NORTHWEST AIDS EDUCATION AND TRAINING CENTER
2013 Asilomar HIV Medical Update
David Spach, MD
Clinical Director, Northwest AETC
Professor of Medicine, Division of Infectious Diseases
University of Washington
Last Updated: October 21, 2013
2013 Asilomar Update
New Occupational PEP Guidelines
Dolutegravir (Tivicay)
Hepatitis C Update
Occupational PEP 2013 Guidelines
2013
Source: Kuhar DT, et al. Infect Control Hosp Epidemiol. 2013;34:875-92.
Case History
HIV Exposure in a Health Care Worker
• A 41-year-old male nurse has a needlestick injury on his left
thumb. The site bled for about 2 minutes after the injury. The
source patient has documented HIV infection, has never taken
antiretroviral medications, and most lab studies showed HIV RNA
level of 2,350 copies/ml and CD4 count of 658 cells/mm3.
• Based on USPHS 2013 Guidelines, what is recommended?
A. 2 drugs: Zidovudine-lamivudine
B. 2 drugs: Tenofovir-emtricitabine
C. 3 drugs: Tenofovir-emtricitabine + Raltegravir
D. 3 drugs: Tenofovir-emtricitabine + Darunavir + ritonavir
2013 USPHS Occupational PEP Guidelines
Number of Antiretroviral Medications to Use
“As less toxic and better-tolerated medications for the
treatment of HIV infection are now available… the PHS
working group recommends prescribing 3 (or more)
tolerable drugs as PEP for all occupational
exposures to HIV.”
Source: Kuhar DT, et al. Infect Control Hosp Epidemiol. 2013;34:875-92.
2013 USPHS Occupational PEP Guidelines
Recommendations for Antiretroviral Regimens
Recommended Antiretroviral Regimens for Occupational PEP (28-Day Duration)
Preferred Regimen
INSTI
NNRTI
Raltegravir (Isentress) Tenofovir-Emtricitabine (Truvada)
400 mg twice daily
1 pill daily
Source: Kuhar DT, et al. Infect Control Hosp Epidemiol. 2013;34:875-92.
Pill Burden
Case History
HIV Exposure in a Health Care Worker
• A 32-year-old physician has a needlestick injury on her
hand that involves an HIV-infected patient. The source
patient is taking tenofovir-emtricitabine-efavirenz (Atripla)
and had an undetectable HIV RNA level 3 months prior.
• Based on USPHS 2013 Guidelines, would you
recommend antiretroviral PEP for this physician?
2013 USPHS Occupational PEP Guidelines
PEP when Source Patient has Undetectable HIV RNA Level
“Exposure to a source patient with an undetectable
serum viral load does not eliminate the possibility of HIV
transmission or the need for PEP and follow-up testing.
While the risk of transmission from an occupational
exposure to a source patient with an undetectable
serum viral load is thought to be very low, PEP
should still be offered.”
Source: Kuhar DT, et al. Infect Control Hosp Epidemiol. 2013;34:875-92.
HIV Occupational Postexposure Prophylaxis
What are situations in which expert consultation is advised?
2013 USPHS Occupational PEP Guidelines
Situations for Which Expert Consultation Advised
• Delayed exposure report (eg. longer than 72 hours)
• Unknown source (eg. needle in sharps disposal)
• Known or suspected pregnancy in exposed person
• Exposed person breast-feeding
• Known or suspected ARV drug resistance in source patient
• Serious medical illness in exposed persons
• Toxicity occurring in exposed person taking PEP regimen
Source: Kuhar DT, et al. Infect Control Hosp Epidemiol. 2013;34:875-92.
Post-Exposure Prophylaxis Line (PEPline)
888-448-4911
Sou
2013 USPHS Occupational PEP Guidelines
Baseline and Follow-Up for Occupational PEP
• Early Reevaluation after Exposure (within 72 hours)
• Baseline and Follow-up HIV Testing
- Baseline HIV testing
- Follow-up HIV testing 6, 12, and 24 weeks after exposure
- Follow-up HIV testing at 6 and 16 weeks if 4th generation assay* used
• Baseline and Follow-up Laboratory Testing
- Baseline renal and hepatic function tests
- Follow-up renal and hepatic function tests at 2 weeks
*4th generation combination assay = HIV p24 antigen-HIV antibody test
Source: Kuhar DT, et al. Infect Control Hosp Epidemiol. 2013;34:875-92.
