PPT下载
advertisement

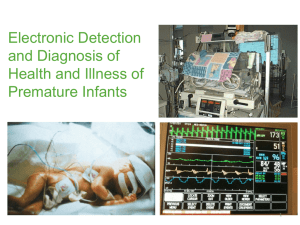
Electronic Detection
and Diagnosis of
Health and Illness of
Premature Infants
Co-Workers
Medical Folks
Quants
Randall Moorman
Pamela Griffin
John Kattwinkel
Alix Paget-Brown
Brooke Vergales
Kelley Zagols
Andy Bowman
Terri Smoot
Statisticians
Doug Lake
George Stukenborg
Chemical Engineers
John Hudson
Matthew Clark
Craig Rusin
Lauren Guin
Physicists
Abigail Flower
Hoshik Lee
John Delos
Supported by NIH.
Overview
Medical Issues:
Apnea of Prematurity
Neonatal Sepsis
What can we Quants
contribute?
Statistical measures
Signal Analysis
Observations:
Electronic Monitoring
of Heart, Respiration
Pattern recognition
methods
Dynamical theories
Outline
Sepsis
medical issue
heart rate monitoring
statistical measures
randomized clinical trial
pattern recognition
physiological modeling
Apnea
medical issue
chest impedance – cardiac artifact
filtering, signal analysis
examples
future work
Conclusion
Sepsis
the presence of bacteria, virus, fungus, or other organism in the blood or other
tissues and the toxins associated with the invasion.
Of 4 million births each year, 56,000 are VLBW (<1.5 Kg). For them the risk of
sepsis is high (25-40%)
Significant mortality and morbidity (doubled risk of death in VLBW infants;
increased length of NICU stay; high cost).
The diagnosis of neonatal sepsis is difficult, with a high rate of false negatives
Physicians administer antibiotics early and often.
Can heart rate monitoring give early warning of sepsis?
(The invading organisms, or the immune response,
may affect the pacemaking system.)
Randall Moorman
Does heart rate give warning of illness?
Plot (Time Between Beats) vs (Beat Number)
ms
ms
beat number
beat number
Does heart rate give warning of illness?
Plot (Time Between Beats) vs (Beat Number)
Reduced variability
pathologic
normal
vs.
Repeated decelerations
pathologic
pathologic
expand
Statistical Measures
of RR Interval Data
NORMAL
Standard Deviation and Sample
Entropy: Variability in the signal.
many small
decelerations
many small
accelerations
Sample Asymmetry: Prevalence of
decelerations over accelerations
implies a skew, or asymmetry, in the
data which we can detect statistically.
Histogram of intervals
ABNORMAL
accelerations decelerationsmany large
decelerations
few or no
accelerations
Histogram of intervals
accelerations decelerations
Find correlation of those measures with illness, and report
correlation in terms of “fold increase of risk of sepsis”:
Take any random moment.
Examine a window of 24 hours (plus 18 hours or minus 6
hours) around that moment.
On average, 1.8% of the infants in our first study had a
sepsis event within that 24 hour window.
If we report a “five-fold increase of risk of sepsis”, it means
that about 10% of the infants showing those heart rate
characteristics had a sepsis event within that 24 hour
window.
Medical Predictive Science Corporation
has developed and is marketing a system for
Heart Rate Characteristics monitoring in the NICU.
A computer beside each NICU bed continuously
collects ECG data, extracts times of R peaks,
tracks RR intervals, and provides the following
Heart Rate Observation (HeRO).
This system is installed in several NICUs in the US,
and a large randomized clinical trial has just been
completed.
HRC rises before illness score
3.0
Clinical score
1.5
1.0
***
*
2.5
**
*
*
*
*
*
0.5
2.0
1.5
0.0
1.0
-4
-2
0
2
Time relative to event (days)
4
HRC index (fold-increase)
HRC index
clinical score
Conclusion 1:
New quantitative analysis of noninvasive,
electronically-measured heart rate characteristics –
standard deviation, asymmetry, and sample entropy –
provides an early noninvasive warning
of sepsis events.
