Emerging patterns of drug resistance and
viral tropism in cART-naïve and failing
patients infected with HIV-1 subtype C
Thumbi Ndung’u, BVM, PhD
Associate Professor
Director, HIV Pathogenesis Programme
Doris Duke Medical Research Institute
Nelson R. Mandela School of Medicine
University of KwaZulu-Natal
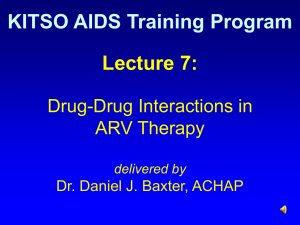
100
HIV-1
Phylogeny
H
100
47.2%
C
100
F1
100
100
F2
100
K
100
D
100
100
M-group
B
100
100
100
100
100
100
100
12.3%
J
G
A1
27.0%
A2
N-group
CPZ US
CPZ GAB
100
O-group
CPZ ANT
5%
Phenotypic Classification of HIV-1
• Slow/low versus rapid/high
• Syntitium-inducing (SI) versus NSI
• Slow/Low = NSI (Early, slow progression)
• Rapid/High = SI (Late, rapid progression)
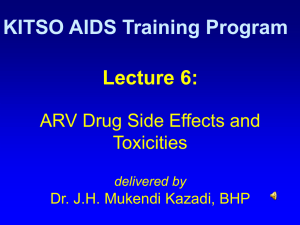
HIV-1 coreceptor usage and viral tropism
Virus Variants
M-tropic
T-tropic
Dual tropic
CCR5
Macrophage
CD4
CXCR4
Primary
T cell
CCR5
CD4
Target Cell Types
CXCR4
T-cell line
CD4
>25 years of HIV/AIDS
> 33
For every 2 people
put on treatment, 5
others are infected
Selection of Resistant strains
Treatment begins
Drug-susceptible quasispecies
Viral load
Drug-resistant quasispecies
Selection of resistant
quasispecies
Incomplete suppression
•Inadequate potency
•Inadequate drug levels
•Inadequate adherence
•Pre-existing resistance
Time
Study rationale
Background:
• Relatively limited information on coreceptor usage by
HIV-1 subtype C isolates, particularly in children.
However, most studies suggest very rare CXCR4 usage
• Some reports suggest increasing X4 usage (in adults) eg.
Johnston et. al. (n=28), 50% using X4 among ART
experienced viremic patients
• Previously used methods may be biased because they
involved first generating viral isolates by co-culture
Study rationale
•
ART may boost T-cell immune responses which have
been shown to preferentially suppress X4 viruses. Thus
partially effective therapy may select against X4 viruses
(Deeks et al, JID 2004; Harouse et al, PNAS 2003)
• ART reduces CCR5 expression on T cells (due to reduction
in T cell activation) potentially selecting for X4 viruses
(Brumme et al, JID 2005; Anderson et al, AIDS 1998)
• Suboptimal drug metabolism (such as AZT) in the cellular
reservoirs for X4 viruses has been suggested and could
lead to selection for X4 viruses (Boucher et al, AIDS 1992)
Aims
Specific Aims:
1) To determine the prevalence of major drug
mutations in ART-naïve and failing children and
adults
2) Determine overall prevalence of X4 tropism among
children and adults initiating and failing HAART
3) Compare prevalence of X4-utilizing viruses between
ART-naïve and ART-experienced subjects with
detectable viremia
4) Explore factors associated with viral tropism in HIV1C infection
HIV-1 Genotyping Assay
plasma
centrifugation
Blood cells
RNA
RT-PCR
cDNA
PCR
DNA
PCR
Dye terminators
A
T
T
C
G
A
T
T
C
T
G
C
C
G
Software analysis
ATAGACCAG : consensus sequence
I
Q
Q
I
Q
*L
ATCGACCTG : patient sequence
Trofile assay summary- for coreceptor usage
5’LTR
tat
rev
vif
gag
vpu
pol
Luc
env
3’LTR
vpr
+
pcDNA-env
CMV
pA
Env
Luciferase assay
CCR5 cells
0.2µ
filter
293T cells
0.2µ
filter
CXCR4 cells
Table 1: Children Demographic and Clinical Characteristics
Characteristics
HAART-Failures (n=41) HAART-Naïve (n=40)
P value
7.9 (4.8-10.4)
0.9 (0.5-2.8)
<0.0001a
Black Race
41 (100.0)
39 (97.5)
0.49b
Male Gender
24 (58.5)
18 (45.0)
0.27b
9.0 (3.1-13.5) (n=33)
14.0 (7.5-22.0) (n=37)
0.008a
Current CD4%, median (IQR)
18.0 (9.0-24.0)
14.0 (7.5-22.0) (n=37)
0.47a
Current CD8%, median (IQR)
51.0 (40.5-58.0)
48.0 (35.5-56.5) (n=37)
0.38a
Current CD3%, median (IQR)
72.0 (67.0-77.0)
66.0 (56.0-77.5) (n=37)
0.18a
4.9 (4.4-5.4)
5.9 (5.6-6.8)
<0.0001a
Age, median years (IQR)
Nadir CD4%, median (IQR)
Current plasma HIV-1 viral load,
median log-10 copies/ml (IQR)
Current WHO Stage:
(n=40)
I
1 (2.5)
0 (0.0)
II
15 (37.5)
1 (2.5)
0.003b
III
18 (45.0)
20 (50.0)
IV
6 (15.0)
19 (47.5)
NOTE. Data are no. (%) of children unless otherwise indicated. For cases where the data is incomplete, the n value is indicated.
