Hot Topics Impacting Payments
advertisement

Hot Topics Impacting
Hospital Payments
2014 Revenue Cycle Fall Workshop
WV HFMA
Hot Topics
–
–
–
–
–
–
–
–
–
–
–
Outpatient facility coding
Provider Based Changes
Critical Care
Emergency Department
Outpatient E&M Services
Medical Necessity
Midlevels
Modifiers
OP Clinical Diagnostic Lab Tests
Two Midnight Rule & Case Studies
ICD-10 Readiness
2
Hot Topics
3
Medicare Claims
Medicare receives over 1.2 billion claims
per year. This equates to:
4.6 million claims per work day, or
575,000 claims per hour
9,580 claims per minute
160 claims per second
4
Outpatient Visit Coding (Facility)
• OPPS rules continue to contain the information on
adopting an internal policy that is indicative of the
resources utilized by the hospital. No mention of the
fact that payment is the same so frequency and
distribution is irrelevant due to same payment.
• Best if chargemaster contains the CPT codes 9920199215 with a different charge at each level in order to
maintain compliance with consistent charging to all
payers.
• Most clients are choosing to flip the E&M code to the
required G code within the system.
• G code is G0463.
• No changes per the 2015 OPPS proposed rule
except as it relates to provider based locations
placing a modifier.
5
Provider Based Rule Change
•
•
•
•
•
Buried in the proposed rule is a small item addressing off-campus
provider-based departments.
CMS notes the increase in hospital acquisitions of physician practices
and the increase in the delivery of physicians’ services in a hospital
setting as the reasons for taking another look at the regulations.
Specifically, CMS is proposing to collect this information beginning
January 1, 2015, by requiring the use of a new HCPCS modifier that
would be reported with every code for physician and outpatient hospital
services furnished in an off-campus provider-based department of a
hospital.
The modifier would be reported on both the CMS-1500 claim form for
physician services and the UB-04 form (CMS Form 1450) for hospital
outpatient services.
CMS is asking for additional public comment on whether the use of a
modifier is the best mechanism for collecting this service-level data.
6
Emergency Department
Critical Care
• Beginning in 2007, nurses must also document duration
of critical care time in order to charge E/M 99291. (Less
than 30 minutes of care does not support critical care)
• 99292: Code used for each 30 minutes beyond the 1st
hour.
• Remember – if it is not documented, it did not happen.
7
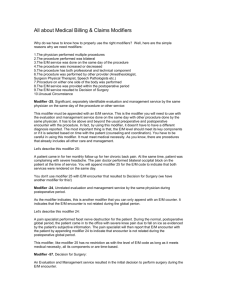
Emergency Department
Distribution of Technical Component (Facility) ED Codes
2012
2014
8
Emergency Department
ED Treatment Rooms
• Do not bill E/M with drug administration charge when an
infusion is the sole reason for the visit
• 2007 OPPS Final Rule – “Providers should bill a lowlevel visit code in such circumstances only if the hospital
provides a significant, separately identifiable low level
visit in association with the packaged service.”
9
Medical Necessity
• Medically Necessary means that a service, supply or
medicine is necessary and appropriate and meets the
standards of good medical practice in the medical
community for the diagnosis or treatment of a covered
illness or injury, as determined by the insurance
company
• Review National Coverage Decisions (NCD)
• Review Local Medical Review Policies (LMRP)
• NCDs take precedence over LMRPs
10
Use of Mid-levels in Provider Based
Clinics & Emergency Departments
• Prior to Provider Based Implementation
– Incident – to under 42 CFR Section 410.26 (physician
office rule)
• After Implementation
– Incident – to – different rule 42 CFR Section 410.27
• Midlevels in ED – Medicare requires bill under name of
Midlevel unless “shared visit requirements are met”
11
Modifiers
Modifier -25
• Significant, separately identifiable evaluation and
management service by the same physician on the
same day of the procedure or other service
• Use on E/M codes only
• Ask yourself “is the patient presenting with a chief
complaint requiring evaluation to determine treatment?”
12
Modifiers
Modifier -59
• Procedure or service was distinct or independent from
other services performed on the same day.
• Indicates that the procedure is not considered to be a
component of another procedure, but instead is a distinct
independent procedure.
• Guidance from CMS can be found at:
http://www.cms.hhs.gov/NationalCorrectCodInitEd/Downloads/modifier59.pdf
13
Modifier -59 Cont.