Randomized Clinical Trial
8 Hospitals
UVa, Wake Forest, UAl (birmingham), Vanderbilt, Umiami, Greenville SC, Palmer
(Orlando) Penn State
Control
Save HeRO data
but do not display it
Sample
Display HeRO Score
(but do not tell clinicians
what to do)
2989 VLBW (<1.5 Kg)
152 deaths/1489, 10.2%
1513 ELBW (<1 Kg)
133 deaths/757, 17.6%
Randomized Clinical Trial
8 Hospitals
UVa, Wake Forest, UAl (birmingham), Vanderbilt, Umiami, Greenville SC, Palmer
(Orlando) Penn State
Control
Save HeRO data
but do not display it
Sample
Display HeRO Score
(but do not tell clinicians
what to do)
2989 VLBW
152 deaths/1489, 10.2%
122 deaths/1500, 8.1%
Δ = 2.1% absolute, 22% relative
1513 ELBW
133 deaths/757, 17.6%
100 deaths/756, 13.2%
Δ = 4.4% absolute, 33% relative
Conclusion 2:
New quantitative analysis of noninvasive,
electronically-measured heart rate characteristics –
standard deviation, asymmetry, and sample entropy –
saves lives.
New Question:
Would direct measures of decelerations
provide additional information?
Pattern Recognition
for detecting decelerations
Abigail Flower
The idea is to detect discrete decelerations in a signal containing noise.
Assume we have a deceleration of shape, n .
We can, then, represent our signal, S (n) , as the sum of these discrete
decelerations and “Gaussian white noise” (n)
S (n) a (n n0 ) (n)
=
+
Create a Mother Wavelet
Examine representative decelerations from one baby:
- symmetry
- steeper slope closer to center of waveform.
2
( n n 0)
(n n0) exp
D
3
1 | n n0 | 2
D
Sweep this wavelet through the signal, one width at a time.
*
a
Calculate
for each translation, n0 and width w
a*
S
2
a30 {a30,1 , a30, 2 ,..., a30, N }
*
*
*
*
Scale = 30 beats
a50 {a50,1 , a50, 2 ,..., a50, N }
*
Scale = 50 beats
*
*
*
15
5
10
4
10
10
3
10
5
2
10
0
0
1
2
3
4
5
6
Number of decelerations
7
8
Fold-increase in sepsis within 24 hours
Number of 4096-beat records
Result:
“Storms” of Decelerations are
Highly Predictive of Sepsis
ln (SD) / decels per 30 min
0.4
Statistical
HRC
index
measures
decelerations
3
0.3
2
0.2
0.1
1
0.0
variability
0
-3
-2
-1
0
1
Time (days; 0 = sepsis)
2
3
Conclusion 2
Counting and measuring decelerations
gives a second method for early
warning of sepsis.
Also an important finding was that HR decelerations
are surprisingly similar in infants.
Discovery
We found that, within extended clusters of decelerations, there
were sometimes shorter intervals of time, lasting up to several
hours, in which the decelerations showed remarkable periodicity.
For six infants in our study population we identified deceleration
clusters in which periodicity was maintained for at least ten minutes.
In these periodic bursts of decelerations, the time to the next
deceleration was about 15 sec.
New Question:
What Causes Periodic Decelerations?
Can we develop a model capable of producing
decelerations like those observed in neonatal
HR records? Such models can guide future
observations or experiments on animals.
Partial Answers
A. A mathematical model with minimal physiological
assumptions: a noisy Hopf bifurcation
B. Physiologically-based models
The pacemaker?
The baroreflex loop?
Periodic apneas?
HR jumps from small fluctuations [“steady-state”]
to periodic decelerations [above-threshold oscillations].