Statistical tests: a Mann-Whitney U test and b Fisher’s exact test (for WHO stage analysis, stages I, II and III were grouped together).
Table 1: Patient Demographic and Clinical Characteristics Cont.
Characteristics
HAART-Failures (n=41) HAART-Naïve (n=40)
P value
Current Drug regimen:
D4T, 3TC, EFV
25 (61.0)
D4T, 3TC, LPV/r ●
6 (14.6)
D4T, DDI, EFV *
1 (2.4)
AZT, 3TC, NVP
3 (7.3)
AZT, 3TC, EFV ○
3 (7.3)
AZT, DDI, EFV
1 (2.4)
AZT, DDI, LPV/r
1 (2.4)
D4T, ABC, LPV/r *
1 (2.4)
Duration of HAART prior to study
28.6 (19.7-37.5) (n=38)
recruitment, median months (IQR)
History of single-dose NVP for PMTCT
10 (26.3) (n=38)
18 (47.4) (n=38)
0.09b
NOTE. Data are no. (%) of children unless otherwise indicated. For cases where the data is incomplete, the n value is indicated.
Prior treatment indicated with underlined drug/s changed ● d4T, 3TC, ritonavir (n=1); * unknown; ○ d4T, 3TC, EFV (n=1) and
AZT, 3TC, NVP (n=1); d4T, 3TC, kaletra; d4T, 3TC, EFV.
Statistical tests: a Mann-Whitney U test and b Fisher’s exact test
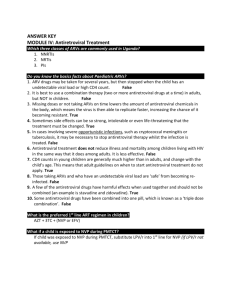
Frequency of drug resistance mutations and levels of resistance in HAART-failing
children to the NRTIs (a) and NNRTIs (b)
58.5% had TAMs
39% had ≥3 TAMs
Average no. of major mutation in patients
failing standard first line treatment (n=30)
• d4T/3TC/EFV (n=25)
– 3 patients have no DRMs (VLs are 617; 79,400; 228,000)
– 20 NRTI DRM
– 2 NNRTI DRM
(one patient had a PI DRM)
• d4T/3TC/kaletra (n=5)
– 3 patients have no DRMs (VLs are 143,000; 198,000; 4,410,000)
– 1 patient has 1 NRTI DRM (M184V) only
– 1 patient has 1 NRTI (M184V) and 1 NNRTI DRM (Y181C)
How many major mutations compromise the
standard second line treatment?
d4T/3TC/EFV (n=25) → AZT/ddI/Kaletra
• 3 patients susceptible to all drugs – no change needed
• All patients susceptible to kaletra
• 3 patients susceptible to 3 drugs in standard second line tx.
AZT Resistance
ddI Resistance
Susceptible (n=2)
High-Level (n=2)
Potential low-level (n=2)
Low level (n=5)
Low-level (n=1)
Intermediate (n=2)
Potential low-level (n=2)
Intermediate (n=8)
Low-level (n=3)
Intermediate (n=2)
High-level (n=1)
High-Level (n=4)
Intermediate (n=2)
High-Level (n=2)
• Overall, 13 of 25 (52%) patients will have some degree of
resistance (low to high) to two of the three drugs in their
new regimen (excluding potential low-level resistance)
d4T/3TC/kaletra (n=5) → AZT/ddI/(NVP/EFV)
• 4 of 5 patients are susceptible to all second line drugs
• 1 patient had intermediate resistance to EFV (3.7 yrs old)(Y181C)
Note: Overall better if not changed
• All still susceptible to PIs and d4T with 3 patients still susceptible to
3TC [2
high-level resistance to 3TC (M184V)]
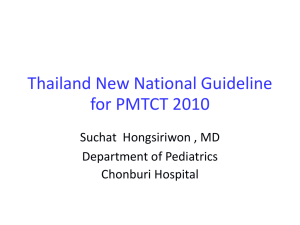
Comparison of coreceptor usage in HAARTfailing and HAART-naïve children
HAART-Naïve
HAART-Failures
HAART-Failures
9.4%
42.9%
42.9%
45.7%
45.7%
R5-tropic
D/M-tropic
R5-tropic
R5-tropic
X4-tropic
X4-tropic
D/M-tropic
D/M-tropic
90.6%
11.4%
11.4%
p<0.0001
Evaluation of Several Genotypic Tools for the Prediction of CXCR4usage
Prediction of CXCR4-usagea
Genotypic Tool
Sensitivity (%) Specificity (%) PPV (%) NPV (%)
aA
11/25 charge rule
30.0
96.9
83.0
74.0
Net V3 charge rule
65.0
78.1
59.0
82.0
C-PSSMsinsi
75.0
87.5
75.0
88.0
Geno2pheno[coreceptor]b
60.0
87.5
70.0
82.0
Combined Rulesc
63.2
100.0
100.0
85.0
C4.5
25.0
100.0
100.0
73.0
C4.5 positions 8-12
25.0
100.0
100.0
73.0
PART
30.0
100.0
100.0
75.0
SVMwetcat
40.0
96.9
86.0
77.0
total of 52 pure subtype C isolates with both phenotypic and genotypic data were included in this analysis. bA false
positive rate of 10% was used. c A combination of the first four genotypic tools were used where the majority prediction
was considered as the final genotype prediction (n=47).
