Potentially
Preventable
Readmissions
RARE Mental Health Collab.
Place picture here
Mark Sonneborn
February 2014
What are PPRs?
• 3M software
• Based on MHA administrative data
• Measures readmissions to the same facility only
o ~ 22% go to different facilities, per literature
How to interpret the reports
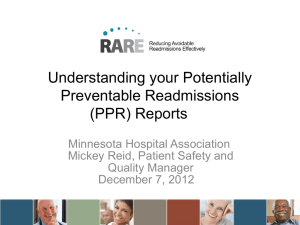
General Guidelines for PPRs
Readmission
Initial Admission
Medical
Surgical
Medical
Surgical
PPR except if clearly
unrelated acute events
Not PPR unless initial
medical diagnosis clearly
should have resulted in
surgery
PPR except conditions
© 3M 2007. All rights reserved.
clearly unrelated
PPR if related to prior
surgery
PPR Global Exclusions
If any of the following conditions apply to the initial admission, a
subsequent readmission is globally excluded from consideration as a
PPR
• Admissions for which follow-up care is intrinsically extensive and
complex
o Major or metastatic malignancies treated medically
o Multiple trauma, burns
• Discharge status indicates limited hospital & provider control
o Left against medical advice
o Transferred to another acute care hospital
• Neonates
• Other exclusions
o Specific eye procedures and infections
o Cystic fibrosis with pulmonary diagnoses
• Died – not included as candidate initial admissions (denominator)
© 3M 2007. All rights reserved.
Clinical Factors make a readmission not
potentially preventable
No clinical relationship to prior discharge
• Cholecystectomy two weeks after hip replacement
Discharge status of prior discharge
• AMA and transferred to another acute care hospital
Type of prior discharge
• Follow-up care is intrinsically complex and extensive
o
Metatastic malignancies, Multiple trauma, Burns
Longer interval between discharge and
readmission
• Long time intervals (>30 days) reduce confidence that
readmission is causally linked to the prior discharge
© 3M 2007. All rights reserved.
Non- PPR Reasons
© 3M 2007. All rights reserved.
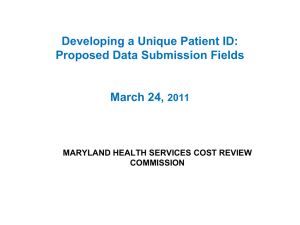
How to interpret PPR results –
Hospital-level
At Risk Actual Expected
Expected
PPRs Cases Rate
Rate
PPRs
172
3,820
4.5
5.0 **
192.3
Target
Difference
PPRs
from Target A/E Ratio
0.90
153.9
18.1
PPRs is the actual number of PPRs detected
during the time period
How to interpret PPR results –
Hospital-level
At Risk Actual Expected
Expected
PPRs Cases Rate
Rate
PPRs
172
3,820
4.5
5.0 **
192.3
Target
Difference
PPRs
from Target A/E Ratio
0.90
153.9
18.1
“At Risk Cases” is the denominator – it’s all cases
minus the exclusions mentioned before
How to interpret PPR results –
Hospital-level
At Risk Actual Expected
Expected
PPRs Cases Rate
Rate
PPRs
172
3,820
4.5
5.0 **
192.3
Target
Difference
PPRs
from Target A/E Ratio
0.90
153.9
18.1
Actual Rate is PPRs divided by At Risk Cases
How to interpret PPR results –
Hospital-level
At Risk Actual Expected
Expected
PPRs Cases Rate
Rate
PPRs
172
3,820
4.5
5.0 **
192.3
Target
Difference
PPRs
from Target A/E Ratio
0.90
153.9
18.1
Expected Rate – this is a unique number for every
hospital based on their patient population.
Generally, hospitals with more severely ill patients
will have higher expected rates.