Hopf Bifurcations
the most common way that a rest point changes to a cycle
Hard (Subcritical) Hopf bifurcation:
Small excerpt of real data and simulation.
large periodic decels
data
simulation
small periodic fluctuations
Hard Hopf oscillations
noise-induced subthreshold oscillations
Conclusion
Output of a Noisy Hopf Bifurcation Model
Resembles
Observed Periodic Decelerations
Thus we have a mathematical model with minimal
physiological assumptions: a noisy Hopf bifurcation.
Is there a physiologically-based model?
1. Pacemaker cells
Sino-Atrial node cells are the natural pacemaker of the heart.
Can they go into “FM” mode with period ~15 seconds?
2. Baroreflex loop
The feedback loop connecting blood pressure and heart rate
can go into oscillation with period ~14 seconds in infants. Does
this resemble the observations?
3. Periodic apneas
Apneas produce decelerations of the heart. Sometimes they
occur periodically, and the period is commonly ~15 seconds.
Mayer (low freq) arrhythmia
RR
HR
BP
BP
•Oscillation with period ~14 s in infants.
•Feedback loop with time delay.
•Many models connect Mayer waves with a Hopf bifurcation.
•However, measurements indicate that under physiological
conditions in adults, the feedback loop is stable (no
oscillations)
•Two studies (DeBoer et al. and Chapuis et al.) propose that
observed Mayer waves are noise-driven subthreshold
oscillations
Hypothesis: Noisy Precursors are
Familiar Mayer Waves.
There MUST be a nearby threshold.
Decelerations are result of a parameter
going above the bifurcation.
A model of the baroreflex loop
J. Ottesen, Roskilde University, Denmark
Rate of change of
blood volume in arteries
=
Rate in from heart –
Rate out through capillaries to veins
dV / dt
=
heart rate x blood volume per beat
- [P(arteries) - P(veins) ] / [Resistance]
P(arteries)
=
V(arteries) / [compliance = V / P
]
Similar formulas for veins
Rate of change of
heart rate
=
Neg(t)
a negative term caused by high BP
+ Pos(t -τ ) a positive term caused by low BP
which however is delayed
A problem in nonlinear dynamics
Do these differential equations have a bifurcation that causes
heart rate and blood pressure to oscillate?
A problem in nonlinear dynamics
Do these differential equations have a bifurcation that causes
heart rate and blood pressure to oscillate?
YES!!
What is the period ??
A problem in nonlinear dynamics
Do these differential equations have a bifurcation that causes
heart rate and blood pressure to oscillate?
YES!!
What is the period ??
Depending on parameters, can be ~ 15 seconds.
Do they resemble the observed oscillations?
A problem in nonlinear dynamics
Do these differential equations have a bifurcation that causes
heart rate and blood pressure to oscillate?
YES!!
What is the period ??
Depending on parameters, can be ~ 15 seconds.
Do they resemble the observed oscillations?
Nope.
Do measurements of HR and BP in infants show the large
correlated oscillations?
A problem in nonlinear dynamics
Do these differential equations have a bifurcation that causes
heart rate and blood pressure to oscillate?
YES!!
What is the period ??
Depending on parameters, can be ~ 15 seconds.
Do they resemble the observed oscillations?
Nope.
Do measurements of HR and BP in infants show the large
correlated oscillations?
Nope.
The Future: Incoming Data Streams
1.
Electronic diagnosis of infectious disease? Can we identify invading
organisms by HR monitoring?
Preliminary evidence:
Reduced variability
Gram-positive bacteria
vancomycin
(e.g. Streptococci, Staphylococci)
Clusters of decels
Gram-negative bacteria
gentamicin, cefotaxime
(e.g. E. coli, Pseudomonas)
If this preliminary result holds up, we have the first example of continuous,
noninvasive, purely electronic monitoring that gives early warning of infectious
disease and also gives partial diagnosis, thereby identifying the recommended
therapy.
(A medical tricorder)
The Future: Experiments proposed or discussed
2. Quadriplegics are subject to
infections that they do not feel.
Can heart rate monitoring
provide early warning?
3. Can large decelerations be induced in animals?
Models suggest that increasing the time delay in the baroreflex loop pushes
the system above bifurcation.
