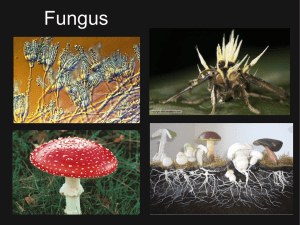
Mycology is the study of
•
•
•
•
•
•
•
•
Beer
Wine
Bread
Cheese
Gourmet mushrooms
Environmental toxins
Biodegradation
Diseases caused by fungi
KINGDOM
CHARACTERISTIC
EXAMPLE
Monera
Prokaryocyte
Bacteria
Actinomyces
Protista
Eukaryocyte
Protozoa
Fungi
Eukaryocyte *
Fungi
Plants
Eukaryocyte
Plants
Moss
Animals
Eukaryocyte *
Arthropods
Mammals
Man
Fungi
• Commonly present in nature as saprophytes,
transiently colonising or etiological agenses.
Frequently present in biological samples. They role in
pathogenesis can be difficult to determine.
Effect of fungi
• Mycetismus – preformed toxins ergotamine alcaloids,
psychotropic substances,
• Mycotoxicoses – aflatoxines, chronical exposition
• alergic reaction – air mycelium alergic pneumonia,
rhinitis, bronchial asthma, aleveolitis, atopic reaction
colonisation and disease – inborne immunity, diseases
are short, self limiting
• Infections
Immunocompetent : superficial, skin, subcutaneous,
systemic
Immunocompromised and AIDS: fungi with low
patogenicity – oportunictic mycoses
Biology and classification
•
•
•
•
•
•
•
Eukaryoric cells
Nucleus, nuclear membrane
Multilayered rigid cell wall
Cell wall with sterols,
Without chlorophyll
Not photosyntetic
Heterotrophic metabolisme – saprophytic, comensals, parasits
Biology and classification
• Yeast - C. albicans
One cell, asexual reproduction by budding (blastoconidia) or by
division. They ca produce filamentous structueres resempling
molds – pseudohyphae, elongated cells resembling sausages
Biology and classification
• Molds(hyphae) – elongation at both ends, can be
multinucleated – coenocitic or septated
The complex of hyphae is known as mycelium
If implemented to the substrate – vegetative
If on the surface - air – releasing specialised structures –
conidia serving as propagation structures – asexual
conidia, dissemination, identification
Patogenic potential of fungi
• Usually exogenous – exept. Candidosis
• Longlasting exposition of man to fungi,
• Pathogenesis depend on nonspecific immune
mechanism – skin, mucous membrane, IDS
• Presence of fatty acids, acidic pH, epitelium,
physiological microbial agens, transferrin
Tools of pathogenicity
• Dermatophytes – co0lonisation of skin, hairs, nails –
ensyme keratinase
• Dimorfic fungi – as molds in the nature, as yeast in
tissues Candida – yeast becomes filamentous during
invasion of tissue
• Capsule - Cryptococcus neoformans
*Primary pathogens - Histoplazma capsulatum,
Blastomyces dermatitis, Coccidioides immitis
* Oportunistic pathogens - Aspergillus, Candida,
Mucor
MORE MYCOTIC INFECTION or
REVIVED INTEREST IN MYCOLOGY
1.
2.
3.
4.
5.
6.
7.
Increased frequency of mycotic diseases
Increased awareness by physicians
Better trained laboratory personnel
More invasive procedures used on patients
Increased use of immunosuppressive drugs
Increase in immunosuppressive disease
Better laboratory diagnostic tools
Mycotic Diseases Are
NOT
Contagious with the
exception of
dermatofytes
ESTABLISHMENT OF INFECTION WITH A
MYCOTIC AGENT DEPENDS ON
1. Inoculum size
2. Resistance of the host
Laboratory diagnosis
• Primary pathogens – microscopy of tissue
sample+cultivation
• Oportunistic pathogens – often only contamination, !
Interpretation! Repeated isolation and presence of
fungi in biological sample by microscopy
* Methods of sampling - sterility, desinfection of the
place of sampling (skin, nails, hairs) 70% etanol + dry,
eschariation.
