WHY GILMORE`S GROIN IS NOT A HERNIA
advertisement

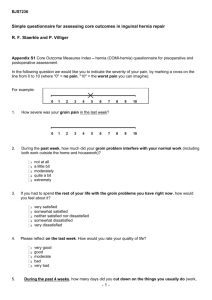
WHY GILMORE’S GROIN IS NOT A HERNIA 16.06.2011 GILMORE’S GROIN SPORTSMEN GROIN GROIN DISRUPTION ATHLETIC PUBALGIA (Sportsmen hernia NO!) CASE 1 D.M. 27 FULL BACK: TOTTENHAM HOTSPUR FC PRESENTED: 28.08.80 SYMPTOMS: 17 WEEKS GROIN PAIN AFTER EVERSION INJURY LAST GAME: 17 WEEKS PAIN INCREASED: SPRINTING KICKING TWISTING & TURNING COUGHING SNEEZING CASE 1 D.M. PREVIOUS INVESTIGATIONS: 3 ORTHOPAEDIC OPINIONS X-RAY CT SCAN U/S SCAN PREVIOUS TREATMENT: COMPLETE REST PHYSIOTHERAPY MANIPULATION LOCAL STEROIDS CASE 1 D.M. PHYSICAL SIGNS INSPECTION: N.A.D. –NO SWELLING PALPATION: N.A.D. – NO LUMP PALPATION VIA SCROTUM: RIGHT SUPERFICIAL INGUINAL RING DILATED - COUGH IMPULSE - TENDER INSERTION OF FINGER PAIN COMPARED TO OPPOSITE SIDE Presented 16.03.81 (Eversion / Overstretching Injury) 15 wks Groin Pain but No Lump Prevented Training /Play Post Op: Training with Aberdeen In Scotland Squad 3 wks 7 wks GROIN DISRUPTION TYPICAL PATIENT • YOUNG MALE • ACTIVE SPORTSMEN • RARE OVER 45 • RARE IN FEMALES (1%) GROIN DISRUPTION • MUSCULO – TENDINOUS INJURY • ALL LAYERS GROIN • INGUINAL + (ADDUCTOR 40%) • “MUSCLE DISLOCATION” ONSET OF SYMPTOMS INSIDIOUS 72% SPECIFIC INJURY 28% OVERSTRETCHING MISKICKING ABDUCTION EVERSION PATIENT’S REFERRED with GROIN PAIN 1980 - 2010 TOTAL 7738 MALE 7479 (97%) 259 (3%) FEMALE INCIDENCE OF OPERATION 1980 - 2010 Referred Ops 58% 7738 pts 4466 pts 1980-2010 Over 31 years 7479 Sporsmen referred with “Groin Pain” Many have returned with other complaints including Haemorrhoids and skin lesions But ONLY 1 with HERNIA C INTERNATIONALS 1980-2010 SOCCER 257 RUGBY UNION 44 ATHLETES 24 CRICKET 22 RUGBY LEAGUE 17 HOCKEY 15 HANDBALL 4 RACQUET GAMES 4 SKIING 2 BASKETBALL 2 FENCING LACROSSE MARTIAL ARTS ICE HOCKEY GYMNASTICS WATERPOLO ROWING "STRONGMAN" WEIGHT LIFTING 2 2 3 2 1 1 1 1 1 _______________________ TOTAL 407 SYMPTOMS DURING EXERCISE PAIN IN GROIN INCREASES WITH RUNNING STRIDING SPRINTING SUDDEN MOVEMENT TWISTING & TURNING SIDE STEPPING JUMPING DEAD BALL KICKING LONG BALL KICKING (BUT NO SWELLING) SYMPTOMS AFTER EXERCISE STIFF & SORE PAIN IN GROIN INCREASES WITH TURNING IN BED GETTING OUT OF BED GETTING OUT OF CAR SIT UPS COUGHING SNEEZING SUDDEN MOVEMENT MRI in Groin Disruption MRI Poor in Abdomen Resolution insufficient for subtle changes But Inguinal ligament – clearly visible Hernia Gross Scar Tissue Defects / Gaps Significant Disruption Also visible MRI Good in Pelvis & Thigh Adductor Tear clearly seen Osteitis pubis HIP Pathology David Connell 2009 Ultrasound in Groin Disruption State of Art Ultrasound Equipment – required Subtle changes in Inguinal ligament Conjoined Tendon maybe seen Dynamic assessment – Essential Abdominal straining Sonopalpation Tender over Inguinal Canal Bulging Post. Wall HERNIA: Shows Clearly as Peritoneal Sac or Protrusion David Connell 2009 31 Years No Groin Patient Complained of Swelling INDICATIONS FOR SURGERY Groin Disruption PROFESSIONAL AND AMATEUR FAILED CONSERVATIVE TREATMENT INDICATION FOR SURGERY: PROFESSIONALS GAME INHIBITED TRAINING INHIBITED LOSS OF SPEED LOSS OF FITNESS INDICATION FOR SURGERY: AMATEURS SYMPTOMS AFFECT EVERYDAY LIFE LOSS OF SPORT AFFECTS QUALITY