Can this be done by chemical means (beta blockers)?
Or electrical means (cut the sympathetic nerve
and use an electrical time delay circuit)?
What happens when corresponding experiments are done on newborn or
premature animals?
Conclusions
1. Decelerations are correlated with illness, and can be used as a
new, noninvasive monitor for illness of premature infants.
2. Periodic decelerations resemble the output of a model based
on Hopf bifurcation theory.
3. Study of periodic apneas is the next step.
4. The search for corresponding phenomena in animals has
clinical, developmental, and dynamical significance.
5. When we quants work together with physicians, and
overcome the knowledge barrier and communication barriers
between us, important and unexpected advances in health
care can be made.
Apnea of Prematurity (AOP)
Apnea (cessation of breathing) is very common for premature
infants.
- > half of babies whose birth weight < 1500 g (VLBW)
- Almost all babies whose birth weight < 1000 g (ELBW)
Definition of (clinical) AOP
Cessation of breathing > 20s
OR
Cessation of breathing > 10s + Bradycardia (Heart Rate < 100 bpm) or
and
O2 Desaturation (SpO2 < 80%)
VLBW : Very Low Birth Weight, < 1500g
ELBW : Extremely Low Birth Weight, < 1000g
Three types of apnea are common in premature infants.
1) Obstructive apnea : a blockage of the airway, typically accompanied by
struggling or thrashing movements of the infant.
2) Central apnea : cessation of respiratory drive, and the infant makes no
effort to breathe.
3) Mixed apneas : obstructive
central.
Central apnea is taken to indicate immaturity of control of respiration, and
discharge from UVa NICU is delayed until apneas have been absent for 8 days.
Apnea may be cause or an effect of many other clinical illnesses
including sepsis or abnormal neurologic development. It is a serious
clinical event which needs immediate medical attention.
However, the current generation of apnea monitors is unsatisfactory.
Data Collection
-
Since January 2009, we have collected all waveform and vital sign data
from the bedside electronic monitors in the UVa NICU.
- Waveforms:
ECG, Chest Impedance, Pulse Ox
- Vital signs:
Heart & respiration rates, oxygen saturation of
hemoglobin
- ~ 1 TB / Baby-Year
-
About 1300 admissions for over two years, more than 300 VLBW infants.
Monitor alarms are stored (e.g. brady, desat, and apnea etc..).
Clinical data relevant to respiratory support are entered manually into
an connected clinical database, including presence and type of
ventilatory support such as mechanical ventilation.
Administration of medication (e.g. caffeine)
-
Chest Impedance Measurement
• Easiest way to monitor the respiration of baby
• Impedance between two electrodes placed at
the chest.
• Use two electrodes already in use for the
measurement of the EKG signal, but use a
frequency (52 kHz) far outside the EKG signal.
• Basic impedance (static) :
several hundred ohms: muscles, tissue, blood
+ electrode-skin transitions, and wires.
• Respiration :
~ 2 ohm
• Heart activity :
- Air has poor conductivity
- More air in the lung, higher impedance
~ 0.5 ohm
- Blood is more conductive than air
- Pumping blood out of thorax, less impedance
ECG & Chest Impedance
Heart Rate
200
100
ECG
Chest Impedance
200
Respiration Rate
100
0
ECG & Chest Impedance during Apnea event
Heart Rate
200
100
ECG
Chest Impedance
200
Respiration Rate
100
0
ECG & Chest Impedance during Apnea event
Heart Rate
200
100
ECG
Chest Impedance
200
Respiration Rate
100
0
How do we remove the cardiac artifact
from chest impedance signal?
Filtering, signal analysis, pattern recognition
Hoshik Lee
Goal :
Filter the heart signal from chest
impedance.
Fourier Transform of
chest impedance
Simple Fourier filter fails. Heart beat
band is too broad. Especially, the heart
beat slows during apnea.
Use the Heart as the Clock !
Cardiac artifact in chest
impedance
contract/stretch
1RR
1RR
Heart Clock
RR intervals are evenly
spaced.