* Procedure: material +10% KOH (destruction of
tissue,, fungi pocess chitin that resist alkaline solution
– mikrosscopy of hyphae – rice agar microscopy or
staining sc. Gomori, Schiff
- cultivation on selective media at 25 and 37.C
Diagnosis
1. Wet Mount
2. Skin test
3. Serology
4. Fluorescent antibody
5. Biopsy and histopathology
6. Culture
7. DNA probes
Cultivation media
• Selective
• Sabouraud agar - dextrose, pepton, less agar, pH 5,5
– acid environment and high concentration of glc
• Saprophytic fungi can overgrow pathogenic – addition
of chloramphenicol (against bacteria) and
cyclohexamid (aganinst saprophytic fungi).
• Recommendation of cultivation on media with and
without ATB, always in 25 and 37*C ( some fungi do
not grow at 37+ H. capsulatum)
• Identification: all are G+, yeat are growing as bacterial
colonies, fungi – longer – several days and even
weeks, microscopy – rice agar block - morphology
THERAPY
Because they are eukaryotic, fungi are
biochemically similar to the human host.
Therefore it is difficult to develop
chemotherapeutic agents that will
destroy the invading fungus without
harming the patient.
Antimycotics
• Polyensy - amfotericin B, nystatin
Azoles – interference with ensymes depending on
cytochromes and acting during demetylation of
lanosterol to ergosterol - miconazol,ketoconazol,
flukonazol,
Nucleotides – inhibition of DNA a RNA
synthesis - 5 fluorocytosin
Grisanes – inhibition of the function of microtubules
KJ – activation of lysosomal ensymes
• Longlasting therapy, monitoring of the patient
• Susceptibility testingovanie – not standardised
IN FUNGAL THERAPY
We attempt to induce cell injury by
causing the cell membrane of the fungus
to become permeable.
PROBLEM
Finding an agent that will selectively injure
fungal cell walls without damaging the host
cell.
PRIMARY ANTI-FUNGAL
AGENTS
1. Polyene derivatives
–
–
Amphotericin B
Nystatin
2. Azoles
–
–
–
–
–
Ketoconazole
Fluconazole
Itraconazole
Voriconazole
Posaconazole
Mycoses
• According to the tissue
• Superficial – superficial layer of skin and
hairs
Skin – epidermis and adnexes
Subsuperficial or subcutaneous - dermis,
deeper tissues, muscles, fasciae - traumatic
• Systemic – primary pathogenic fungi –
endemic, dimorfic
• Oportunistic – non pathogenic fungi, or fungi
causing usually localised infection – spread and
cause life threating infection
Superficial
• Cosmetic destruction of stratum corneum and cuticula
of hair, without cell immunity reaction of the patients
• Skin - Malassezia furfur (pityriasis versicolor) microscopically „spagetti look)
- Exophiala wernecki ( tinea nigra) - microscopically,
cutivation - dimorphismus – brown colonies and
hyphae
• Hairs - Piedraia hortoe (black piedra) – direct
microscopy of hair
- Trichosporon beigelii (white piedra) – direct
microscopy of hair, dimorphismus
• Th: keratolytical local substances (salicylates),
miconazol – interfer synthesis of ergosterol, hygiene,
relapsing
Cutaneous - dermatophytes
• Skin, hairs, nails – only on the areas of skin and
adnexes containing keratin. Cell immunity reaction
• Clinical manifestation – worm-like serpentin or ring-like
• More than 100 species - dermatophytes.
Trichophyton, Epidermophyton, Microsporum
anthropofil (chronic anoying infections), zoophil and
geophil dermatophytes (inflamatory reaction,
selflimiting) – good prognosis
Certain are endemic, age related
• Therapy: skin – local - miconazol, clotrimazol,
econazol hair - griseofulvin p.o., fungistatic
•
Laboratory diagnosis of
dermatophytes
Sampling and processing with KOH
Microscopy
- branching septated hyphae from skin and nails
- spores in or surrounding hair
- Trichophyton schoenleinii – vax-like substance of
hyphae surrounding base of hair folicules –
microscopy indentify just the mycotic ethiology. For
species identification cultivation. Selektive medium
with ATB and cyclohexamid at 25* - as long as 4
weeks.
