Xpert MTB-RIF Algorithms
advertisement

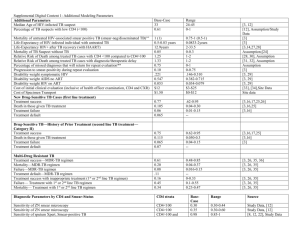
Xpert in the diagnostic algorithm of pulmonary TB in adult patients who are neither high risk for HIV, nor high risk for MDR-TB Preparations for the global consultation DEWG core team meeting, Berlin 10 Nov 2010 Jacob Creswell, Knut Lönnroth, Ikushi Onozaki, Salah Ottmani, Suvanand Sahu, Mukund Uplekar Group work in the consultation • Operationalize STAG recommendations – develop implementation road map: 1. 2. 3. HIV (high HIV prevalence settings / people suspected of HIV) MDR-TB (high MDR-TB prevalence settings / MDR risk groups) DOTS expansion and enhancement (settings and individuals where HIV and MDR-TB are of lesser concern). • Three topics for discussion 1. 2. 3. Proposed algorithm(s) Implementation issues Operational research • Preparations for group 3: 1. 2. 3. Small ad hoc group in Secretariat have done preliminary work Discussion in DEWG core team 10 Nov Mini task force to finalise draft for the consultation STAG-TB supports Expert Group guidance that: 1. Xpert MTB/RIF should be used as the initial diagnostic test in individuals suspected of MDR-TB or HIV-associated TB (strong recommendation); 2. Xpert MTB/RIF may be used as a follow-on test to microscopy in settings where MDR and/or HIV is of lesser concern, especially in smear-negative specimens (conditional recommendation, recognising major resource implications). Group 3 algorithms - assumptions 1. The issue is not only to find the appropriate place of Xpert in the current algorithm, but also to re-consider the whole algorithm, including potentially changed role of microscopy and X-ray for screening, diagnosis and case categorization. 2. The priority is algorithms for "passive" case finding. Additional algorithms may have to be developed for "active" case findings in TB risk groups other than people with HIV. 3. The algorithms need to be linked to / integrated with / consistent with algorithms for people at high risk of MDR-TB and people with HIV, which have not yet been finalized. 4. The recommendation to use Xpert "as the initial diagnostic test" for people at high risk of HIV or MDR-TB, does not necessarily mean first screening test 5. Different algorithms are required for at least two different levels of the health system: a. Facilities with smear microscopy but no X-ray b. Facilities with X-ray 6. The algorithms should work in both high and low MDR prevalance / HIV prevalance settings 7. The first step is to identify the most effective and costeffective approach. Affordability and feasibility issues are considered under implementation challenges. • Not HIV clinic Legend/Guide • Not TB cases failing treatment Start • Not contact investigation • Not active case findings Process/Action TB SUSPECT Is HIV+? Option 1: Diagnostic algorithm for passive case finding in a facility with microscopy and no CXR HIV- or Unknown Result Microscopy HIV+ Decision Follow HIV Algorithm Referral for CXR SS- Endpoint Result CXR Abnormal SS+ CXR Normal YES XPERT TB+ No Res MDR Risk Factors? Result NO No TB TB+ Rif Res Further FLD SLD Clinical Management FLD Legend/Guide TB SUSPECT Start Process/Action Option 2a: Diagnostic algorithm for passive case finding in facilities with CXR CXR Result CXR Abnormal Decision CXR Normal XPERT Endpoint Result **Note - Use of culture and DST will be necessary in parallel with GeneXpert use TB+ No Res No TB TB+ Rif Res Further FLD SLD Clinical Management Legend/Guide TB SUSPECT Start Process/Action Option 2b: Diagnostic algorithm for passive case finding in facilities with CXR CXR Result CXR Abnormal Decision XPERT Endpoint ss- Smear? ? ss+ Result **Note - Use of culture and DST will be necessary in parallel with GeneXpert use TB+ No Res No TB TB+ Rif Res Further FLD SLD Clinical Management CXR Normal Absolute Increases in bacteriologically identified Case Detection Asuming 12% C+ in Population of 10,000 TB Suspects 1400 1276 1200 1104 1250 1146 1093 1164 1121 1070 1058 1055 1000 800 720 720 Absolute TB Cases TB Cases Absolute True Positives 600 400 200 0 Standard Xpert CXR, Xpert CXR, Smear Xpert Algorithm SS Xpert SS CXR Xpert 90% 80% Percentage Increase in bacteriologically identified Case Detection from Current Algorithm % increase in CD compared to standard 77% % increase in true CD 74% 70% 62% 59% 60% 53% 56% 52% 49% 50% 50% 47% % 40% 30% 20% 10% 0% Xpert CXR, Xpert CXR, Smear Xpert Algorithm SS Xpert SS CXR Xpert Costs per Case of TB Diagnosis Equipment cost only for Xpert! 180 200 $/case (tests) 173 $/case with digital CXR (tests) 160 163 144 133 140 120 114 120 USD 100 80 60 74 68 56 40 20 0 Standard Screening Xpert CXR, Xpert CXR, Smear Xpert Algorithm SS Xpert SS CXR Xpert Algorithm- Issues to discuss during consultation • Detailed technical discussion on proposed algorithms • Can we use the same algorithm in both low- and high MDR-TB / HIV settings? • How to link with algorithms for people at risk of HIV and MDR-TB? • Can we use the same algorithm in high and low TB prevalance settings? • Do we need to change the definition of a TB case and method for monitoring treatment outcomes (if sputum smear microscopy is no longer essential for diagnosis)? Implementation • Considerations for NTPs, partners, and donors: – Should we develop an interim algorithm for settings that are already planning to purchase Xpert, or discourage general use until results from further research findings? – If interim algorithm, should we prepare an operational research protocol that should be used in all sites? – Where is the appropriate place of Xpert in the health system? – What are the capacity strengthening needs for Xpert, X-ray, R&R, etc? – What are the health systems pros and cons of different algorithms (e.g. improving X-ray capacity is beneficial for diagnosis of many other conditions) Strategy for Xpert use in the private sector – Should private providers engaged in PPM schemes have access to Xpert at reduced cost? – Should the be an agreement with Sepheid to only sell Xpert to private providers on condition of report to NTP where Xpert has been purchased as well as mandatory reporting/notification of diagnosed cases? – Accreditation / certification? – Need to update ISTC? – Should NTPs accept cases diagnosed with Xpert in the private sector (need to change case definition)? Research needs • What recommendations for the evaluation of Xpert in the FIND sites, concerning cases that are neither HIV-positive, nor high risk for MDR? – Use sputum smear microscopy, Xpert, X-ray, and culture for all suspects in order to fully assess sensitivity and specificity of all permutations? – Full assessment of risk factor profile for MDR and TB (HIV, smoking, diabetes, etc) among all suspects in order to assess differences in yield and precision across risk groups • Operational research questions and protocol; which operational question?