Group 2
advertisement

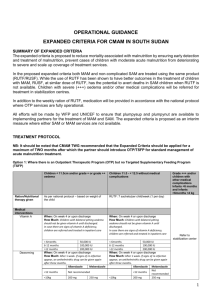
Severe Acute Malnutrition Strategy in Oromiya Region, Ethiopia Case Competition Group 2 Achieving MDGs for Global Health Summer School School of Public Health Fudan University - 2014 Group 2 members Supervisor: Dr. Jiang Hong (Fudan University) Name Institution Anissa Rizkianti University of Sydney Qin Xianjing Guangxi Medical University Fang Liang Central South University Yang Wei Fudan University Xuan Xiuchen Harbin Medical University 8/04/2015 2 Outline • Severe acute malnutrition – Introduction – Definition of severe acute malnutrition – Current situation in Oromiya region – Prevention strategy • Project proposal – Study design – Objectives – Sample – Outcomes – Intervention – Budget allocation • Limitations and challenges • Recommendations 8/04/2015 3 SEVERE ACUTE MALNUTRITION IN OROMIYA, ETHIOPIA 8/04/2015 4 8/04/2015 5 Oromiya, Ethiopia • Total population: 28,067,000, with only 14 percent lives in urban areas (Ethiopia Demography and Health, 2008). • Economy: – Major national income: agriculture • Coffee (50-60% of total exports) • Crops (cereal, pulses and oil crops) – Vulnerable to food shortages due to natural disaster (flooding, droughts) • Education level: – Literacy rate: 36% (2004), male > female, female literacy in rural only 17% – Education attainment: 66% of females with no education, with less than 2% completed primary and secondary leve • Health worker: – Ratio of health workers: 3 per 10,000 – Ratio of public health workers: <0.5 per 10,000 8/04/2015 6 Life Expectancy of Ethiopia Source: World Health Statistics 2009 8/04/2015 7 Trends of Childhood Mortality in Ethiopia 8/04/2015 8 Malnutrition among Under-five Children in Ethiopia Source: Ethiopia DHS Report, 2011 8/04/2015 9 Malnutrition • • • • Malnutrition is commonly used as an alternative to under-nutrition but also refers to over-nutrition. Malnourished: inadequate calories and protein for growth and maintenance or inability to fully utilize the food due to illness (undernutrition). Malnourished children are susceptible to increased risk of infections (diarrhea and Acute Respiratory Infection) Anthropometric indicators of nutritional status by WHO (WHO Child Growth Standards) : – Weight-for-age – Height-for-age – Weight-for-height 8/04/2015 10 Severe Acute Malnutrition • Severe acute malnutrition “wasting” is defined as very low weight for height (below -3 SD of the median WHO growth standards) Indicator Measure Severe wasting Weight-for-height < -3 SD Severe wasting Mid-upper-arm circumference (MUAC) < 110 mm 8/04/2015 Cut-off Source: WHO Children Growth Standards, 2009 11 The Prevalence of Acute Malnutrition in East Africa Region 8/04/2015 Source: Ethiopia DHS Report, 2011 12 Trends of Severe Acute Malnutrition in Ethiopia % 8/04/2015 Source: Ethiopia DHS Report, 2000, 2005, 2011 13 Conceptual Framework Causes of Malnutrition in Society 8/04/2015 Source: Unicef, 2009 14 Prevention Strategy Facility-based treatment (F-100) • Advantages: – Basic ingredients components – WHO recommendation • Disadvantages: – – – – 8/04/2015 Longer recovery time Relatively expensive Cooking required Water-based food (bacterial contamination) • Challenges: – The dearth of skilled health workers and health infrastructure – Poor accessibility (physical and economic) to these facilities – Opportunity and travel costs incurred by the mother (or caregiver) getting to staying at the health center with her child (more spending time) 15 Prevention Strategy Community-based treatment (RUTFs) • • Advantages: – Short time recovery – Relatively cheap – No cooking required – Oil-based food (less bacterial contamination) – Fewer communicable illnesses (through hospital transmission with other patients) Disadvantages: – Patent issue – Imported ingredients 8/04/2015 • Challenges: – Importing ingredients are not available locally (particularly dry skimmed milk and the mineral–vitamin mix) – Requires clinic nearby or community health workers for monitoring progress, treating illnesses, and distributing RUTF – Limited evidence on the efficacy 16 RUTF • Ready-to-Use Therapeutic Food (RUTF): homebased therapy for severe child malnutrition or severe wasting 8/04/2015 17 • RUTF is a lipid rich spread paste, contains of a mixture of ingredients Typical Recipe for RUTF 8/04/2015 18 Project Proposal RUTF DEVELOPMENT & COMMUNITY-BASED TREATMENT 8/04/2015 19 Study Design • • • • Study type: Randomized controlled trial Research questions: Is RUTF more effective and cost-effective strategy to treat severe acute malnutrition among under-five children