Managed Care contracting: opportunities and risks.
advertisement

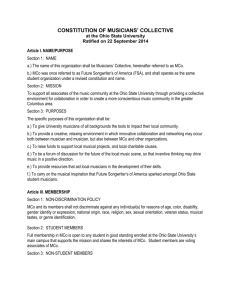
Are You Ready for Managed Care? Bearing and Contracting for Risk in New York’s Managed Care Environment Stephen A. Warnke, Esq. Ropes & Gray LLP ROPES & GRAY LLP Agenda • Legislative and Regulatory Context for the Transition to Managed Care • Impact of Managed Care on Providers of Services to the Intellectually and Developmentally Disabled • What It Means to Bear “Risk” • Types of Risk Sharing Arrangements – Independent Practice Associations (IPAs) – Care Management • Pitfalls to Avoid in Provider Contracting 3 ROPES & GRAY Legislative and Regulatory Context • New York’s application for a Medicaid “Section 1115” waiver to enroll developmentally disabled (DD) individuals in managed care is poised for final federal approval • Under 2013-2014 budget legislation passed in March, Medicaid DD recipients will receive a comprehensive benefit package, including habilitation services and health and long-term health care services, through one of the following Article 44 managed care organization (MCO) vehicles: • – A Developmental Disabilities Individual Support and Care Coordination Organization (DISCO) – A commercial HMO that expands its service offerings and commercial benefit package to the DD population – A specialized Medicaid Long-Term Care Plan (MLTCP) capable of furnishing services to the DD population (three of which are eligible to participate in the Fully Integrated Duals Advantage demonstration program) Rules are still inchoate; we await: – “Special Terms and Conditions” of CMS’s Section 1115 approval – Issuance of a revised Request for Applications by OPWDD for DISCOs – Other application forms and regulatory guidance 4 ROPES & GRAY Impact on DD Providers • Under the Cuomo Administration’s philosophy of “Care Management for All,” a phase-out of fee-for-service payment for DD services • DD providers will need to contract with multiple DD-authorized MCOs in order to maintain their existing revenue streams • Participating provider agreements, not OPWDD Medicaid payment regulations, will determine: – Rates of payment – Claims submission windows – Remedies for late or denied payment – Credentialing standards – Audit and documentation requirements • Potential upside if a provider is able to assume and manage risk (i.e., the assumption of financial responsibility for the cost and utilization of services) 5 ROPES & GRAY Risk Transfer • Risk may be borne at both the MCO and downstream provider levels • By statute and contract, an MCO accepts responsibility for payment of claims out of a capitation budget – MCO realizes surplus if the cost of claims and administrative expenses is less than aggregate premiums – MCO realizes loss if the opposite equation prevails • Under New York law, an MCO may also share financial responsibility with its contracted providers under an approved risktransfer arrangement • Risk transfer is highly regulated, and never absolute: an MCO may share, but not divest itself of, financial responsibility • The level of regulation and capital reserve requirements depends on the amount of risk transferred by the MCO to the provider 6 ROPES & GRAY DFS/DOH Jurisdiction Over Risk • Both the Department of Financial Services (DFS) and Department of Health (DOH) have jurisdiction over risk-transfer arrangements involving the cost of care delivered to MCO enrollees • DOH guidance requires advance review and approval of an MCO’s template agreements with downstream providers, including any “material amendments” to such template agreements – “Material amendments” include any change in compensation terms, thus capturing all risk transfer arrangements • Regulatory impetus is two-fold – Ensure adequate reserves against adverse claims experience – Prevent undue incentives for “skimping” or withholding of care 7 ROPES & GRAY Levels of Risk Sharing DOH requires different types of provider arrangements to meet financial viability and financial security deposit requirements depending on the level of risk shared by the provider • Fee-for-Service: Payment for services on a fee-for-service basis pursuant to a pre-defined fee schedule – No requirement to demonstrate financial viability or to maintain a financial security deposit • Level 1: Fee-for-service arrangements with withholds or bonuses up to 25% of the payment for health care services – No requirement to demonstrate financial viability or to maintain a financial security deposit • Level 2: Capitated risk transfers to a provider for a single specific service that the provider directly provides – No requirement to demonstrate financial viability or to maintain a financial security deposit 8 ROPES & GRAY