Goal :
Filter the heart signal from chest
impedance.
Fourier Transform of
chest impedance
Simple Fourier filter fails. Heart beat
band is too broad. Especially, the heart
beat slows during apnea.
Use the Heart as the Clock !
Cardiac artifact in chest
impedance
contract/stretch
1RR
1RR
Heart Clock
RR intervals are evenly
spaced.
Goal :
Filter the heart signal from chest
impedance.
Fourier Transform of
chest impedance
Simple Fourier filter fails. Heart beat
band is too broad. Especially, the heart
beat slows during apnea.
Use the Heart as the Clock !
Cardiac artifact in chest
impedance
contract/stretch
1RR
1RR
Heart Clock
RR intervals are evenly
spaced.
Fourier Transform of CI
Fourier Transform of CI
Using Heart Clock
Fourier Transform of CI
Fourier Transform of CI
Using Heart Clock
Cardiac
Artifact
Fourier Transform of CI
Fourier Transform of CI
Using Heart Clock
Cardiac
Artifact
Breathing
Fourier Transform of CI
Fourier Transform of CI
Using Heart Clock
Cardiac
Artifact
Slow change : movement or
unknown but not breathing
Breathing
HR
EKG
Chest Impedance
`
Chest impedance
Cardiac Artifact
Removed
Filtered
Chest Impedance
There remain some small fluctuations in filtered CI. Compute the
residual variance of the signal on 2 sec intervals, spaced by ¼ sec,
and get a probability of apnea.
Probability of Apnea
‘Energy’ in fluctuations (variance)
Probability of Apnea
‘Energy’ in fluctuations (variance)
Thresholding function looks like the Fermi distribution function. We obtain
fitting function with two parameters.
P( E )
1
1 exp[ ( E E0 )]
Summary: from Chest impedance to probability of apnea
CI
Remove
cardiac artifact
Remove slow
variations and
renormalize
Compute
2s variance
P(apnea)
Examples
Philips Research North America
07/13/2011
200
100
100
50
100
1
0
0
Philips Research North America
07/13/2011
Very Long Apnea Undetected by monitor
We detected 782 apneas > 60 s in two years data
Periodic Breathing = Periodic Apneas
200
100
100
50
100
1
0
0
Philips Research North America
07/13/2011
Current Studies
What fraction of apneas are recorded by nurses?
How does the apnea rate change with age?
Does caffeine reduce apnea?
Do transfusions reduce apnea?
Can we get early warning of serious apneas?
What is the significance of long apneas?
Are short but periodic apneas benign?
(~1/3)
^
(?)
(Yes)
(Maybe)
Future Work
•Convert to real-time monitor
- The system is set up for retrospective work : collecting statistics of
apnea events and correlation with other clinical events.
•Combined with (wearable) Automatic Stimulation system.
- e.g. vibrate shirt, mattress and so on.
•Improve sepsis detection? (HeRO monitoring)
Add-on system which provides a new way to analyze data
that had previously been discarded
Conclusions
1. Decelerations are correlated with illness, and can be used as a
new, noninvasive monitor for illness of premature infants.
2. Periodic decelerations resemble the output of a model based
on Hopf bifurcation theory.
3. Study of periodic apneas is the next step.
4. The search for corresponding phenomena in animals has
clinical, developmental, and dynamical significance.
5. When we quants work together with physicians, and
overcome the knowledge barrier and communication barriers
between us, important and unexpected advances in health
care can be made.
ASSUME:
the heart rate is governed by some set of
feedback loops that can be modeled by some
big set of differential equations
dx/dt = F(x;p)
x = (x1,x2,…)
(dynamical variables)
p = (p1,p2,…)
(parameters)
Example:
x1 = heart rate, x2 = blood pressure, x3 = …
2.
The equations have a “rest point” at which
all variables are constant (including HR)
F(xrest(p);p) = 0.
Move origin of coordinates so rest point = 0.
3.
F(x;p) can be expanded in a Taylor series
in x’s.