• mycelia are not diagnostic - microscopy and
identification acc.to conidia
Subcutaneous Mycoses
• Confined to subcutaneous tissue and
rarely spread systemically. The causative
agents are soil organisms introduced into
the extremities by trauma
Subsuperficial, subcutaneous
• Wide spectrum of infections usually after traumatic
innoculation (thorn, tick, wood, nail – deeper layers,
chronical process, spread under epidermis.
• Localised usually on extremities
• Dif. dg. actinomycoses, mycetoma, atypical
mycobacteriosis.
• Therapy can be frustrating, radical, surgery,
amputation.
• exotické
• Sporothrix schencki – lymphocutanneous or
disseminated
• Mycetom
• Other subcutaneous mycoses - zygomycosis,
Mycetom
- clinical unit
- caused by bacteria (Actinomyces izraelí, Nocardia
asteroides, Streptomyces, Actinomadura) or fungi (Madurella
grisea, )
Dg: pus from liquid from sinuses
- macroscopic granules,
- microscopic
Th: important to identify the ethiology bacterial or mycotic, total
surgical excision, amputation
Systemic Mycoses
• Involve skin and deep viscera
• May become widely disseminated
• Predilection for specific organs
Dimorphic Fungi
• Yeast Form
• Parasitic form
• Tissue form
• Cultured at 37 C
• Mycelial Form
• Saprophytic form
• Cultured at 25 C
Sytemic mycoses
• Primary pathogenic: (dimorfic - Histoplasma capsulatum,
Blastomyces detmatitidis, paracoccidioides brasiliensis,
Coccidioides immitis Crytococcus neoformans
• C. neoformans – is the only monomorfic - at 25 and 37* yeast, mucopolysacharide capsule
• Primary place of infectione - lung – usually asymptomatic
infection. If sec. spread - dissemination
• Usually endemic
• Cryptococcosis – torulosis, european blastomycoses.
Not dimorphismus: 4 serotypes A,D and C,B
Virulence - capsule
- asymptomatic lung disease – solitary lung nodul – imitation of
Ca, symptomatic pneumonia – difuse infiltration
- hematogenous dissemination - meningitis (headache,
longlasting fever,
- skin lesions, lysis of bones.
Dg detection of antigen – polysacharide capsule - latex
agglutination Burri method.
Cultivation
Discrimination of pathogenic and not pathogenic – growth at
41*C – patogenic do not grow
Th amfotericin B, 5 fluorocytosin CNS - 10 weeks,
• Blastomycosiss - lung disease, often
innaparent, later ulceros lesion on skin and
bones.
Dg. – serology immunodiffusion, skin test,
cultivation of the tissue and microscopy –
budding yeast cells.
Identification by dimorfismus.
Th - amphotericin B, in non complicated lung ketokonazol
• Coccidioidomykóza
- inhalation, asymptomatic or life threating, meningitis.
Dimorphismus – filamentous in the nature (cylindric conidia).
In the tissue multinuclear structures changing to endospores
with one nucleus growing and developing to new spherules
Endemic.
Dg. Serology imunodifusion, precipitation (early stages) or
CF(later stages), skin test
Th. Amfotericin B (poorly enter to CSM). Ketokonazol –
intrruption of the infection - relapses after interruption of the
therapypo prerušení liečby.
• Paracoccidioidomycosis – lung disease after
inhalation – asymptomatic, or ulcerouse forme
in mouth or nos or progresive lung or systemic
infection.
• Clinically usually in men
• Dimorfic – mold in nature, yeast in tissue diagnostic
Dg. Serology immunodiffusion, histology,
cultivation 14 days at 25*C - mycelium –
transport to 37*C – change of the phase – to
yeast
• microscopy („ captain wheele“ – central cell with
• Histoplasmosis - asymptomatic or influenza-like, big exposition
– pneumonia with rare complications – pericarditis, fibrosis of
mediastinum.Diseminated in immunocompromised.
• Dg.-serologically CFR, imunodifusion (antigen histoplasmin –
• - histological,
- cultivation (sputum, microscopy - long.
- skin test with histoplasmin (questionable).
- Ag detection in blood and urine.
• Th: amfotericin B
Oportunistic mycoses
• Usually well tolerated without sequelae with the
exception of alergic hypersensitivity.