Adult patient information
Patient
HAART-Experienced HAART-Naïve p-value
Characteristic
Patients failing Patients (n=45)
Treatment (n=45)
Age, median years
(Q1-Q3)
Gender: Female
36 (24-51)
36 (20-78)
28 (65%)
27 (60%)
Black race
45 (100%)
45 (100%)
174 (9-718)
57 (3-197)
6, 653
(225-220,010)
123 (8-660)
44,042
(1,702-1,167,759)
32 (71 %)
13 (29 %)
9 (20 %)
36 (80%)
CD4 count, median
3
cells/mm (Q1-Q3)
Current
Nadir
Vial load,
median copies/ml
WHO stage at visit
I-III
IV
0.65
0.036
0.0004
0.001
Patterns of drug
resistance
• What is the outcome of patients failing if started on the
standard second line of treatment without having
genotypic data?
Average no. of major mutation in patients
failing standard first line treatment (n=16)
• d4T/3TC/ (EFV/NVP) (n=16) (Note: 2 on NVP)
– No major PI mutations
– 1.75 NRTI DRM
– 1.69 NNRTI DRM
How many compromise the standard
second line treatment?
d4T/3TC/ (EFV/NVP) (n=16) → AZT/ddI/LPV/r
• All patients susceptible to kaletra (LPV/r)
• 6 patients susceptible to all 3 drugs in standard second line tx.
AZT Resistance
ddI Resistance
Potential low-level (n=3)
Susceptible (n=4)
High-Level (n=1)
Susceptible(n=1)
Potential low-level (n=2)
Low-level (n=1)
Low-level (n=2)
Low-level (n=2)
Intermediate (n=2)
Low-level (n=2)
• 4 of 16 (25%) patients will have some degree of resistance
(low to intermediate) to two of the three drugs in their new
regimen (excluding potential low-level resistance).
• 6 of 16 (37.5%) will have some degree of resistance (low to
high) to one of the three drugs in their new regimen
(excluding potential low-level resistance).
High levels of CXCR4
viruses in patients
failing therapy- limited
salvage options
V3 loop-based methods for coreceptor usage prediction
Method
11/25
Overall net V3 charge
C-PSSM
Geno2Pheno
Combined algorithm*
% of sequences
correctly
predicted
78
75
81
84
87
% of R5
sequences
correctly
predicted
90
71
85
86
90
% of X4/D/M
sequences
correctly
predicted
55
81
72
82
80
*In the combined algorithm, concordant results from at least 3 of 4 methods
(i.e. the amino acids at positions 11 and/or 25, the overall net V3 charge, C-PSSM
prediction and Geno2Pheno prediction) were used.
Conclusions
• Virologic failure is mainly due to DRMs
• High levels of TAMs is source of concern- suggests
subpotimal adherence and need for intensive
monitoring
• Higher levels of CXCR4 using viruses among HAART
experienced patients- need to explore CCR5
antagonists as part of first-line/early treatment
• Collectively, these data highlight the need for
intensified adherence counselling and better HAART
monitoring to maximize benefits.
Acknowledgements
UKZN
Monogram Biosciences
•
•
•
•
•
•
• Jacqueline Reeves
• Yolanda Lie
• Elizabeth Anton
Taryn Green
Ashika Singh
Mohendran Archary
Michelle Gordon
Raziya Bobat
Hoosen Coovadia
McCord Hospital
• Henry Sunpath
• Richard Murphy
Harvard University
• Daniel Kuritzkes
• Bruce Walker
Funding
•
•
•
•
IMPAACT Network, NIH
Harvard University CFAR
South African DST/NRF
Hasso Plattner Foundation
 0
0