Journal of the International Neuropsychological Society, 18(S1)
advertisement
")
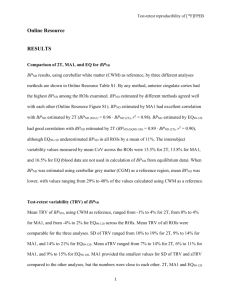
Test-retest reliability was relatively larger for PD’s Copy score (r=.68) compared to controls (r=.11). Stability coefficients for PDs and controls ranged from small to medium on immediate (r=.631, .735) and delayed trials (r=.734, .708). Coefficients were small for the unit scores (rs < .60) for both groups. Compared to the PDs, controls were more susceptible to practice effects. Test-Retest Reliability on the Rey-Osterrieth Complex Figure Test in a Sample of Parkinson’s Disease Patients Compared to Normal Controls 1 1 1 1 1 Freedland, A., Glass Umfleet, L., Schwab, N., Ward, J., Leninger, S., 1Coronado, N., 1Tanner, J., 1Nguyen, P., 2Okun, M., 1Bowers, D., 1Price, C. Supported by: Affiliations: 1Department of Clinical and Health Psychology, University of Florida; 2Department of Neurology, University of Florida K23NS60660 (CP) Objectives It is common practice for Neuropsychologists to administer the same •Rey –Osterrieth Complex Figure Test (ROCFT): tests on more than one occasion to document the progression of a •Participants were administered the ROCFT presented in landscape patient’s cognitive status. When interpreting changes, one should take version. They were required to copy the figure on a landscape white into consideration the stability of the measure as well as practice piece of paper, immediately recall the figure, and then recall the figure effects. The Rey-Osterrieth Complex Figure Test (ROCFT) is a after a 30 minutes delay. To achieve inter-rater reliability 10 figures in frequently administered test that assesses cognitive functions such as the three conditions were scored twice according to Denman criteria visuospatial organization and memory. Previous test-retest studies on (72 total points for each condition ; Denman, 1984), by two different the ROCFT have been mixed, with reliability coefficients ranging trained research assistants, to reduce examiner scoring errors from poor to adequate (Knight & Kaplan, 2003). To enhance the (r=.944). The testing intervals was one year ± 1.2 months for both generalizability of prior investigations, we examined the test-retest PD and control groups. •Test-retest reliability was relatively larger for PD’s Copy score (r=.70) compared to controls (r=.29). Stability coefficients for PDs and controls were adequate on immediate and delayed trials •Illustrated in Figure 5 are ROCFT Copy, Immediate Recall, and Delayed Recall mean raw scores at both testing periods for PDs and Controls. reliability of the ROCFT in a sample of participants with Parkinson’s •Independent samples t-tests revealed statistically significant differences disease (PD) and normal controls. between the PD and control group on all ROCFT variables at retest (ps While reliable test-retest differences were not expected, we predicted <.05). However, the controls and PDs did not differ on ROCFT means at that normal controls, compared to PD patients, will demonstrate time 1. higher scores at retest across the ROCFT Copy, Immediate Recall, and •These findings may suggest that groups were relatively comparable on Delayed Recall tasks. Participants Results Methods and Procedures Figure 1. Copy time 1 for PD Figure 2. Copy time 2 for PD initial testing, but Controls improved at 1 year thereby suggesting a practice effect. •33 non-demented PD (7 women, 26 men) and 26 non-demented controls (5 women, 21 men). Means for age and education are 67.06 (SD = 5.58) and 16.09 (SD = 2.99) for PD, and 67.69 (SD = 4.64) and 16.58 (SD = 2.60) for Controls. Conclusions/Implications •Participants were matched by age and education • Exclusion criteria: having another medical disease likely to limit Figure 3. Copy time 1 for control Figure 4. Copy time 2 for control year (Bartels, Wegrzyn, Wiedl, Ackerman, & Ehrenreich, 2010). lifespan or confound outcome analysis •PD patients could not have undergone Deep Brain Stimulation and could not have evidence of secondary or atypical Parkinsonism as suggested by the presence of any of the following: 1) history of major stroke(s), 2) exposure to toxins or neuroleptics, 3) history of encephalitis, 4) neurological signs of upper motor neuron disease, cerebellar involvement, supranuclear palsy, or significant orthostatic hypertension. •Our findings were similar to previous studies with testing intervals ≥ 1 Cognitive/ Neuropsychological Tests Administered: •Clinicians should cautiously proceed with interpreting changes on the •In addition to the ROCFT, participants were administered the Wechsler ROCFT over one year test-retest intervals, especially when examining Test of Adult Reading (Wechsler, 2001), the Dementia Rating Scale-2 less impaired subjects. (Jurica, Leitten, & Mattis, 2001), and the Wechsler Test of Adult Reading reliable change metric appears appropriate. Wechsler, 2001) to screen for dementia and match for estimated •Using the ROCFT for individuals with Parkinson’s disease appears premorbid intelligence. No significant differences emerged between PDs reasonable, but clinicians are encouraged to consider symptom variability and Controls on the WTAR, DRS-2, and WTAR scores (ps >.05). between patients. For non-disease individuals (e.g., controls) a