OF LIFE GROIN DISRUPTION: PATHOLOGY Found at Operation TORN EXTERNAL OBLIQUE ==== DILATED SUPERFICIAL INGUINAL RING TORN CONJOINED TENDON CONJOINED TENDON } DEHISCENCE INGUINAL LIGAMENT ( 40% also have Adductor Pathology) Groin Disruption Surgery Groin Reconstruction • • • • • Normal Anatomy - Restored Each layer – Repaired Each Injury- Repaired Permanent Suture – Essential Nylon Darn / Ethilon Darn • Preferable to Absorbable Sutures (Don’t Last) • Preferable to Mesh (May Restrict Mobility) CONJOINED TENDON REPAIR TRASVERSALIS FASCIA PLICATED with O Vicryl TENSION FREE NYLON DARN (CONJ. TENDON to ING. LIG) EXT OBLIQUE REPAIR (NEW S.I.R) GROIN DISRUPTION & ADDUCTOR TEAR PRESENT IN 40% HALF REQUIRE ADDUCTOR TENOTOMY HERNIA IN SPORTSMEN No evidence of increased incidence of Hernia in Sportsmen Groin Disruption/Gilmore’s Groin Neither Hernia or Pre Hernia Terminology HERNIA: Incorrect D QUOTE “Jerry I had your “Groin” in 74, As did my colleague Alan Mullery We both had to rest for months There was no other treatment then” Terry Venables 2006 B HERNIA A Protrusion of a Viscus beyond it’s normal confines E HERNIA (2% MALES IN UK) INGUINAL 73% FEMORAL 17% (Bailey & Love ) GROIN HERNIA INGUINAL – DIRECT INDIRECT FEMORAL OBTURATOR INDIRECT INGUINAL HERNIA PRESENTATION Usually young males Swelling only occurs with standing/straining Swelling can be difficult to reduce If swelling persists - Pain H HERNIA: INDICATION FOR SURGERY Swelling which when present causes pain or discomfort Irreducible swelling Strangulation INDIRECT INGUINAL HERNIA OPERATION Herniotomy (Excise Indirect Sac) Reconstitute Inguinal canal (Repair only necessary if post wall defect) DIRECT INGUINAL HERNIA Protrusion of Viscus through Post Inguinal Canal Wall Due to defect in Post Wall I DIRECT INGUINAL HERNIA PRESENTATION Swelling readily appears with Coughing or Standing Swelling reduces when lying down Patient often complains of discomfort with Standing e.g. cocktail parties or window shopping (Sport rarely Restricted)J K DIRECT INGUINAL HERNIA OPERATION Reduce Peritoneal Sac Insert Mesh Close Ext Oblique & Skin FEMORAL HERNIA Protrusion through Femoral Canal Swelling: Below and lateral to pubic tubercle i.e. Upper thigh FEMORAL HERNIA OPERATION Reduce Sac contents Excise Sac Suture Lacunar to Inguinal ligament SYMPTOMS & PATHOLOGY Groin Disruption/Gilmore’s Groin Significantly different to Hernia Inguinal Femoral Obturator Only similarity: SITE CORRECT SURGICAL TREATMENT ALWAYS DEPENDS ON ACCURATE DIAGNOSIS Of PATHOLOGY PATHOLOGY in Groin Disruption/Gilmore’s Groin Significantly different to Hernia REPAIR using Hernia Mesh Technique Open or Laparoscopic Usually FAILS 8% our Operations in Patients with Previous Groin Repair “I have had the mesh repair But I can still feel a tear behind the mesh My symptoms have not improved” P.W Patient 2009 F QUOTE “General Surgeons in this area either do not recognise Gilmore’s Groin or They treat it as a Hernia with mesh repair, which fails” Johnny Morris Sports Medicine Physician A Hampshire 2011 Conclusion:Wrong Diagnosis Resulting in Wrong Operation DOES NOT CURE OFTEN COMPLICATES SIGNIFICANT DELAY in RECOVERY or RESULTS IN FAILURE F Patients with Groin Problems Deserve a GROIN SURGEON 16.06.2011