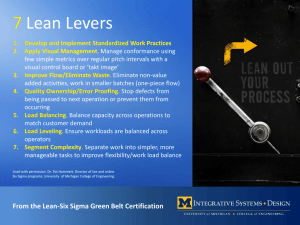
QC using patients data
advertisement

بسم هللا الرحمن الرحيم Professor of Clinical Pathology (Clinical Chemistry) Faculty of Medicine, Mansoura University The Laboratory test begins with a physician deciding which test to order and ends with that physician evaluating the test result. A process of brain to brain transmission of medical in formation. Problems arise primarily from imperfect processes, not from imperfect people. The quality problems are primarily management problems because only management has the power to change work process. The total system for a health care organization involves the interaction of all of the following processes as well as many others: Physicians might view a health care organization as a provider of processes for: A. Patient examination. B. Patient testing. C. Patient diagnosis. D. patient treatment. Health care administrators might view the activities in terms of processes for : A. Admitting B. Patient services C. Discharging patients D. Billing for costs of service Laboratory directors might understand their responsibilities in terms of processes for: A. Acquisition of specimens B. Processing of specimens C. Analysis of samples D. Reporting of test results Laboratory analysts might view their work as processes for: A. Acquiring samples B. Analyzing samples C. Performing quality control D. Releasing patient test results Report Written order Specimen Measurement Specimen preparation Patient preparation Quality Assurance (Q.A) The five Q framework Defines how quality can be managed using the scientific method or the PDCA cycle Plan do check Act: • Quality planning • QLP Includes analytical process and the general policies, practices and procedures that define how all aspects of the work get done. • Q.C. • Statistical. • Non statistical: e.g.: Linearity checks , reagent and standard checks and procedure. • Q.A. quality assessment concerned with: Measures and monitors performance as: of laboratory Turaround Specimen identification Patient identification Test utility • Q.I. quality improvement: Provides a structural problem-solving process With better analytical quality a lab can eliminate repeat run requests for test (this work is waste). If quality are improved waste will be reduced which reduce cost and provide a competitive advantage. If quality means conformance to requirements, then quality costs must be cost of conformance and cost of non-conformance. To customer requirement PREVENTION (To prevent problem) For appraising performance For poor analytical performance For analytical quality Essential Elements for Q.A. I. II. III. IV. V. Commitment. Facilities and Resources. Technical Competence. Technical Procedures. Problem solving Mechanism. • Input from QC technologist or supervisors to initiate the mechanism. • In service training program. • Specialized trouble shooting skills. • Quality team responsible for problem solving (small groups). Essential elements for Q.A. Essential elements for Q.A. Essential elements for Q.A. Essential elements for Q.A. Technical procedures Technical procedures Methodology Technical procedures Standardization and calibration: Reference calibrator material (RCM) (primary calibrator): by definitive method (absolute physical quantity such as mass) e.g. isotope dilution mass spectroscopy. Test calibrator material (TCM) (secondary calibrator): by reference method and high quality staff. Structure of an accuracy-based measurement system showing relationships among reference methods and materials . Technical procedures Documentation of analytical protocols and procedures. Monitoring of critical equipment and materials. Technical procedures The Monitoring of analytical quality by the use of: Q.C. SD, bias and 6 sigma • Levey – Jennings chart • Westgard multirules • Cum Sum P.T. Q.C. Levey Jennings control chart: Analyze control 20 different days mean ± SD. Construct Control chart. Control limits set as the mean ± 3s. Concentration is plotted on