• High degree of inborne resistance against colonisation
with fungi, low degree of virulence of fungi
• If immunodeficiency – life threating diseases (AIDS,
drugs, irradiation, cytotoxic therapy)
• Most common - Candida albigans, Aspergillus
fumigatus, Rhizopus -
•
•
•
•
•
•
Candidosis
Candida sp. – part of normal physiological microbial flora
(mucous membrane of mouth, vagina, rectum), colonisation
without symptomes. Seldom on skin. Hemataogenous
dissemination from oropharynx or GIT if injury of m.m.,
chemtherapy, contaminated catheters (usually endogenous
infection
Lung, spleen, kidneys, liver, heart, brain, eye, skin lesion during
dissemination. Hemocultivation is usually negative.
Localised infection of skin and nails (dif.dg.from
dermatophytosis) Infection of m.m. of mouth, vagina,
aesophagus, brochi
Chronic mucocutaneous candidosis
Disseminated candidosis
Imunity – mostly cellular
Th: local for skin and mucocutaneous inf.
Systemic and nail -amfotericín B a 5 fluorocytozín, ketokonazol
Dg of candidosis
• Usually blastospores, pseudohyphae and
septated hyphae.
• C.glabrata –only yeast
• Colonies - big, cream like
• Rapid test of - C. albicans - germ tubes test –
hyphae propagules when cultivated in human
serum
Aspergilosis
• Aspergilosis - exogenous infection
• . A. flavus, A. fumigatus.
• Cause only opportunistic infections.
Alergic aspergilosis, secundary colonisation, systemic
aspergilosis
• Lab.dg.: regularly septated hyphae, oriented in one direction in
the sample
• Cultivation usually negative
• Invasive disease – repeated isolation from the same place
zygomycosis
• Zygomycosis (mucormycosisa, phycomycosis)
- usually in the environment
• Similar to asperfilosis
• Coenocitic hyphae
• Infection from paranasal sinuses, spreading to orbita and brain
• Terminal stage of patients in acidosis in metabolic disorders
(DM)
• Invasive after colonisation of burned places
• When disseminating – predilection to big vessels, embolisation,
ischemia, necrosis
• .Dg.: filamentose, coenocytic
Opportunistic Mycoses
Infections due to fungi of low
virulence in patients who are
immunologically compromised
PATHOGENIC FUNGI
•
NORMAL HOST
•
•
•
•
Systemic pathogens - 25 species
Cutaneous pathogens - 33 species
Subcutaneous pathogens - 10 species
IMMUNOCOMPROMISED HOST
Opportunistic fungi
- 300 species
HOST-PATHOGEN EQUILIBRIUM
NUMBER OF ORGANISMS X VIRULENCE
HOST RESISTANCE
=
DISEASE
Opportunistic Fungi
1. Saprophytic - from the environment
2. Endogenous – a commensal organism
MOST SERIOUS
OPPORTUNISTIC INFECTIONS
• CANDIDA SPECIES
• ASPERGILLUS SPECIES
• MUCOR SPECIES (ZYGOMYCES)
CLINICAL PRESENTATION
1.
2.
3.
4.
5.
Atypical Signs and Symptoms
Unusual Organ Affinity
Outside Endemic Area
Unusual histopathology
Unusual Pathogens
CLINICAL PRESENTATION
1.
2.
3.
4.
5.
Atypical Signs and Symptoms
Unusual Organ Affinity
Outside Endemic Area
Unusual histopathology
Unusual Pathogens
CLINICAL PRESENTATION
1.
2.
3.
4.
5.
Atypical Signs and Symptoms
Unusual Organ Affinity
Outside Endemic Area
Unusual histopathology
Unusual Pathogens
CLINICAL PRESENTATION
1.
2.
3.
4.
5.
Atypical Signs and Symptoms
Unusual Organ Affinity
Outside Endemic Area
Unusual Histopathology
Unusual Pathogens
CLINICAL PRESENTATION
1.
2.
3.
4.
5.
Atypical Signs and Symptoms
Unusual Organ Affinity
Outside Endemic Area
Unusual histopathology
Unusual Pathogens
MYCOLGISTS have more
FUNGI
 0
0