Plan
•
Disorders of penis
•
Malformations
•
Acquired disorders
•
Semen analysis
•
Male infertility - investigations
Penis
Congenital
Acquired disorders
Penis
Congenital
Acquired disorders
inflammatory
neoplasms
congenital disorder
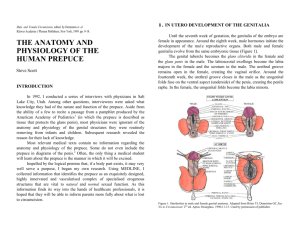
Malformations
abnormality in the location of distal urethral orifice
Hypospadias (opening of urethra along ventral
aspect)
epispadias (opening of urethra along dorsal
aspect)
congenital disorder
Malformations
abnormality in the location of distal urethral orifice
Hypospadias (opening of urethra along ventral
aspect of penis)
more common (1 in 300 live male births)
urinary obstruction common
associated with other genital anomalies
inguinal hernia
undescended testis
congenital disorder
Malformations
abnormality in the location of distal urethral orifice
Epispadias (opening of urethra along dorsal
aspect of penis)
Epispadias
Phimosis
Orifice of prepuce is too small to permit normal retraction
over the glans penis
Maybe due to
Anomalous development
Scarring of preputial ring following infections
Importance
Interferes with cleanliness
Accumulation of secretions and detritus under prepuce
Favours development of infection and carcinoma
Paraphimosis
•
When a phimotic prepuce is forcibly retracted
over the glans penis, marked constriction and
subsequent swelling of glans may prevent
replacement of prepuce creating paraphimosis
•
Condition extremely painful
•
Potential cause of acute urinary retention due
to urethral obstruction
Paraphimosis
•
Phimosi
s
Inflammations
•
Invariably involve the glans and prepuce
•
•
Specific infections
•
Syphilis, chancroid, granuloma inguinale
•
Genital herpes
Non specific infections
•
Balanoposthitis: caused by
•
Candida albicans
•
Anerobic bacteria
•
Gardnerella
•
Pyogenic bacteria
Inflammations
•
Pathogenesis
•
Consequence of poor local hygiene in uncircumcised males
•
accumulation of desquamated squamous cells, sweat and
debris - SMEGMA - acts as local irritant
•
Persistence of infection leads to scarring - phimosis
Tumours
•
Benign
•
Malignant
•
Premalignant
Condyloma Acuminatum
•
Benign tumour
•
Caused by Human papilloma Virus - HPV
•
Related to common wart (verruca vulgaris)
•
Occurs on moist mucocutaneous junctions
•
HPV and associated diseases are sexually
transmitted
•
Type 6 and type 11 associated with
Condylomata Acuminata
Morphology
•
May occur on genital or perineal areas
•
On penis occurs commonly about the
coronal sulcus and inner aspect of
prepuce
•
Single or multiple
•
Sessile or pedunculated
•
Red papillary excrescences
•
Vary from 1 mm to several mms
Histology
•
Branching, villous, papillary connective tissue
stroma
•
Covered by epithelium which may have
hyperkeratosis and thickening of epidermis
(acanthosis)
Histology
Orderly maturation of epithelial cells
Clear vacuolization of prickle cells
Basement membrane intact, no evidence of infl
Clinical course
•
Tend to recur
•
Do not evolve into cancers
Tumours
•
Uncommon
•
Most frequent is carcinoma and benign epithelial tumour
- condyloma acuminatum
•
Other forms - carcinoma in situ - Bowens disease
Malignant tumors
•
Carcinoma insitu
•
Invasive carcinoma
Carcinoma in situ
•
Histologic term
•
Epithelial lesion
•
Cytologic changes of malignancy are limited to the
epithelium
•
No evidence of local invasion or distant metastasis
•
Considered precancerous condition
•
Potential to evolve into invasive cancer
Carcinoma in situ
•
•
In the male external genitalia there are two distinct
lesions that show carcinoma in situ
•
BOWEN Disease
•
BOWENOID papulosis
Lesions strongly associated with HPV type 16
Carcinoma in situ
•
Bowen Disease
•
Genital region of both men and women
•
Usually over the age of 35 years
•
In men it involves: skin of shaft of penis, scrotum
•