How to interpret PPR results –
Hospital-level
At Risk Actual Expected
Expected
PPRs Cases Rate
Rate
PPRs
172
3,820
4.5
5.0 **
192.3
Target
Difference
PPRs
from Target A/E Ratio
0.90
153.9
18.1
One star is statistically “worse than expected” (or
higher); Two stars is “no different than expected”; Three
stars is “better than expected” (or lower)
How to interpret PPR results –
Hospital-level
At Risk Actual Expected
Expected
PPRs Cases Rate
Rate
PPRs
172
3,820
4.5
5.0 **
192.3
Target
Difference
PPRs
from Target A/E Ratio
0.90
153.9
18.1
Expected PPRs is the Expected Rate times the At
Risk Cases
How to interpret PPR results –
Hospital-level
At Risk Actual Expected
Expected
PPRs Cases Rate
Rate
PPRs
172
3,820
4.5
5.0 **
192.3
Target
Difference
PPRs
from Target A/E Ratio
0.90
153.9
18.1
Target PPRs is 20% less than Expected PPRs
How to interpret PPR results –
Hospital-level
At Risk Actual Expected
Expected
PPRs Cases Rate
Rate
PPRs
172
3,820
4.5
5.0 **
192.3
Target
Difference
PPRs
from Target A/E Ratio
0.90
153.9
18.1
Difference from Target is your actual PPRs (first column)
minus the Target PPRs.
The goal for this hospital is to reduce by 18 PPRs per
year.
Actual to Expected Ratio
Actual
Expected
Rate
Rate
4.5
5.0
A/E Ratio
0.90
An A/E Ratio above 1.0 is more than expected; below
is less than expected.
The goal for the RARE campaign is to get the A/E ratio
down to 0.80
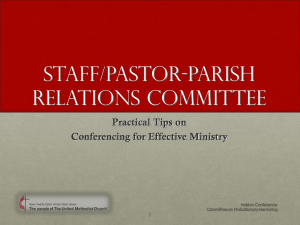
Example Detail (Record-level) Report
ACCTNB MEDREC ADMIT_Y ADMIT_
R
NO R
MM
2013 05
2013 07
2013 05
2013 05
2013 08
2013 03
2013 09
2013 07
2013 09
2013 05
2013 07
2013 04
ADMIT_
DD
11
03
06
23
10
23
16
01
11
03
16
16
DISCHAR DISCHAR DISCHAR APR_DR
PPR_DAY RECORD
GE_YR GE_MM GE_DD G
APR_SOI S
_TYPE
2013 05
13
140
1 #NULL! OA
2013 07
10
207
1 303 OA
2013 05
07
513
1 #NULL! IA
2013 05
25
813
2
16 RA
2013 08
13
560
2 #NULL! OA
2013 04
02
460
3
15 RA
2013 09
17
246
2 #NULL! OA
2013 07
03
302
2 #NULL! OA
2013 09
12
223
1 #NULL! OA
2013 05
05
249
1 #NULL! OA
2013 07
18
560
1 #NULL! OA
2013 04
17
560
2 #NULL! OA
PDX
49121
4589
6262
99831
65811
5849
5579
71536
5409
27651
64511
66341
DISCHAR
GE_STAT
US
MDC
1
3
1
1
1
3
1
1
1
1
1
1
NORM_R
ATE DRG
4 0.094996 192
5 0.051087 315
13 0.020316 743
21 0.070496 920
14
0 774
11 0.114181 683
6 0.044374 395
8 0.028048 470
6 0.092424 343
6 0.032941 641
14
0 775
14
0 775
Detail Reports
• Acct #, Med Rec #
• Admit, Discharge Date
• APR-DRG, APR-DRG Severity of Illness
This is what the statewide norms are based on
• PPR days
Days between discharge and admission
• Record Type
2-letter codes – THIS IS THE KEY FIELD
• Principal Diagnosis, MDC, DRG
• Discharge Status
• Statewide Norm
Hints for Using Detail Reports to
Analyze Performance
Find patients that had potentially preventable
readmissions
• IA (Initial Admissions) have at least one affiliated RA
(Readmission)
o All of the other two-letter codes are not for patients that were
readmitted
Use A/E ratio results from hospital-level report to
hone in on certain types of cases
Look for patterns and characteristics of readmitted
patients vs. non-readmitted
• Are there differences in demographics or diagnoses?
Questions?
Mark Sonneborn,
msonneborn@mnhospitals.org