Occupational HIV Postexposure Prophylaxis
Suggestions for Training
A. Incorporate Occupational PEP into Larger Trainings
B. Provide 3 Point Takeaway Training
(1) When PEP given, use 3 or more ARV drugs
(2) Use Tenofovir-emtricitabine + Raltegravir
(3) Know when and how to get expert consultations
C. Give trainees PEPLine information/pamphlet
Dolutegravir (Tivicay)
Raltegravir (Isentress) & Dolutegravir (Tivicay)
Tablet Size
Raltegravir
Source: Slide courtesy of Brian Wood, MD.
Dolutegravir
Dolutegravir
Recommended Dolutegravir Dosing
Adult Population
Recommended Dose
Treatment-naïve
or
Treatment-experienced INSTI-naïve
50 mg once daily
Coadministered with potent UGT1A/CYP3A inducer:
Efavirenz
Fosamprenavir/ritonavir
Tipranavir/ritonavir
Rifampin
50 mg twice daily
INSTI-experienced with certain INSTI mutations*
or
Clinically suspected INSTI resistance
50 mg twice daily
Poor virologic response associated with Q148 Substitution plus ≥ 2 more INSTI mutations
Source: Dolutegravir Prescribing Information
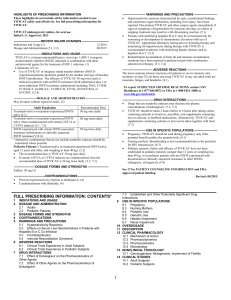
Dolutegravir Increases Serum Creatinine by Benign Inhibition
of Tubular Secretion of Creatinine
Bowman’s Capsule
Proximal Tubule
Distal Tubule
Organic Cation Transporter 2
(OCT2)
Dolutegravir
Collecting
Tubule
Inhibits tubular secretion of
creatinine via inhibition of OCT2
Loop of Henle
Excretion
Source: Koteff J, et al. Br J Clin Pharmacol. 2013:75:990-6.
Dolutegravir (Tivicay)
Should dolutegravir replace raltegravir in clinical practice?
Dolutegravir Phase 3 Studies
Study
ARV History
Comparison
Results
1 SPRING-2
ARV-Naïve
Dolutegravir QD vs.
Raltegravir
• Non-inferior
(88% vs. 85%)
2 SINGLE
ARV-Naïve
Dolutegravir QD vs.
Efavirenz
✔ Dolutegravir superior
(88% vs. 81%)
3 FLAMINGO
ARV-Naïve
Dolutegravir QD vs.
Darunavir-RTV
✔ Dolutegravir superior
(90% vs. 81%)
4 SAILING
>2-class
ARV resistance
Dolutegravir QD vs.
Raltegravir
✔ Dolutegravir superior
(71% vs. 64%)
5 VIKING-3
Integrase
resistance
Single-arm,
Dolutegravir BID
• Virological suppression
(64%)
(1) Raffi F, et al. Lancet 2013;381:735-43.
(2) Walmsley S. 52nd ICAAC 2012. Abstract H556b.
(3) Feinberg J, et al. 53nd ICAAC. 2013: Abstract H-146-a.
(4) Cahn P, et al. Lancet 2013;382:700–8.
.
(5) Nichols G, et al. 7th Conference IAS 2013: Abstract TULBPE19.
Dolutegravir + 2NRTIs versus Darunavir-RTV + 2NRTIs
FLAMINGO: Design
Study Design
Protocol
- Open-label, randomized study
- Phase 3 trial
- Antiretroviral-naïve patients
- Treatment Arms
Dolutegravir* (QD) + 2NRTIs
Darunavir* + RTV (QD) + 2NRTIs
- NRTIs
Tenofovir-emtricitabine
Abacavir-lamivudine
Dolutegravir + 2NRTIs
(n = 242)
Darunavir + 2NRTIs
*Dolutegravir dose = 50 mg once daily; Darunavir dose = 800 mg once daily
Source: Feinberg J, et al. 53nd ICAAC. 2013: Abstract H-146-a.