Grossly: appears solitary thickened gray white
opaque plaque with shallow ulcerations and
crusting
•
When it occurs on glans or prepuce - single or
multiple shiny red velvety plaques - clinically
referred to as Erythroplasia of Querat
Carcinoma in situ
•
Bowen Disease
•
Histology
•
Proliferation of epidermis
•
Numerous mitosis, some atpical
•
Cells markedly dysplastic
•
Large hyperchromatic nuclei
•
Over years 10% may transform in carcinoma
Carcinoma in situ
•
Bowenoid papulosis
•
Occurs in sexually active adults
•
Younger age of patients
•
Presence of multiple pigmented (reddish brown)
papular lesions, some cases maybe verrucoid
mistaken for Candyloma acuminatum
•
Histologically indistinguishable from Bowen
disease, related to HPV 16
•
Never develops into invasive carcinoma
•
Many cases spontaneously regress
Invasive Carcinoma
•
Common in Asia 10% to 20%
•
Uncommon in United states. Less than 1%
•
Striking correlation between Circumcision and
occurrence of carcinoma
•
Circumcision confers protection
•
Extremely uncommon in Jews and Moslems
Invasive Carcinoma
•
Circumcision associated with better genital
hygiene
•
Reduces exposure to carcinogens that are
concentrated in Smegma
•
Decreases likelihood of infection with
potentially oncogenic HPV
•
HPV type 16 is the most common, also HPV
18
Invasive Carcinoma
•
Carcinoma in situ - 80% associated with HPV
•
Invasive carcinoma - 50 % association-HPV
•
Indicates that HPV alone may not be sufficient
to convert Ca in situ to invasive malignancy.
Requires other carcinogenic influences like
•
Cigarette smoking
Verrucous carcinoma
•
Uncommon
•
Well differentiated variant of squamous
carcinoma
•
Has low malignant potential
•
Locally invasive, can invade the underlying
tissue
•
Rarely metastasize
•
Has a papillary appearance similar to
condyloma but larger in size
Invasive Carcinoma
•
Morphology
•
Usually begins on glans or inner surface of
prepuce near the coronal sulcus
•
Two macroscopic patterns
•
Papillary : simulate condylomata,
produces cauliflower like fungating
masses
•
Flat : appear as epithelial thickening
accompanied by graying and fissuring.
Invasive Carcinoma
•
Clinical course
•
Slow growing
•
Locally invasive
•
Lesion not painful unless ulcerated/infected
•
Bleed frequently
•
Early metastases to inguinal and iliac nodes
•
Prognosis related to stage of tumor
•
Prognosis poor if regional lymphnodes are
involved
Semen Analysis
Male infertility - investigations
Semen analysis
Constituents
spermatozoa
secretions from
testes
epididymis
prostate
seminal vesicle
bulbourethral glands
Semen analysis
evaluation of reproductive dysfunction
selection of donors for therapeutic
insemination
to monitor the success of surgical procedures
varicocelectomy
vasectomy
Semen analysis
Includes
Microscopic evaluation
Macroscopic evaluatin
Semen analysis
Includes
Microscopic evaluation
Concentration
Motility
Morphology
agglutination
Macroscopic evaluation
physical
chemical properties
Semen analysis
Macroscopic evaluation
Liquefaction - normal : within 60 minutes
Appearance - After liquefaction - homogenous
grey opalescent
Volume - 2 to 5 ml
Viscosity
pH : 6.4 to 8.0
Semen
analysis
Includes
Microscopic evaluation
Concentration
Less than 20 mill/ml - Oligospermia
Motility
less than 50% motile sperms Asthenospermia
Morphology
Less than 50% normal morphology Teratozoospermia
agglutination
Semen analysis
Classification of sperm morphology
Head defects
Neck and mid piece defects
Tail defects
Cytoplasmic droplets
Semen analysis
Biochemical assays
prostate gland
Citric acid, Zinc, GGTP, Acid phosphatase
Seminal vesicle
Fructose and prostaglandins
Epididymis
Free L carnitine, glycerophosphocholine
Male infertility
Semen analysis
FSH/Testosterone
Anti sperm antibodies
FNAC/biopsy of testes
Ctogenetics