Effective January 5, 2015 the new "more specific"
modifiers (in place of modifier -59), include:
• XE Separate Encounter: A Service That Is Distinct
Because It Occurred During A Separate Encounter
• XS Separate Structure: A Service That Is Distinct
Because It Was Performed On A Separate
Organ/Structure
• XP Separate Practitioner: A Service That Is Distinct
Because It Was Performed By A Different Practitioner
• XU Unusual Non-Overlapping Service: The Use Of
A Service That Is Distinct Because It Does Not
Overlap Usual Components Of The Main Service.
14
Modifier -59 Cont.
Per CMS instructions page 3
“As a default, at this time CMS will initially accept either a 59 modifier OR a more selective - X{EPSU} modifier as
correct coding, although the rapid migration of providers to
the more selective modifiers is encouraged."
However, please note that these modifiers are valid even
before national edits are in place. MACs are not prohibited
from requiring the use of selective modifiers in lieu of the
general -59 modifier, when necessitated by local program
integrity and compliance needs.”
15
Modifier -59 Cont.
Question:
We have a new cardiologist who orders an EKG before and
after all his heart catheterization procedures and stress
tests. He insists that we should be adding modifier -59
(distinct procedural service) to each of these because they
are not done as part of the procedure. Our compliance
office disagrees. Is it appropriate to add modifier -59 in this
scenario?
16
Modifier -59 Cont.
Answer:
• Is there a more appropriate modifier that can be appended to
explain the situation
– the answer would be no, as none of the anatomical modifiers or
other modifiers—such as those for a repeat procedure—are
applicable
• When a physician orders a cardiac procedure, typically there has
been consideration or indications that there is a cardiac situation
that needs to be evaluated
– when the physician orders the EKG as part of the order set for the procedure, the
EKGs are part of the procedure
– No sign/symptom of a problem supports the medical necessity of reporting the
procedure
• The EKG can be done, but should be reported as part of the
cardiac procedure
17
Modifier -59 Cont.
In the example when would the -59 apply?
• The patient has signs/symptoms of some issue
occurring, such as chest pain after the cardiac procedure
is over and wants to leave the facility
– In that situation the test has a diagnostic purpose
– The physician needs to know what the patient’s
cardiac rhythm is to see what needs to be done to
treat the chest pain
– The EKG was performed for a reason separate and
distinct from the reason/rationale for the cardiac
procedure, and reporting the EKG with modifier -59
would be appropriate
18
OP Clinical Diagnostic Lab Tests
• Over the past 15 years, CMS has refined its
understanding of and commitment to OPPS as a
prospective payment system and not as fee-schedule
driven, with separate payment made for each coded line
item
• Beginning 1/1/14 CMS finalized one of the most
aggressive packaging policies under OPPS history
• The rule packaged the payment of outpatient lab tests
(other than molecular pathology) under the OPPS rather
than separate CLFS payment, effective for dates of
service beginning on 1/1/14.
19
OP Clinical Diagnostic Lab Tests
• Later in 2014, CMS published further instructions
regarding when laboratory tests are paid separately and
ultimately packaged in Transmittal 2971 and MLN
Matters SE1412. (Implementation date = 1/6/14)
• Packaged payment applies to all lab tests (other than
molecular pathology) billed by OPPS hospitals on a
013X Type of Bill (TOB) (Hospital Outpatient).
20
OP Clinical Diagnostic Lab Tests
• CMS created very limited exceptions to the packaging
policy and instructed hospitals to use the 014X TOB
(Hospital Non-Patient) to obtain separate payment only
in the following circumstances
– Non-patient (referred) specimen
– A hospital collects specimen and furnishes only the outpatient
labs on a given date of service or
– A hospital conducts outpatient lab tests that are clinically
unrelated to other hospital outpatient services furnished the
same day.
– “Unrelated” means
•
the laboratory test is ordered by a different practitioner than the practitioner
who ordered the other hospital outpatient services, for a different diagnosis.
21
OP Clinical Diagnostic Lab Tests
• Beginning with dates of service on or after July 1, 2014, CMS
requires appending modifier -L1 to assist with revenue cycle
operations and securing separate payment from CMS when stated
provisions are met. The Type of bill remains 013X rather than 014X
• This modifier on the claim indicates that one of the exceptions
previously stated are met
– CMS will be reviewing claims data for CY 2014 for potential
inappropriate unbundling of laboratory services under the new
OPPS packaging policy.
