Chronic HIV Care with ART
CHALLENGES TO SELF-MANAGEMENT
AND QUALITY CHRONIC CARE
The acute care paradigm
- Reactive care
- Patient who is in office now
- Little continuity
- Diagnose and treat
- No time
- Competing demands
- Physician centered
- No system or infrastructure
- Self-Management: “Not my role”
Institute of Medicine & Committee on Quality of Health Care in America (2001)
“Crossing the Quality Chasm: A New Health System for the 21st Century; National Academy Press
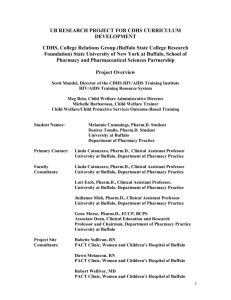
CHRONIC (PLANNED)
CARE MODEL
Acute Care
Planned Care
Reactive
Proactive
Visit Based
Population Based
Little Continuity
Planned - Schedule
Diagnose and Treat
Assess and Support
Physician Centered
Patient Centered
Directed to “Urgent”
Directed to Major Causes
Disease
Wagner E, et al. (1996) Milbank Quarterly 74(4):511-544
Transition to good chronic HIV
care
Common current
situation:
Health services
provide episodic
acute care for HIV
complications.
[Exception: TB]
Patient-held
records for each
acute episode
Only organized
chronic care is
home-based
To introduce and
scale-up ART:
Need to establish
good chronic HIV care
in facility
Good care by an
individual doctor or
specialist does not
replace the need for
establishing good
chronic care with a
clinical team!
Patient HIV care/ART
record and registers,
Sequence of care
Task Shifting
Allows non-doctors to play a significant role in
HIV care/ART
both in peripheral facilities and on the district
clinical team
Central
or Provincial
Specialised referral
(physicians)
District
Supervision and referral
services provided by doctors
and/or medical officers
Health Centre
First-line treatment and care provided by nurses,
clinical officers and ART Aid on clinical team
Community Support
Care and support provided by treatment
supporters, community health workers
and care givers from within the community
Community Preparedness
Mobilization and sensitization to increase treatment
literacy of community
Consider task shifts to allow scale-up
Care, treatment & prevention
Specialized physicians to
doctors
Doctors to nurses
Nurses to PLHA HIV care/ART
aids—education, psychosocial
support, adherence
preparation and support can
be taught to PLHA, other lay
providers, nursing assistants
Clinical team to patient:
Self-management
Clinical team to community- for
treatment support, drug refills,
simple monitoring
Training
Expert patient-trainers
Patient tracking- treatment
card to register, monthly report
PLHA on ART
Present cases, provide
feedback to health workers
Choose those who like
particular aptitude
PLHA, other lay providers or
nursing assistants
Build functional clinical teams
within a district system
Technical basis for task shifts
Emphasize safety
Validate ability to make critical decisions
by validation studies (during guideline
development)
case review, close supervision, monitoring
(during implementation)
ART Aid
Increased need of HR in the context of
scale up
ART Aids (counsellors, health educators,
PLWA) are often more effective than
doctors and health officers/clinical officers
at patient education and adherence
support.
Basic ART Aid Course is designed for
people with little or NO clinical
background—LAY PROVIDERS can
become ART Aid
ART Aid
speaks the same language
patient as the patient
comes from the community to
the clinical team
is a link with the community
knows what is available at
community level
progressively learns what is
needed at community level for
ART and HIV care scale up
inform patients and the rest of
the clinical team on the
community services
advocates with community
stakeholders
Roles of the Basic ART Aid
Adherence preparation (includes ART
preparation and initiation)
Monitoring and supporting patients on ART
Post-test and on-going psychosocial
support
Patient education on HIV/AIDS,
disclosure, prevention, and positive living
in the context of clinical care
Triage
Peer support
WHO Basic ART Aid Training
Course
Index
Section 1
Introduction to the BASIC ART Aid course
Section 2
Roles and responsibilities of the ART Aid as part of the clinical team
Section 3
Care for HIV/AIDS
Section 4
Communication skills
Section 5
Treatment available for HIV/AIDS: cotrimoxazole and ART
Section 6
Adherence preparation
Section 7
Adherence initiation
Section 8
Adherence monitoring and support
Section 9
Prevention in the context of clinical care
Section 10
Disclosure
Section 11
Post-test and ongoing support
Section 12
Positive living
Section 13
Triage
What is needed to integrate community
members more effectively?
Lay provider needs to
"formally" integrated
in the health system
with regular jobs as
trainers and ART Aid.
"Emergency" policy
decisions to create
new posts for LP in
the context of the
clinical team and for
community support
3 levels/approaches to community
Integrated management of HIV/AIDS at
facility with linked community
interventions: prevention, treatment and
care (IMAI/IMCI)
Systems for facility-community links: home visits,
trace patients, monitoring, refills, back-up to homebased care
CHW training
Peer support groups- trained facilitators
Use of same patient education flipchart
Caregiver booklet
Targeted community interventions with
outreach: sex workers, IDU, MSM, others
Broad-based community prevention and
treatment preparedness