located laterally (beyond (A) (B) (C) Fig. 2: Female patient 25 years old. A) Preoperative x-ray shows HVA of 40° and IMA of 25°. B) Immediate postoperative after wedge osteotomy and distal soft tissue release which was fixed by k-wire. C) Follow up x- ray shows healing of osteotomy site, improved HVA to 15°, IMA to 5° and pronation of first metatarsal was corrected as sesamoid changed position from Hardy 6 to 4. 237 EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 Abd El-Fattah respectively. Shortening of the first metatarsal bone (mean 3 mm) occurred in five patients and dorsiflexion deformity of the metatarsal head in one patient. 17 DISCUSSION: More than 130 operations for hallux valgus in adolescents have been reporte. They fall into 4 main categories: proximal metatarsal osteotomies, distal metatarsal osteotomies, soft tissue procedures and combinations of the above procedures. 13 In this study, 15 feet in 12 patients managed by closed wedge osteotomy and distal soft tissue release, the mean intermetatarsal angle was 16° preoperatively, and 5° postoperatively while the mean hallux valgus angle was 39° preoperatively, and 15° postoperatively. Patients noted an average preoperative AOFAS score of 53 points compared with 91 points postoperative. Basal metatarsal osteotomies has the following advantages: Cancellous bone and broad contact surface promote early stability and union. Proximal osteotomies allow a greater correction of the increased intermetatarsal angle than distal osteotomies which are usually used for mild or moderate deformities. 14,15 We did not encounter bone healing problems, probably because the contact area between the two parts of the osteotomised bone is wide. The metatarsal is shortened minimally, because the width of osteotomy cut is compensated for by the straightening of the bone (medial angulation shorten the bone). Slightly tilting the distal fragment planter ward reduces load bearing by the second metatarsal. Narrowing of the forefoot improves the variety of footwear possible and gives an excellent cosmetic result. 16 Fixation of osteotomy site in our cases were done by three K-wires. The first wire pass from the big toe to the medial cuneiform along the axis of the first metatarsal bone that preventing varus or valgus angulation. Supination of the first metatarsal was maintained in place by 2 wires fixing it to the rest of metatarsals, that restores the normal anatomical relationship. The disadvantages of this technique: Three incisions are required and cast immobilization is frequently needed. 16 CONCLUSIONS: Proximal medial closed wedge metatarsal osteotomy allows early stability and union, greater correction of the increased intermetatarsal angle, slightly tilting the distal fragment planter ward reduces load bearing by the second metatarsal. Correction of pronation restores the normal anatomical relationships in the metarsophalangeal region. Mann et al., 1992 on 79 adult patients (109 feet) using basal osteotomy, the average hallux valgus correction was 24° and the average correction of the intermetatarsal angle was 8°. The incidence of under correction was 2% and 12% had a hallux varus deformity. 6 Pehlivan O, 2002 on 25 adult male patients using basal osteotomy, the mean corrections in the hallux valgus angle and the intermetatarsal angle were 22.1° and 10.8°, The results suggest that correction of hallux valgus deformity by proximal medial closed wedge metatarsal osteotomy and distal soft- 238 EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 tissue release may be preferable in terms of ease, low complication rate and patient satisfaction. Abd El-Fattah correction with proximal crescentic osteotomy and distal soft-tissue release. Arch Orthop Trauma Surg.; 120: 397-402, 2000. 