in community-based level compared to F-100? Study hypothesis: – Null hypothesis: RUTF is as effective and cost-effective as F-100 in the treatment of severe acute malnutrition among under-five children in community-based level Study population: all under-five children aged 6-59 months suffering from severe acute malnutrition, living in East Hararghe zone in Oromiya region (the highest adjusted proportion of severe wasting) – Inclusion criteria: • Presence of severe wasting (WHO criteria: weight-for-height Z-score is less than -3 SD) • Ability of parents or guardians to provide informed consent – Exclusion criteria: • Presence of chronic diseases and not good appetite 8/04/2015 20 Objectives • To compare the effectiveness of F-100 and RUTF as the treatment of severe acute child malnutrition among under-five children in community-based level 8/04/2015 21 Sample • Sample size is calculated by the sampling method of comparing proportions for two independent samples. • From the previous study, % mortality rates for the treatment of RUTF and F-100 are 3.0% and 5.4%, respectively.1 Assuming 5% two-sided significance level and power of 80%, we get the sample size of 1,096 for each group. So, total sample for this study is 2,192 children. 1. Ciliberto MA, Sandige H, Ndekha MJ, et al. Comparison of home-based therapy with ready-to-use therapeutic food with standard therapy in the treatment of malnourished Malawian children: a controlled, clinical eff ectiveness trial. Am J Clin Nutr 2005; 81: 864–70. 8/04/2015 22 Outcomes • Primary outcomes: – Rates of growth (% children with weight-forheight Z-scores >-2 SD) • Secondary outcomes: – Mortality (% death rate) – Rates of normal weight-for-age and heightfor-age (Z-scores >-2 SD) – Cost of treatment – Length of recovery time (days) 8/04/2015 23 Intervention • Intervention: – Standard F-100 (control) – Standard RUTF • Sample is randomly assigned to each intervention (n1 = n2 = 1,096) for 8 weeks follow-up • Each children who is assessed for anthropometry and identified by the health workers as severe acute malnutrition will be allocated to the treatment 8/04/2015 24 Case Identification • Anthropometric screening for weight-for-height -3 SD (severe acute malnutrition/wasting) by the community health workers • Children are taken to the nearest village health posts to get measured on weight and height • Mothers are expected to have additional transport cost to the village health post incentives 8/04/2015 25 8/04/2015 26 8/04/2015 27 Budget Allocation No Allocation Quantity 1 F-100 supply 60 days x 1,096 children 2 RUTF supply 10 kg x 1,096 children 3 Health workers training 4 Cost Total cost $2/day $131,520 $3/kg $32,880 30 health workers x 1 day $30/person/day $900 Mothers’ training 2,192 mothers x 1 day $20/person/day $43,840 5 Transport incentives for mothers 2,192 mothers x 1 day-return $20/person/dayreturn $43,840 6 Incentives for health workers 30 health workers x 2,192 children $10/patient/day $657,600 7 Incentives for volunteers (transport) 30 volunteers x 60 days $20/person/day $36,000 8 Instruments (standardized weight and height scale) 15 $1,500 $22,500 9 Data management (data collection, analysis) 1 package $10,000 $10,000 10 Advocacy and media 1 package $5,000 $5,000 TOTAL 8/04/2015 $984,080 28 Next steps…. • Disseminate the results in policy brief paper to encourage the government and other stakeholders and persuade potential industry to locally produce RUTF • Ask for government support in providing initial budget, raw ingredients and technical assistance building advocacy 8/04/2015 29 Long-term Development 8/04/2015 30 Discussion CHALLENGES & RECOMMENDATIONS 8/04/2015 31 Limitation and Challenges • Study limitation: – Blinding is not applied – Conducted only in one area – Measurement bias • Challenges: – – – – – – 8/04/2015 Limited numbers of health workers and professionals Inadequate health facilities Low coverage of media and health information Poor transportation system due to geographical condition Limited funding Legal ramification issue in RUTF patent and license long-term development 32 Recommendations • Community-based therapeutic care scaled up in both emergency and non-emergency settings • Provide appropriate training included in medical, nursing and primary health-care curricula • RUTF widely produced and distributed to decrease barriers in access, reduce opportunity costs associated with treatment and encourage compliance by patients • Provide further study (qualitative) on the response or perception from local people, government and community leaders 8/04/2015 33 4/8/2015 34