Pseudomonas & Other Non

Pseudomonas
&
Other Non-fermenters
Professor Sudheer Kher
KEY WORDS
• Pseudomonas aeruginosa
• Pigments
– Pyocyanin
– Fluorescein
• Toxin A
• Opportunistic Infections
• Greenish Pus
• Non-fermenter
• Oxidase positive
• Motile
• Hospital infection
• Antibiotic resistance
Pseudomonas
•
Obligate Aerobe, mostly saprophytic
•
Gram-negative non-sporing rods
•
Motile
•
Majority of human infections
– P. aeruginosa
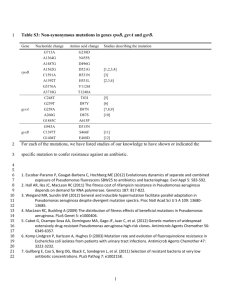
Medically important species of
Pseudomonas
Pigment production
Greenish yellow pigment
No pigment
Pseudomonas aeruginosa Burkholderia mallei
Burkholderia pseudomallei
Common in the environment
•
water
•
air
•
soil
P. aeruginosa and compromised host
•
Burns and wounds
– destruction of blood vessels
– phagocyte access limited
•
Cancer
– cytotoxic drugs
* destroy the immune system
•
Cystic fibrosis
– altered respiratory epithelium
– pneumonia
Cystic fibrosis ( CF ) is a hereditary disease that affects mainly the lungs and digestive system, causing
. pancreas , this entity has increasingly been labeled simply cystic fibrosis .
[1] Average life expectancy is around 37 years, although improvements in treatments mean a baby born today could expect to live longer.
[2]
Identification
•
Pigments
–
Pyocyanin (blue-green)
–
Fluorescein (green-yellow, fluorescent)
– Best produced in King’s A & B Media
•
Biochemical reactions – Non fermenter
•
Oxidase positive
•
Cultures have fruity smell (Grape like)
Pathogenesis
•
Toxin A - ADP ribosylates EF2 functions as NADase
– similar to diphtheria toxin
•
Slime layer is anti-phagocytic
Virulence factors of P. aeruginosa
• Lipopolysaccharide: endotoxin, pyrogen
• Capsule: anti-phagocytosis, inhibits complement fnc.
• Proteases: damage host proteins such as complement and IgA
• Hemolysins
• Exotoxin A: a diptheria-like toxin - toxic for macrophages
• Pyocyanin: impairs ciliary activity
• Fimbriae: adherence factor
• Other non-pilus adhesins
• Others like elastases………..
Source
Exogenous
Pathogenesis
Endogenous (skin of axilla, perineum or GIT)
Respirators, bed pans, lotions, ointments, eye drops, stock of distilled water, disinfectants (QAC)
Transmission Endogenous infection Contact spread
Virulence Toxin and Extracellular products
Protease , Pyocyanin, Cytotoxin (leukocidin)
Endotoxin, Haemolysin, Exotoxin A & Exotoxin S
Mucoid strains in Cystic fibrosis due to alginate
Diseases (Pathogenicity)
Community Suppurative Otitis
Nosocomial infection Hospital
Eye Keratitis and Endophthalmitis
Ear
Skin
UTI
RTI
GIT
CNS
Otitis externa and Otitis media
Burns infection, wound sepsis
Ecthyma gangrenosum
Cystitis (catheterized)
Pneumonia (ventilation / tracheostomy)
Infantile diarrhea
Meningitis brain abscess (iatrogenic)
Lab Diagnosis
Wound discharge, sputum, urine, blood Specimens
Microscopy Gram negative bacilli
MAC
NA
NLF, blue green with distinct feathered edges
Green diffusible pigment
Cetrimide agar
Selective media
Identification tests
Oxidase + TSI: K- / K(non fermenter)
AST
Bacteriophage typing
Ceftazidime, ticarcillin, piperacillin, ciprofloxacin, amikacin, gentamicin, Polymyxin B
Hospital outbreak investigation
Aeroginocine
(Pyocine) typing
11 Indicator strains
Phage Typing
Treatment & Control
Antipseudomonad beta lactam
Aminoglycosides
Fluoroquinolones
Combination therapy in impaired defense mechanism
Strict attention to asepsis
Treatment of underlying disease
(correction of granulocytopenia)
• 8:10 PM Atul: are you there
• me: Hi
• Atul: hi
• 8:11 PM me: That day I came on line in d evening but by that time u were off! How's life?