(n = 242)
Dolutegravir + 2NRTIs versus Darunavir-RTV + 2NRTIs
FLAMINGO: Result
Week 48 Virologic Response
Source: Feinberg J, et al. 53nd ICAAC. 2013: Abstract H-146-a.
Dolutegravir
Does the NRTI backbone with dolutegravir matter?
Tenofovir-emtricitabine
Abacavir-lamivudine
Dolutegravir + 2NRTIs versus Darunavir-RTV + 2NRTIs
FLAMINGO: Result
Week 48 Virologic Response: Background Dual NRTI Therapy
Source: Feinberg J, et al. 53nd ICAAC. 2013: Abstract H-146-a.
Dolutegravir-ABC-3TC versus Efavirenz-TDF-FTC
SINGLE: Result
Week 48 Virologic Response
Source: Walmsley S, et al. 52nd ICAAC. 2012: Abstract H-556-b.
Dolutegravir + 2NRTIs versus Raltegravir + 2NRTIs
SPRING-2: Result
Week 96 Virologic Response: Background Dual NRTI Therapy
Source: Raffi F, et al. 7th IAS. 2013. Abstract TuLBPE17.
Dolutegravir + 2NRTIs versus Raltegravir + 2NRTIs
SPRING-2: Result
Week 96 Virologic Response: Background Dual NRTI Therapy
Source: Raffi F, et al. 7th IAS. 2013. Abstract TuLBPE17.
Dolutegravir + 2NRTIs versus Raltegravir + 2NRTIs
SPRING-2: Result
Week 96: Background Dual NRTI Therapy in Patients on Dolutegravir
Source: Raffi F, et al. 7th IAS. 2013. Abstract TuLBPE17.
Major Pathways of Resistance with Raltegravir
Raltegravir
Early
N155H
Delayed
Q148H/K/R
Secondary Mutations
(L74M, E92Q, T97A, V151I, G163R)
Secondary Mutations
(L74M, G140A/S, E138K)
Source: Fransen S, et al. J Virol. 2009;83:11440-6.
Integrase Resistance Testing
• Integrase Genotype ✔
- Quest Diagnostics
- Lab Corp (Monogram Biosciences)
- Virco
• Integrase Phenotype
- Lab Corp (Monogram Biosciences)
- Virco
Dolutegravir in Treatment-Experienced with Integrase Resistance
VIKING-3
Study Design
Protocol
- HIV-infected adults with
VL >500 copies
- Resistance to raltegravir
or elvitegravir, plus
resistance to at least 2
additional ARV classes
Dolutegravir
50 mg BID
+ Failing Regimen
Dolutegravir
50 mg BID
+ OBT
Functional monotherapy
phase (7 days)
Day 8
Sources: 1) ViiV Healthcare Press release. Nov 2012. 2) Nichols G et al. IAS 2013.
3) http://www.viivhealthcare.com/media/58599/us_tivicay.pdf
Dolutegravir in Patients with Raltegravir Resistance
VIKING-3: Results
*without additional INSTI mutations
Source: Dolutegravir Product Information.
Dolutegravir Discussion
How should we use dolutegravir in clinical practice?
- In treatment naïve?
- In treatment experienced (intregrase naïve)?
- In treatment experience and integrase resistant?
Use of Dolutegravir
• Treatment naïve
- Excellent first line agent
- Likely will become a preferred agent in DHHS Guidelines
• Treatment experienced (Integrase-naïve)
- Attractive as component of salvage regimen
• Treatment experience (Integrase resistant or experienced)
- Parameters for once or twice daily dosing poorly defined
- Avoid use with Q148 + ≥ 2 secondary mutations
Hepatitis C Update
Hepatitis C Epidemiology in United States
Annual Deaths from HCV?
.
Age-Adjusted Mortality Rates* from HBV, HCV, & HIV
United States, 1999-2007
7
Rate per 100,000 PY
HIV
n = 15,106
6
5
4
Hepatitis C
3
2
1
Hepatitis B
0
1999
2000
2001
2002
2003
Year
*Mortality Rates = HBV, HCV, HIV listed as cause of death
Source: Ly KN, et al. Ann Intern Med. 2012:156:271-8.