9. Sammarco GJ, Brainard BJ, and Sammarco VJ: Bunion correction using proximal Chevron osteotomy. Foot Ankle.; 14: 8-14, 1993. 10. Chiodo CP, Schon LC, and Myerson MS: Clinical results with the Ludloff osteotomy for correction of adult hallux valgus. Foot Ankle Int; 25: 532-6, 2004. 11. Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myerson MS and Sanders : Clinical rating system for the ankle-hindfoot, midfoot, hallux and lesser toes. Foot Ankle Int,; 15(7): 349-53, 1994. 12. Hardy RA and Clapham JCR: Observations on hallux valgus. Based on a controlled series. J Bone Joint Surg; 33-B: 376-391, 1951. 13. Helal B. Surgery for adolescent hallux valgus. Clin Orthop; 157 : 5063, 1981. 14. Robinson AHN and Limbers JP: Modern concepts in the treatment of hallux valgus J Bone Joint Surg; 87B: 1038 – 1045, 2005. 15. Okuda R, Kinoshita M, Morikawa J, Yasuda T and Abe M: Proxima-lmetatarsal osteotomy: relation between 1- to greater than 3years results. Clin Orthop Relat Res; 435: 191-6, 2005. 16. Richardson EG, Donley BG, Vaughn RA and Stephenson KA: Keller resection arthroplasty for treatment of hallux valgus deformity: increased correction with fibular sesamoidectomy. Foot Ankle Int;23: 699-703, 2002. 17. Pehlivan O: Short-term results of proximal oblique Crescentic osteotomy in hallux valgus. Acta Orthop Traumatol Turc; 36 (5): 41722, 2002. REFERENCES: 1. Jahss MH, Troy AI and Kummer F: Roentgenographic and mathematical analysis of first metatarsal osteotomies for metatarsus primus varus: a comparative study. Foot Ankle; 5:280-321, 1985. 2. Kummer FJ: Mathematical analysis of first metatarsal osteotomies. Foot Ankle; 9: 281-9, 1989. 3. Mann RA: Distal soft tissue procedure and proximal metatarsal osteotomy for correction of hallux valgus deformity. Orthopedics; 13: 1013-8, 1990. 4. Easley ME, Kiebzak GM, Davis WH, and Anderson RB: Prospective, randomized comparison of proximal crescentic and proximal chevron osteotomies for correction of hallux valgus deformity. Foot Ankle Int; 17: 307-16, 1996. 5. Markbreiter LA and Thompson FM: Proximal metatarsal osteotomy in hallux valgus correction: a comparison of crescentic and chevron procedures. Foot Ankle Int; 18: 71-6, 1997. 6. Mann RA, Rudicel S and Graves SC: Repair of hallux valgus with a distal soft-tissue procedure and proximal metatarsal osteotomy. A long-term follow-up. J Bone Joint Surg; 74: 124-9, 1992. 7. Brodsky JW, Beischer AD, Robinson AH, Westra S, Negrine JP, and Shabat S: Surgery for hallux valgus with proximal crescentic osteotomy causes variable postoperative pressure patterns. Clin Orthop Relat Res.; 443: 280-6, 2006. 8. Zettl R, Trnka HJ, Easley M, Salzer M, and Ritschl P: Moderate to severe hallux valgus deformity: 239 Abd El-Fattah EL-MINIA MED., BULL., VOL. 18, NO. 1, JAN., 2007 التشوه المتوسط الي الشديد البهام القدم االروح التصليح بعمل قطع عظمي انسي قريب وتحرير االنسجه الرخوه البعيده احمد صالح عبد الفتاح مدرس جراحه العظام واالصابات كليه الطب جامعه المنيا لقد تم عالج 12مريضا بهم 15قدما مصابه بعمل قطع عظمي اسفيني مشطي مغلق انسي قريب وتحرير االنسجه الرخوه البعيده لعالج التشوه المتوسط الي الشديد البهام القدم االروح ويتم استخدام اسالك كيرشنر وبطح الجزء البعيد .وكان متوسط اعمارهم 26سنه وكان متوسط فتره المتابعه 18شهر .التقييم الموضوعي تضمن الزاويه االبهاميه االروحيه والزاويه البين مشطيه وقبل العمليه كانت الزاويه البين مشطيه 16والزاويه االبهاميه االروحيه 39بينما بعد العمليه كانت 5و 15بالترتيب التقييم الشخصي تم باستخدام مقياس الجمعيه االمريكيه للقدم والكاحل قبل وبعد العمليه .وقد حقق المرضي متوسط 53نقطه علي مقياس الجمعيه االمريكيه قبل العمليه بالمقارنه ب 91 نقطه بعد العمليه. الخالصة :بينت النتائج ان تعديل تشوه ابهام القدم االروح بعمل قطع عظمي اسفيني قريب انسي مشطي وتحرير لالنسجه الرخوه قد يتميز بالبساطه و انخفاض معدل المضاعفات ورضا المريض . 240