NY Times March 2, 2007 Most Support U.S.
advertisement

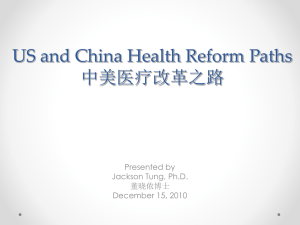
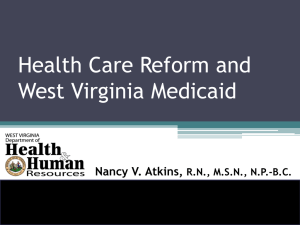
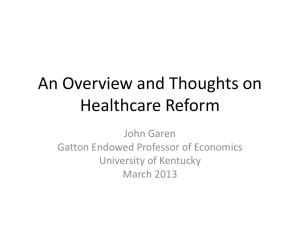
U.S. Health Care System: History, status, current reform James G. Kahn, MD, MPH 28 April 2012 Overview 1. History 2. Current system 3. Profile Performance vs OECD Federal reform – the ACA Major US Health Reform Efforts and Events & Medicaid Medical benefits to increase compensation during WWII salary freeze Other Forces Affecting US Health Care Weak cost controls • RBRVS (a scale for outpatient care) • DRGs (inpatient per diagnosis) Rise of technology and specialty care Rise of corporate form for insurers & providers 80 007 70 006 60 005 50 004 40 003 30 002 20 1997 001 10 0 Enrollment Source: InterStudy National HMO Census. Plans 19 96 19 94 19 92 19 90 19 88 19 86 19 84 19 82 19 80 19 78 19 76 19 74 19 72 19 70 0 Number of Plans Enrollment (in millions) CORPORATE MEDICINE IS HERE TO STAY (and has been for a long time) Growth in HMO Enrollment and Plans, 1970-1997 Key features of US Health Care Financing 17.4% of GDP 2009 and rising, $2.5 T, 8,086 per capita Public – 43% (27% federal, 16% state/local) • CMS (Center for Medicare and Medicaid Services) Medicare – federal, aged & disabled ($502 B) Medicaid – state/federal, poor & long term care ($374 B) • Veteran’s Admin, Military, Indian Health Svc, … • State and local safety net Private – 34% • Employers – 21% • Families – premium contribution – 13% Families – uninsured services & copays etc – 15% Other private – 7% Martin, Health Affairs 2011 U.S. vs Other OECD countries Spending per capita ~50% higher Generally fewer doctor visits and hospital days Difference in spending due to: • price (costs of doctor, procedure, drugs) • use of high technology • administrative costs (later) Health care outcomes same or worse Number of Uninsured in the US Source: US Census Bureau, Current Population Surveys 50 Millions of people 45 15.8% of population 40 35 30 25 2006 2000 1990 1985 1980 1976 20 Schoen 2005 US standing on health care outcomes Rank of 13 industrialized nations Low birth weight % (U.S. in Red) Infant mortality Years of potential life lost Age adjusted mortality Life expectancy @ 1 yr Life expectancy @ 40 yrs Life expectancy @ 65 yrs Life expectancy @ 80 yrs Average for all indicators Poorest Best Billing and Insurance-Related Administrative Costs U.S. Health Care Financing Multi-payer health care financing Funds Payers Providers Public & Private Employer Premium contrib. Many "pools" Multiple private payers & many benefit plans Income taxes PPO vs capitated, many blends/variants Public: Medicare, Medi-Cal, Out-of-pocket S-CHiP, VA, Indian Health,. ~ 60 safety net programs Doctors Hospitals Pharmacies Device vendors Skilled Nursing Fac. Other Admin costs of insurance 15% Admin costs overall 30% $400 billion annually in billing and insurance-related (BIR) administration = $1300 per person per year ~60% is at providers >$250 billion is “excess” - avoidable Elements of Provider BIR - 1 Complexity of the insurance process: multiple steps, often detailed & demanding: Contracting, maintaining benefits database, patient insurance determination, collection of copayments, formulary and prior authorization procedures, procedure coding, submitting claims, receiving payments, paying subcontracted providers, appealing denials and underpayments, negotiating endof-year resolution of unsettled claims, and collecting from patients, … Elements of Provider BIR - 2 Friction: some BIR steps are (or seem) designed to slow and complicate the process, e.g., prior authorization, high rates of denials / errors / underpayment. Variation: modest number of payers, but dozens to hundreds of plans, including negotiated variants. Providers need to track plan-specific benefits and pay rules. Allocation of spending for hospital and physician care paid through private insurers Insurer cMLR 19.0% Medical care 62.0% Hospital BIR 3.9% Physician BIR 5% Medical care admin 10.1% Reform Incremental … Systemic Major types of health reform Free market – let individuals buy health insurance / care, subsidize the poor. Often called “consumer driven”. Based on principles of moral hazard. Improved mixed system – regulate private insurance, expand public insurance (PPACA). “Managed competition” Single payer / universal – use a public fund to pay for private and public providers, everyone covered with good benefit package. Common in OECD countries. By What Criteria Should We Judge Reform Proposals? The IOM Report: 2004: Health care coverage should be universal. Health care coverage should be continuous. Health care coverage should be affordable to individuals and families. The health insurance strategy should be affordable and sustainable for society. Health insurance should enhance health and well-being by promoting access to high-quality care that is effective, efficient, safe, timely, patient-centered, and equitable. Patient Protection and Affordable Care Act - PPACA (March 2010) Key provisions Private insurance regulation - fairer, less baroque Insurance exchanges - individuals / small business Public means-tested – expand (Medicaid, CHIP) Medicare - close gaps, control costs Individual mandate Subsidies for poor / near-poor Patient Protection and Affordable Care Act (PPACA) Prospective report card on Obama health care reform Much Worse worse No Δ Better Solved x Coverage 92-94% covered? (vs 85% now) Pre-existing illness exclusion x Eliminated (they say) Chronic disease premium cost x Eliminated - "community rating" Recission (revoking policy) x Disallowed, and shielded by above changes. Primary care strengthening x Various initiatives Quality of care x "Accountable care" & "comparative effectiveness" Medical malpractice x Special court? Comprehensive benefits ? To keep premiums low, fewer benefits. Unless … meaningful benefits minimum standard. Financial burden to individuals ? New policies: high cost-sharing to save feds money. But annual caps on out-of-pocket. Administrative burden / costs Insurer profits More private for-profit insurance; persistent product profusion; added admin (eg mandate). x x x Federal govt costs System costs More private for-profit insurance. x More subsidies vs. reasonable Medicare cost control ("accountable care"). More insured with missed opportunity for large savings (eg less administration). PPACA waivers Used to further coddle insurers, edentulating the bill. Dozens granted, e.g., Child coverage: Insurers complained may have to exit market if forced to cover sick children on parents’ policies. The govt allowed brief open-enrollment periods and higher premiums. Insurers free to set their own premium rates, with limited states restraint. Medical loss ratios (MLRs) set at 80-85%. Concessions: counting expenses of quality assurance as medical costs, deduct taxes from premiums before calculating MLR, and the ability to appeal for lower MLR for up to 3 years in states where “there is a reasonable likelihood that market destabilization could harm consumers”. Four states so far. Exempted plans: Many insurance plans, including most large employers, exempt from PPACA - “grandfathered in” > 100 employers and other insurers can retain very low annual limits of coverage (eg. only $2,000 a year, hardly qualifying as insurance). E.g., McDonald’s, after warning regulators that it might have to drop coverage for 30,000 hourly workers, can keep “mini-med” policies. John Geyman, PNHP blog, Dec 2010