2004
2005
2006
2007
Forecasted 2010-2060 Annual HCV-Related Deaths in the United States
Persons with Chronic Hepatitis C and no Cirrhosis in 2005
45,000
Deaths
40,000
35,000
Number
30,000
25,000
20,000
15,000
10,000
5,000
0
2010 2014 2018 2022 2026 2030 2034 2038 2042 2046 2050 2054 2058
Year
Source: Rein DR, et al. Dig Liver Dis. 2011:43:66-72.
Hepatitis C Cascade of Care in United States
100%
50%
35%
9%
Source: Holmberg SD, et al. N Engl J Med. 2013;368:1859-61.
6%
HCV-HIV Coinfection
HIV-Infected Persons in United States
HIV
Monoinfection
Source: Sulkowski M, et al. Ann Intern Med. 2003;138:197-207.
HIV-HCV
Coinfection
Cause of Death (Incidence) in the D:A:D Study
N = 1,246 deaths
Source: Weber R, et al. Arch Intern Med. 2006;166:1632-41.
Testing for Hepatitis C
• A 34-year-old man is diagnosed with HIV infection. His
risk factor for acquiring HIV is having sex with other
men. He has about 8-10 male sexual partners per
year.He has never injected drugs. His CD4 count is 684
cells/mm3. He is referred for routine HIV care.
• At his initial evaluation, should you test this patient
for hepatitis C infection?
• If the HCV antibody test is negative, should he have
repeat testing?
Entry into Care
Recommendations for HCV Testing
“On entry into HIV care, all HIV-infected patients should
undergo routine HCV screening.”
Source: 2013 Opportunistic Infections Guidelines. AIDS Info. (www.aidsinfo.nih.gov)
Recommendations for Repeat Testing
for Hepatitis C in HIV-Infected Persons
“For at risk HCV-seronegative persons, HCV antibody testing
is recommended annually or as indicated by risk exposure.”
Source: Page R-2. 2013 Opportunistic Infections Guidelines. AIDS Info. (www.aidsinfo.nih.gov)
Hepatitis C and Cure
Why can antiviral cure hepatitis C but not HIV?
Sustained Virologic Response (SVR) with HCV Treatment = Cure
Comparative Treatment Goals with Antiviral Therapy
HIV
HBV
HCV
(latent reservoir)
(latent reservoir)
(no latent reservoir)
HCV RNA
ccDNA
Proviral DNA
Host DNA
Host DNA
Host DNA
Host Cell
Host Cell
Host Cell
Lifelong suppression
of viral replication
Long-term reduction
of viral replication
Source: Kieffer TA, et al. J Antimicrob Chemother. 2010:65:2012-12
Definitive
Viral Clearance
Therapy for Hepatitis C
Milestones Prior to Use of Direct Acting Agents ( DAAs)
Timeline
1986
1998
2001
2002
Therapy for Hepatitis C
Projected SVR Rates with Multiple DAAs
Timeline
2011
2014
2015
Simeprevir: October 24, 2013
Sofosbuvir: October 25, 2013
Hepatitis C Virus
Genome
HCV Genome
5’
3’
Structural
Non-Structural
Hepatitis C Virus
Translation
HCV Genome
5’
3’
Structural
Non-Structural
Translation
C
E1
E2
p7
NS2
NS3
A
NS4
B
A
Polyprotein Precursor: ≈ 3,000 amino acids
NS5
B
Hepatitis C Virus
Protein Processing
HCV Genome
Translation
Polyprotein Precursor
C
E1
E2
p7
NS2
NS3
A
NS4
B
A
NS5
B
Protein Processing
Proteins
C
E1
E2
p7
NS2
NS3
NS4
A
NS4B
NS5A
NS5B
Hepatitis C Virus
Structural and Nonstructural Proteins
Hepatitis C Proteins
Structural Proteins