F(x;p) = Mx + xNx +….
Analyze first at linear level.
Almost all matrices can be transformed to diagonal form
y Cx
CMC1
dy / dt y yCNC1y ...
At linear level
dy1 / dt 1y1
dy 2 / dt 2 y 2
Equations are real, so eigenvalues are real
or come in complex conjugate pairs
4.
All except two eigenvalues have negative
real parts. Two eigenvalues are complex,
and have real part near zero.
i
* i
is near zero, and as parameters p
change, it can pass through zero.
THEN:
[Center Manifold Theorem]
In the many-dimensional y-space, there is a
smooth two-dimensional surface called the
center manifold, in which all the interesting
behavior occurs:
a. If the system starts on that surface, it
stays on that surface
b. If it starts elsewhere, it decays to that
surface
c. The equations in that surface have a
Taylor expansion
AND FURTHERMORE:
[Normal Form Theorem]
There exists a smooth change of coordinates
such that the diff eqs can be put into a “Normal
Form”; using polar coords in the center
manifold, that form is:
dr / dt r ar br ...
3
d / dt ...
and this is easy to analyze !!!!
5
YOU can easily show:
As increases through zero,
The stable rest point goes unstable, and
EITHER
A stable cycle appears
OR
An unstable cycle disappears
That is a Hopf bifurcation.
Summary: In the many-dimensional space, there is a
smooth two-dimensional attractor in which all the
interesting behavior occurs, and there exists a smooth
change of coordinates such that the diff eqs can be put
into a “Normal Form”:
dr / dt r ar 3 br 5 ...
d / dt ...
As increases through zero, the stable rest point goes
unstable, and either a stable cycle appears,
or an unstable cycle disappears
That is a Hopf bifurcation.
In the new variables the motion is a sinusoidal
t ),v(t) r sin( t )
oscillation, u(t) r cos(
We can connect to time between beats RR(t)
t ) ).
by assuming RR = RR(u(t)) = RR(r cos(
But we know the shape of the decelerations, and
we can represent that shape by a Fourier cosine
series.
Then the sinusoidal oscillation is converted into a
sequence of decelerations.
Small time delay
Heart rate
Arterial BP
Venous BP
These oscillations are “noisy precursors” :
With no noise the system goes to steady state
Subthreshold oscillations arise because of noise and a nearby bifurcation
Peter Andriessen
Figure 5. This figure shows a 60-s trace of R-R interval and systolic blood pressure values of the
3-min segment, as presented in Figure 1. It shows the temporal relationship between systolic
blood pressure (SBP) and R-R interval fluctuations. SBP (left y axis) and R-R interval (right y
axis) values are shown as a function of time. High frequent fluctuations with small amplitude
variation, related to respiratory activity, can be observed. In addition, approximately six low
frequent fluctuations with a variation of 3 mmHg per cycle in this 60-s trace can be observed,
corresponding to an oscillation frequency of approximately 0.1 Hz. Each rise in SBP (indicated by
the first arrow) is followed by an increase in R-R interval (indicated by the second arrow), with a
time delay varying from 1.5 to 4 s (periods between arrows). The averaged time delay from this
60-s trace (2.7 s) is close to the calculated transfer phase.
High freq fluctuations: RR ~ opposite to BP
Low freq fluctuations: BP leads RR
respiratory arrythmia
Mayer waves
Above the bifurcation (longer time delay)
the system oscillates even with no noise.
Above bif, the oscillations are large. The shape is (maybe) a passable
imitation of periodic decels seen in infants. Period 10 s for adults.
RR
time
Comparison of model (based on adult data) with observations:
There is a bifurcation which produces large regular oscillations in HR.
Increase in delay time of sympathetic action gives the bif.
Shape of decels – could be better.
Liapunov exponent is too small. (Slow approach to steady oscillations.)
It’s a soft Hopf bif instead of a hard Hopf bif.
(I think by playing with parameters we might convert it to hard Hopf.)
Continuing research:
1. More fun with baroreflex models
2. Begin study of respiration models