• Atul: did i tell you about isolation of burkholderia pseudomallei at dharwad me: Saw my mail?
• 8:12 PM Atul: yha me: No. Just now I am preparing my power point on that very topic. May be I can use ur story to make lecture interesting!
• 8:13 PM Atul: please send me as many full text articles you can on this topic.\ sure i will send you the case report. when do you want it
• 8:14 PM me: Certainly. Can u send me a brief summary. May be tomorrow a real brief one.. but incl all essentials.
• Atul: sending it now
• 8:15 PM me: Wonderful. The students will like it and I will mention the co-incidence that my friend was talking of exactly the same organism!! Telepathy?
Burkholderia pseudomalai septicaemia – a case report
• A 35 old male working as daily labourer presented to the
Medicine OPD on 19th September 2007 at 1 pm with complaint of fever for 8 days and reduced urine output for about one month. He was known diabetic and was on regular insulin therapy of which precise duration could not be known. He belonged to the costal town Karwar of
Karnataka, India.
• On examination the patient was emaciated and dehydrated. His blood pressure was 70 mm / 50 mm of
Hg and pulse rate was 120 per minute. CVS examination revealed S1 S2. On auscultation he showed bilateral basal crepitations. There was a vertical scar on the abdomen and the patient gave history of splenectomy 10 years ago of which reason was not identified. Liver was palpable one finger below costal margin and he had mild ascitis. Samples were sent for investigation including blood culture and he was put on Metrogyl (Dose) and
Monocef 1 gm i/v.
Burkholderia pseudo mallei
Whitmore’s bacillus
No pigment, motile
Cause Melioidosis (glanders like disease)
Acute septicemia (typhoid like disease)
Multiple abscess formation
Transmitted via rats either by rat fleas or food contaminated with excreta
B urkholderia mallei
No pigment, non motile
Cause Glanders in horses, donkeys and mules
Rarely cause human disease (suppurative lesions)
Stenotrophomonas maltophilia
(cont.)
EPIDEMIOLOGY
Hospital Epidemics from Contaminated Moist
Reservoirs:
Disinfectant solutions
Respiratory equipment
Ice machines
Flower vases
Risk Factors
Hospitalization
Impaired host defense mechanisms (e.g., highly immunocompromised)
Long-term broad-spectrum antibiotics (e.g., bone marrow transplant patients)
REVIEW
Acinetobacter baumanii (calcoaceticus)
CLINICAL SYNDROMES
Respiratory tract
Urinary tract
Wounds
Septicemia
Opportunistic Infections
EPIDEMIOLOGY
Niches Include:
Natural environments
Moist surfaces in hospitals (e.g., respiratory therapy equipment)
Dry surfaces (e.g., human skin); rare for gram-negative bacilli
Occasionally normal flora in oropharynx
TREATMENT, PREVENTION & CONTROL
Antibiotic Resistance Common
Empirical Treatment for Acute Infections: β-lactam +
Aminoglycoside
Specific Therapy According to Antibiotic Susceptibility
REVIEW
Moraxella catarrhalis
GENERAL OVERVIEW
Formerly classified as Neisseria & more recently Branhamella
CLINICAL SYNDROMES
In Elderly Patients with Chronic Pulmonary Disease
Bronchitis
Bronchopneumonia
In Previously Healthy People
Sinusitis
Otitis
TREATMENT, PREVENTION, AND CONTROL
Most strains produce
β-lactamase; Penicillin Resistant
REVIEW
KEY WORDS
• Pseudomonas aeruginosa
• Pigments
– Pyocyanin
– Fluorescein
• Toxin A
• Opportunistic Infections
• Greenish Pus
• Non-fermenter
• Oxidase positive
• Motile
• Hospital infection
• Antibiotic resistance