C
E1
Nucleocapsid
Envelope
Glycoprotein
E2
Nonstructural (NS) Proteins
p7
Envelope
Glycoprotein
NS2
NS3
Cysteine
Protease
Vioporin
NS4
A
NS4B
Protease
Cofactors
Protease
RNA
Helicase
NS5A
NS5B
RNA binding and assembly
recognition complex
Membranous
Web
Induction
RNA-Dependent
RNA Polymerase
Hepatitis C Virus
Direct Acting Agents (DAAs)
Hepatitis C Proteins
Structural Proteins
C
E1
E2
Nonstructural (NS) Proteins
p7
NS2
NS3
NS4
A
NS4B
NS5A
NS5B
RNA binding and assembly
recognition complex
Protease
Protease
Cofactors
RNA-Dependent
RNA Polymerase
Hepatitis C Virus
Direct Acting Agents (DAAs)
Hepatitis C Proteins as Antiviral Targets for DAAs
NS3
NS4A
NS3/4A
Protease Inhibitors
NS5A
NS5A Inhibitors
NS5B
NS5B
Polymerase Inhibitors
NRTIs NNRTIs
Future HCV Direct Acting Agents (DAAs)
NS3
NS4A
NS5A
NS5B
Protease Inhibitors
NS5A Inhibitors
Polymerase Inhibitors
Asunaprevir
Daclatasvir
Mericitabine
Danoprevir
Ledipasvir
Sofosbuvir
Faldaprevir
ABT-267
ABT-333
Simeprevir
IDX-719
BMS-791325
Vaniprevir
ABT-450/r
BI-207127
Sofosbuvir
• Investigational
- FDA Advisory Panel meeting October 25, 2013
• Class & Mechanism
- NS5B nucleotide analogue polymerase inhibitor
- Pan genotypic
• Sofosbuvir Dosing
- 400 mg PO once daily
• Clinical Use
- GT 2 (?3): In combination with ribavirin alone (dual therapy)
- GT 1,4,5,6: in combination with peginterferon + ribavirin (triple therapy)
• Drug Interactions and Adverse Effects (AE)
- Minimal drug interaction
- Well-tolerated
Sofosbuvir: Summary of Key Studies
HCV Monoinfection
• Phase 3 Trials in Treatment Naive
- NEUTRINO: Sofosbuvir + PEG + RBV; GT 1,4,5,6
- FISSION: Sofosbuvir + RBV vs. PEG + RBV; GT 2,3
- POSITRON: Sofosbuvir + RBV; GT 2,3; Interferon intolerant
• Phase 3 Trials in Treatment Experienced
- FUSION: Sofosbuvir + RBV for 12 vs. 16 weeks; prior Rx failure; GT 2,3
• Phase 2 Trials in Treatment Naïve
- NIAID: Sofosbuvir + RBV; GT 1; Unfavorable baseline characteristics
HCV Monoinfection
Sofosbuvir in Treatment-Naïve Genotypes 1,4,5,6
NEUTRINO Trial*
*Note: Published in tandem with FISSION Trial (Genotypes 2,3)
Sofosbuvir for Chronic Untreated HCV Infection (GT 1,4,5,6)
NEUTRINO
Week
N =327
0
12
Sofosbuvir + PEG + RBV
Drug Dosing
Sofosbuvir 400 mg once daily
Peginterferon alfa-2a = 180 µg once weekly
Ribavirin (weight-based): 1000 mg if < 75kg or 1200 mg/day if ≥ 75kg
Source: Lawitz E, et al. N Engl J Med. 2013;368:1878-87.
24
SVR12
Sofosbuvir for Chronic Untreated HCV Infection (GT 1,4,5,6)
NEUTRINO: SVR12 by Genotype
• Percentage of Patients with SVR
GT = genotype
Source: Lawitz E, et al. N Engl J Med. 2013;368:1878-87.
Sofosbuvir for Chronic Untreated HCV Infection (GT 1,4,5,6)
NEUTRINO: SVR12 by Race
• Percentage of Patients with SVR
Source: Lawitz E, et al. N Engl J Med. 2013;368:1878-87.
Sofosbuvir for Chronic Untreated HCV Infection (GT 1,4,5,6)
NEUTRINO: SVR12 by Presence of Cirrhosis
• Percentage of Patients with SVR
Source: Lawitz E, et al. N Engl J Med. 2013;368:1878-87.