– As stated in the OPPS final rule, CMS does not expect changes
in practice patterns under the new policy.
– Hospitals may not establish new scheduling patterns in order to
provide laboratory services on separate dates of service from
other hospital services for the purpose of receiving separate
payment under the CLFS
22
Two Midnight Benchmark
The Two Midnight Benchmark describes the physician’s expectation at the
time of admission and how CMS will review claims under the Two Midnight rule
– Contractors will include the time the beneficiary spends receiving
outpatient care in their review decision (includes outpatient care in a
hospital-based outpatient department whether on campus or off campus)
– If total time the beneficiary is expected to spend receiving medically
necessary hospital care (includes both outpatient care and inpatient care)
equals-• 0-1 Midnight: Review contractor will review claim to see if the
beneficiary was admitted for an inpatient-only procedure or if other
circumstances justify inpatient admission per CMS guidance (e.g.,
new onset ventilation) (Note: admission to ICU does not by itself justify
an inpatient admission). Otherwise, Part A payment will be denied.
• 2 or More Midnights: Review contractor will generally find Part A
payment to be appropriate.
23
The Presumption Selection of Claims
for Medical Review
How will claims be selected for review under the two midnight rule
• If a claim shows two or more midnights after the time of formal
inpatient admission —
– The contractor will presume for claim selection purposes that
inpatient admission is appropriate
– This claim will not be the focus of medical review
• Exception: Medicare contractor will monitor claim patterns for
evidence of systematic gaming or abuse, such as
unnecessary delays in the provision of care to surpass two
inpatient midnights
– Statistical drops in the number of 0-1 Day Stays; spikes in
the number of 2 Day Stays after 10/1/2013.
.
24
Two Midnight Rule
CASE SCENARIOS
25
CASE SCENARIO 1
A 68-year-old male presents at the ED with several days’ history of urinary symptoms,
vague intermittent abdominal discomfort, he had gassy and feverish feeling over the past
several days, and intermittent chills and nausea without vomiting. This patient is on oral
meds for constipation, hypertension, cholesterol, and diabetes. The patient complains that
he is just not feeling like himself, he has no appetite, he’s tired, and may have a touch of
the flu. No other complaints are noted.
This patient presents on October 1st at 10:00 p.m. and is triaged. At 10:10 p.m., a urine
sample and glucometer reading are obtained, and the patient is sent back to the waiting
room. At 11:00 p.m., the physician assesses the patient and orders therapeutic and
additional diagnostic modalities. At 12:00 a.m., the patient has a new complaint of chest
pain. Additional tests and treatments are provided.
On October 2nd at 12:15 a.m., the physician reevaluates the patient after the new
complaint and determines that he will need to stay in the hospital for at least two
midnights of medically necessary hospital services. At 12:35 a.m., a formal order and
inpatient admission are provided. The patient stays overnight, and on October
3rd at 7:35 a.m., the patient is safe for discharge home.
26
CASE SCENARIO 2
An 80-year-old female presents to her primary care physician’s office
not feeling well. She has a past medical history significant for chronic
obstructive pulmonary disease and is on multiple medications. She has
been experiencing increased shortness of breath for the last several
days. On October 1st at 6:00 p.m., she’s evaluated by her primary care
physician and sent to the hospital for further evaluation. She’s sent via
ambulance.
At 9:00 p.m., upon arrival at the hospital, the admitting practitioner
confirms the suspected diagnosis and admits the woman based on his
expectation that the patient’s care will span at least two midnights. The
patient continues to receive medically necessary hospital services from
October 2nd through October 4th. On October 5th at 9:00 a.m., the
patient is discharged home.
27
ICD-10 Expected Impacts
28
ICD-10 Readiness
•
•
•
•
•
•
•
•
•
•
•
•
Check vendor preparedness now
Create a dashboard to track documentation opportunities
Begin claims testing with external vendors
Start dual coding
Educate physicians and create training scenarios
Identify skill gaps
Review the dual coding differences to begin to calculate ICD-10
reimbursement impact
Adjust budgets and projections for impacts
Prepare for productivity declines by staffing up or contracting with an
agency
Establish contingency plans for high risk areas
Train front end staff on new medical necessity guidelines
Plan for real-time coordinator to field questions during transition
29
CONTACT INFORMATION
Jill Griffith
Jill.Griffith@aftcpas.com
Toll Free: 1-800-642-3601
30