Levels of Risk Sharing (cont.) • Level 3: Broader risk transfer to a provider (e.g., capitated arrangement for multiple services provided directly or fee-forservice arrangements with withholds or bonuses of greater than 25% of the payment for health care services) – Such contracts must demonstrate the provider’s financial viability – If the provider’s net worth is less than or equal to zero, a security deposit must be established for the provider’s in-network costs • Level 4: Contracts that transfer risk to IPAs for single or multiple services – Such contracts must demonstrate the IPA’s financial viability and establish a security deposit 9 ROPES & GRAY Medical Loss Ratio Requirements • Regardless of the amount of risk transferred to a provider, MCOs receiving New York state funding will be held to increasing medical loss ratio (MLR) requirements • MLR requirements limit the percentage of state funds received by an MCO that may be spent on services other than health care services (e.g., a MLR of 75/25 requires that 75% of state funds received by an MCO be spent on health care services, leaving 25% to support administrative costs) • Governor Cuomo has mandated a phase-in of MLR requirements such that, by April 1, 2015 and thereafter, MCOs will be held to an 85/15 MLR 10 ROPES & GRAY IPA Structure and Formation • An IPA is a special-purpose MCO contracting vehicle under Part 98 of DOH regulations • Serves as an intermediary between an MCO and all or a portion of the MCO’s downstream providers, subcontracting with providers to arrange for the delivery of care to MCO enrollees • Authorized to arrange for services of multiple providers, whether on a fee-for-service or risk sharing basis, without violating New York corporate practice of medicine prohibitions 11 ROPES & GRAY IPA Reserve Requirements • If at risk, an IPA must carry a separate, IPA-level reserve – Equal to 12.5% of the payments received from the MCO – Must be held in a special account, subject to the approval of DOH • Unlike with reinsurance contracts, IPA reserves are not a basis for reducing the MCO’s reserve requirements • End Result: Downstream risk-based payments to an IPA require reserves to be met by both the MCO and IPA 12 ROPES & GRAY IPAs: Pros and Cons Pros Cons • Relatively easy to form • • Allows separately organized (otherwise competitive) DD providers to come together for purposes of single-signature contracting with MCOs Joint contracting must be ancillary to integrative efficiencies • Basing joint contracting on clinical integration can be time consuming and expensive • Separate, non-waivable IPA reserve requirements • If IPA engages in utilization review, it must: • • Allows DD providers to accept risk (upside/downside) and realize benefits of care coordination without the burdens of MCO licensure and operations Vehicle through which to perform key MCO delegated functions (e.g., credentialing, quality assurance) 13 – Do so through a separate DOH-approved management contract, and – Be licensed as a utilization review agent ROPES & GRAY Care Management as an Alternative • As an alternative to forming an IPA with other DD providers, a DD provider may contract to provide care management administrative services (CMAS) for MCOs • Through a CMAS arrangement, a DD provider can realize the benefits of care coordination without many of the burdens associated with being part of an IPA • DOH requirements for CMAS contracts are less onerous – Traditional “management functions” such as quality assurance must be addressed in a separate management services agreement that satisfies applicable DOH guidance – The CMAS-contracting entity must be a licensed health care provider or other entity approved by DOH • Stand-alone care management contracts may have a short shelf live as delegated care coordination functions transition to health homes, as they have for certain non-DD populations 14 ROPES & GRAY Managed Care Provider Contracts: Potential Pitfalls • Understanding key terms and issues for a DD provider contracting with an MCO: – Definition of “clean claim” – Submission windows and pre-authorization – Prompt payment requirements – Definition of “medical necessity” – Appeal and grievance processes – Recoupment rights – Unilateral amendment based on MCO’s government contract – Unilateral amendment based on changes in MCO’s Provider Manual – Understand the MCO’s Utilization Review and Quality Assurance processes • Understanding bargaining power and limited room for negotiation (many requirements are mandated by DOH) • Thinking carefully about how provisions will be operationalized 15 ROPES & GRAY Thank You Stephen A. Warnke Ropes & Gray LLP stephen.warnke@ropesgray.com 212-841-0681 16 ROPES & GRAY