HCV Monoinfection
Sofosbuvir in Treatment-Naïve Genotypes 2,3
FISSION Trial*
*Note: Published in tandem with NEUTRINO Trial (Genotypes 1,4,5,6)
Sofosbuvir and Ribavirin for Chronic Untreated HCV
FISSION Trial
Week
N =256
N =243
0
12
Sofosbuvir +
RBV (weight-based)
24
SVR12
Peginterferon + RBV (fixed dose)
Drug Dosing
Sofosbuvir 400 mg once daily
Peginterferon alfa-2a = 180 µg once weekly
Ribavirin (weight-based): 1000 mg if < 75kg or 1200 mg/day if ≥ 75kg
Ribavirin (fixed dose): 800 mg/day divided BID
Source: Lawitz E, et al. N Engl J Med. 2013;368:1878-87.
36
SVR12
Sofosbuvir for Chronic Untreated HCV Infection GT 2,3
FISSION Study: Results
SVR12 (by Genotype)
RBV = Ribavirin; PegIFN = Peginterferon
Source: Lawitz E, et al. N Engl J Med. 2013;368:1878-87.
Sofosbuvir in HIV-Infected
Sofosbuvir
Key Summary Points
• Major impact drug for hepatitis C treatment
• Active against all HCV genotypes
• Option for interferon-free treatment of GT2 (?GT3)
• Excellent results with most difficult to treat GT-1 patients
• Safe, convenient, potent, and minimal drug interactions
• Optimal approach with sofosbuvir and genotype 3 uncertain
• Likely will be very safe and effective in HIV-infected patients
• Payment/reimbursement with HIV-infected unknown
Simeprevir
• Investigational
- FDA application submitted March 2013
- FDA Advisory Committee meeting on October 24, 2013
• Class & Mechanism
- NS3/4A protease inhibitor
- Multi-genotypic activity against genotypes 1,2,4,5 and 6.
• Simeprevir Dosing
- 150 mg PO once daily
- In combination with peginterferon + ribavirin (triple therapy)
• Adverse Effects (AE) attributable to Simeprevir
- Reversible hyperbilirubinemia (due to interference with
OATP1B1/MRP2 transporters)
Simeprevir and Peginterferon plus Ribavirin for Chronic HCV
QUEST-1 Trial
Week
12
0
24
Randomized 2:1,
stratified on IL28B
and HCV subtype
N = 264
N =130
Simeprevir
+ PEG + RBV
Placebo
+ PEG + RBV
48
Response-guided therapy: Patients with
extended RVR (HCV RNA <25 IU/ml at
weeks 4 and 12) were allowed to stop
treatment after 24 weeks.
PEG + RBV
PEG + RBV
PEG + RBV
Drug Dosing
Simeprevir 150 mg once daily
Peginterferon alfa-2a (PEG): 180 mcg/week
Ribavirin (RBV) weight-based: 1000 mg if < 75 kg or 1200 mg/day if ≥ 75kg
Source: Jacobson I, et al. 48th Annual Meeting of EASL. Abstract 1425.
Simeprevir and Peginterferon plus Ribavirin for Chronic HCV
QUEST-1 Results
Proportion of Patients with SVR12
P < 0.001
Abbreviations: SVR12 = sustained virologic response at 12 weeks; PEG = peginterferon; RBV = ribavirin
Source: Jacobson I, et al. 48th Annual Meeting of EASL. Abstract 1425.
Simeprevir
Key Summary Points
• Modest impact drug for hepatitis C treatment
• Similar to boceprevir and telaprevir but ONCE DAILY
• Future use likely as component of multi-DAA therapy
• Payment/reimbursement with HIV-infected unknown
Hepatitis C: Key Points
• Revolution in Treatment
- Cure ≈ 90% of GT1 with 12-week therapy
- Cure ≈ 90% GT2 with all 12-weeks all-oral therapy
- Future all-oral therapy will have cure > 90% for all GTs
• Dramatic improvements needed in HCV cascade of care
• Unknown how quickly new meds available for HIV
End