the y-axis versus time (run number) on the x- axis. Introduce the control into each run & record the value. Control limit: ± 2 SD observation when (n) the is number one rejection problem (Pfr). ± 3 SD when n = 2 or more detection (Ped is low). of false error Concentrations Q.C. Levey Jennings chart M+3SD M+2SD M+1SD Mean M M-1SD M-2SD M-3SD 1 2 3 4 5 6 7 8 9 10 Q.C. Westgard Multirules Chart If the control is within mean ± 2SD in control: I2s one excced mean ± 2SD ( warning that initiate testing of other control rules). I3s one excced mean ± 3SD ( Random error ) 22s 2 consecutive control excced mean ± 2SD (systemic error) R4s 2 consecutive excced mean plus and minus 2SD) ( Random error) 41s 4 consecutive excced mean ± 1SD ( syst. errors ) 10x` consecutive deviation Less than 1SD on (system errors) one side Concentrations Q.C Westgard chart 13s (random) M+3SD 22s systemic 12s (warning ) 4s (Random) M+2SD 41s systemic M+1SD Mean M M-1SD M-2SD M-3SD 1 2 3 4 5 6 7 8 9 10 A word from Dr. Westgard Westgard Multirule Chart Pfr is kept low Ped is improved Q.C Westgard chart Introduce two control specimens into each analytical run : When both fall with 2s limits accept the analytical run and report the patient results. When one exceeds 2s limit hold the patients results and inspect the control data using l3s, R45, 22s and 10xWhen one of these rules is out of control, reject the analytical run & don’t report the analytical results . When all of these rules indicate that the run is in control , accept the analytical run and report the patient results Q.C Westgard chart R4s is applied only within a run –between Run interpritted as RE Rule may be applied "across" materials one observations can be on the low, concentration and the other on the high concentration as long as they are within the same run . Rules 22s, 41s and 10x rules can be applied across runs and materials. This effectively increases n and improve the Ped of the procedure Q.C. Systemic error: caused by variations in: Instruments Technique Reagents or other material Random error: Appear despite, Analytical method Tightly Controlled, Sample piptting Dissolving reagent Mixing sample and reagents Baths temp instability. Q.C. The overall objective of these rules is to obtain a high probability of error detection and a low frequency of false rejection of runs: If the rules are violated it must: QC performance characteristics Different QC procedures have different sensitivities or capabilities for detecting analytical errors. The best is that with lowest Pfr and highest Ped. QC Cumulative sum CUSUM chart Calculate difference between mean & the result (e.g. mean 100 , result 110 the diff = 10) -add this difference to the following each day. Interpret the chart data . Steep slope of the Cusum Line, suggest systemic errors and the run is out of control. QC CUSUM QC CUSUM The Same as before but the difference is calculated between the estimated control value and k1 or ku (mean ±SD): The cusum calculation do not start until a control value exceeds a certain threshold above (Ku) or below (K1) of the expected mean (X). QC CUSUM This difference summated for 2 weeks If the summation exceed the control Limit the method out of control changed to If the sign changed (+ - or the reverse the calculation stopped the method is in – control Calculations and Tabular Record for Decision Limit Cusum For Control Material. With X=100, S=5.0, kU = 105 , K1 =95,hu=13.5,h1=13,5). QC CUSUM Q.C using patients data (Its efficiency is relatively low) Clinical correlation: • Correlate clinical diagnosis with laboratory test results e.g. impossible test result such as normal serum bilirubin in a highly jaundiced patients. Correlation with other laboratory tests e.g. T4 and TSH, urea and creatinine. Q.C using patients data Inter laboratory duplicate: • Divide sample into 2 aliquots and do analysis. This is a simple Q.C. procedure used in absence of stable control material. Q.C using patients data Delta checks with previous test: • To detect certain errors identification or labelling. e.g. • Compare laboratory test results with value obtained on previous specimens from the same patients. Delta check limit based on 3-day interval in term % of change from the initial value e.g. Na+ 5%, CK 99%. Q.C using patients data Limit checks: • Patients test results should be reviewed to check that they are within the physiological ranges compatible with life. Low warning S. Albumin (g/dl) 1.5 S. Uric acid (mg/dl) 1.0 S. Sodium (mmol/L) 120.0 High warning 6.0 12.0 150 External Q.C. Analyze the same Lot of control material: N. ± 1-1.5. > 2 Indicate that the Lab is not in agreement with the test of other Laboratories in the program. Must correct any test method instrum. trouble shooting. External Q.C. SDI for the same instruments and techniques: = External Q.C. Comparison of Lab. Mean and group mean by t-test. If significant (<0.05), the Lab. Result is biased. Role of proficiency testing (PT) in Accreditation According to Clinical Laboratory Improvement Amendments (CLIA88) Study 5 samples 3 times per year so as to improve the capability of detecting "unacceptable“ performance. The lab. must produce correct results on 4 out of 5 specimens for each of the analytes in that category and have an overall score of at least 80% for 3 consecutive challenges. The criteria of PT failure is: Two of five incorrect results on two of three consecutive PT surveys If there are 2 incorrect results for any analyte , The Lab. is considered "on probation " Lab . Suspended Lab: If the lab .has 2 or more incorrect results for any analyte or has any score less than 80% on two of three consecutive surveys. Suspended Lab. must cease all analytes in that specialty category until it is reinstated . Target value (% or absolute value): The mean of all responses after removal of outliers (more than 3SD). Or the mean established by definitive or reference method (acceptable by the national committee of standard NCS). Comparative method may be used in absence of the former methods. Post Analytical Goals and Clinical Interpretation of Lab. Procedures The following questions must be asked for test results: Screening : Is an apparent disease present ? Pathoghysiology : What is the disease process ? Confirmation : How can Confidence in the tentative diagnosis be increased ? Prognosis : How Severe is the disease process ? Monitoring : Has a change occurred since the Last observation ? Is it significantly different from previous result ? The probability that the difference between two result is analytically significant (p< 0.05) is 2.8 times the analytical SD (SDA of repeated measurements of a single quality normal control serum). To decide whether an analytical change is clinically significant, it is necessary to consider the extent of natural biological variation (means of SDB for repeated measure ments made at weekly intervals in healthy subjects over 10 weeks). The effects of analytical and biological variation can be assessed by calculating the overall standard deviation of the test by: If the difference between two test results exceeds 2.8 times the SD of the test, it can be considered of potential clinical significant: Is it consistent with clinical findings ? LAB. TESTING PROCESSES AND THEIR POTENTIAL ERRORS LAB. TESTING PROCESSES AND THEIR POTENTIAL ERRORS Process Potential Errors •Inappropriate test Test ordering •Handwriting not legible •Wrong patient identification •Special requirements not specified •Cost or delayed order LAB. TESTING PROCESSES AND THEIR POTENTIAL ERRORS Process Potential Errors •Incorrect tube or container •Incorrect patient identification •Inadequate volume Specimen •Invalid specimen acquisition (e.g. hemolyzed or too dilute) •Collected at wrong time •Improper transport conditions LAB. TESTING PROCESSES AND THEIR POTENTIAL ERRORS Process Potential Errors •Instrument not •calibarted correctly Analytical •Specimen mix –up measurement •Incorrect volume of specimen •Interfering substance present •Instrument precision problem LAB. TESTING PROCESSES AND THEIR POTENTIAL ERRORS Process Potential Errors •Wrong patient identification •Report not posted in chart Test reporting •Report not legible •Report delayed •Transcription error LAB. TESTING PROCESSES AND THEIR POTENTIAL ERRORS Process Test interpretation Potential Errors •Interfering substances not recognized •Specificity of test not understood •Precision limitations not recognized •Analytical sensitivity not appropriate •Previous values not available for comparison Six Sigma Six Sigma Today’s competitive environment leaves no room for error This is why six sigma quality must be a a part of our culture. What is six sigma It is a process that helps us focus on developing and delivering near perfect products and services. Why sigma Six Sigma The word is a statistical term that measures how far a given process deviates from perfection. The central idea behind six sigma is that you can measure how many” Defects” you have in a process, you can systematically figure out how to eliminate them and get as close to “zero defects” as Possible. Six Sigma The principles of Six Sigma go back to Motorola’s approach to TQM in the early 1990s and the performance goal that “6 sigmas or 6 standard deviations of process variation should fit within the tolerance limits of the process”; hence, the name Six Sigma. Six Sigma Six Sigma Methods of sigmametric measurement Six Sigma Sigma = (Tea – bias)/cv Tea = tolerable error or allowable total error (determined by CLIA) Bias = inaccuracy Six Sigma A shift or bias of 1.5 sigma would hardly cause any defects in a six sigma process. The actual rates that are expected are as follows: • 3.4 DPM for a six-sigma process; • 233 DPM for a five-sigma process; • 6210 DPM for a four-sigma process; • 66,807 DPM for three-sigma; and • 308,537 DPM for a two-sigma process Six Sigma Six Sigma Six Sigma Six Sigma Six Sigma Methods with 6 sigma performance are considered “World class”. Methods with sigma performance less than 3 are not acceptable for production. Six Sigma Chemistry Test or Analyte CLIA Acceptable Performance Five-Sigma Precision Six-Sigma Precision Blood gas pCO2 5 mm Hg or 8% (greater) 1 mm Hg or 1.6% 0.8 mm Hg or 1.3% Blood gas pH 0.04 pH units 0.008 pH units 0.00067 pH units Calcium, total 1.0 mg/dL 0.2 mg/dL 0.17 mg/dL Chloride 5% 1.0% 0.83% Cholesterol, total 10% 2.0% 1.7% Cholesterol, HDL 30% 6.0% 5.0% Creatine kinase 30% 6.0% 5.0% Creatinine 0.3 mg/dl or 15% (greater) 0.06 mg/dL or 3.0% 0.05 mg/dL or 2.5% Six Sigma Chemistry Test or Analyte CLIA Acceptable Performance Five-Sigma Precision Six-Sigma Precision ALT 20% 4.0% 3.3% Albumin 10% 2.0% 1.7% Alkaline Phosphatase 30% 6.0% 5.0% Amylase 30% 6.0% 5.0% Bilirubin, total 0.4 mg/dL or 20% (greater) 0.08 mg/dL or 4% 0.067 mg/dL or 3.3% Six Sigma Glucose 6 mg/dL or 10% (greater) 1.2 mg/dL or 2.0% 1.0 mg/dL or 1.7% Iron, total 20% 4.0% 3.3% LDH 20% 4.0% 3.3% Magnesium 25% 5.0% 4.2% Potassium 0.5 mmol/L 0.1 mmol/L 0.08 mmol/L Sodium 4 mmol/L 0.8 mmol/L 0.67 mmol/L Total protein 10% 2.0% 1.7% Urea Nitrogen 2 mg/dL or 9% (greater) 0.4 mg/dL or 1.8% 0.33 mg/dL or 1.5% Uric acid 17% 3.4% 2.8% Toxicology Test or Analyte Alcohol, blood 25% 5.0% 4.2% Blood lead 10% or 4 mcg/dL (greater) 2.0% or 0.8 mcg/dL 1.7% or 0.67 mcg/dL Carbamazepine 25% 5.0% 4.2% Digoxin 20% or 0.2 ng/mL (greater) 4.0% or 0.04 ng/mL 3.3% or 0.033 ng/mL Ethosuximide 20% 4.0% 3.3% Gentamicin 20% 4.0% 3.3% Lithium 0.3 mmol/L or 20% (greater) 0.06 mmol/L or 4.0% 0.05 mmol/L or 3.3% Phenobarbital 20% 4.0% 3.3% Phenytoin 25% 5.0% 4.2% Primidone 25% 5.0% 4.2% Procainamide 25% 5.0% 4.2% Quinidine 25% 5.0% 4.2% Theophylline 25% 5.0% 4.2% Tobramycin 25% 5.0% 4.2% Valproic acid 25% 5.0% 4.2% Six Sigma Hematology Test or Analyte Erythrocyte count 6% 1.2% 1.0% Hematocrit 6% 1.2% 1.0% Hemoglobin 7% 1.4% 1.2% Leukocyte count 15% 3.0% 2.5% Platelet count 25% 5.0% 4.2% Fibrinogen 25% 5.0% 4.2% Partial thromboplastin time 15% 3.0% 2.5% Prothrombin time 15% 3.0% 2.5%