EGardner-pain path g..
advertisement

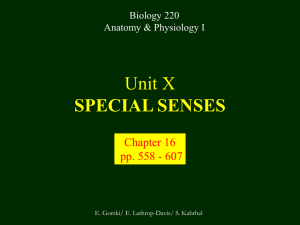
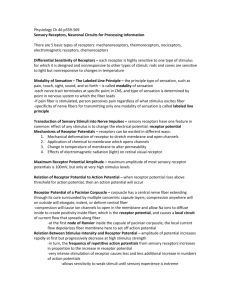
What is Pain? • “An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.” – International Association for the Study of Pain Pain and temperature sensed by free nerve endings Fiber diameter profile of peripheral nerves Heat and cold stimulate pain receptors (nociceptors) Temperature Sense • Normal skin temperature: T = 30-32 °C • Thermal sensations span four ranges: 1. Cold (T < 15 °C) 2. Cool (T > 15 °C and < 30 °C) 3. Warm (T > 35 °C and < 45 °C) 4. Hot (T > 45 °C) • Specific temperature-sensitive receptors code each range Thermal Receptors • Cold Receptors (TRPM8) – A-d fibers (thinly myelinated) – Stimulus: Cooling between T = 8 °C and 40 °C – Most sensitive at T = 25 °C – Saturate at T < 8 °C • Warm Receptors (TRPV3) – C fibers (unmyelinated) – Stimulus: Warming between T = 35 °C and 45 °C – Most sensitive at T = ~42 °C – Saturate at T > 45 °C Cold fibers signal rapid skin cooling Dynamic Response to Temperature Warm Receptors Code T > 35 °C Warm Receptors Saturate at High T Thermo-TRPs respond to specific temperature ranges TRP = Transient receptor potential Heat Nociceptors … and Burning Pain • A-d fibers (NS) or C fibers (HPC) • • • • Express TRPV1 and/or TRPV2 receptors Firing rate signals heat intensity at T > 45 °C Response outlasts heat stimulus Sensitize to repeated heat stimuli Noxious Cold (T < 10 °C) • Cold Fibers (TRPM8) – A-d fibers (thinly myelinated) – Saturate at T < 8 °C • Polymodal Nociceptors (HeatPinchCold) – – – – – C fibers (unmyelinated) Firing rate signals degree of cooling at T < 25 °C Fire at highest rates at T < 0 °C Express TRPA1, TRPV1 and TRPM8 receptors Paradoxical Cold: Freezing temperatures are perceived as burning pain Heat and cold stimulate specific groups of receptors What is Pain? • Aversive sensation • Intensity ranges from unpleasant to horrible • Various classes of pain – – – – pricking, stabbing, pinching (mechanical ) burning, freezing (thermal ) aching, stinging, soreness (chemical ) visceral (mechanical, chemical ) • Emotional component (pain tolerance) • Protective function – Warn of injury that should be avoided or treated Four classes of noxious (painful) sensations Heat pain Chemical Mechanical Cold pain Mechanical Nociceptors • Receptors specialized for painful mechanical stimuli (Nociceptive Specific) – A-d fibers (thinly myelinated) – Do not respond to light touch (high threshold) – Excited by strong pressure, pinch or squeezing – Mediate pain from skeletal muscle or viscera due to excessive stretch or contractile force – Most respond to noxious heat (T > 45 °C) Mechanical nociceptors respond to prick and pinch Polymodal nociceptors • • • • C fibers (unmyelinated free nerve endings) Respond to heat, pinch and cold (HPC receptors) Express TRPV1, TRPA1 and other TRP receptors Respond to irritant chemicals – – – – – Capsaicin (chili peppers): TRPV1 receptors Mustard oil, garlic, horseradish: TRPA1 receptor Low pH (acids) Endogenous peptides: Bradykinin, NGF Environmental irritants and pollutants Polymodal nociceptors express multiple receptors Nociceptors Respond to Chemicals • Exogenous chemicals that penetrate skin – Acids, alkalis, organic molecules – Capsaicin, Mustard oil • Intracellular molecules released by cell injury – Cations [K+, H+] – Peptides, neurotransmitters – Prostaglandins, histamine • Toxins [micro-organisms, insect bites, venom] • Pathological substances released by diseased tissue Tissue Damage Stimulates Nociceptors TRP receptors respond to pungent chemicals Garlic, radishes, mustard oil Menthol Camphor Capsaicin Irritant chemicals activate TRP receptors Inflammation sensitizes nociceptors Noxious stimuli are spread by axon reflexes Hyperalgesia Touch and pain fibers project to distinct spinal laminae Pain Inputs to Spinal Cord Lamina I Cells Respond Only to Pain • Mechanical and Heat (NS) • Cold • Polymodal (Heat, Pinch, Cold) • Irritant Chemicals (Histamine, Capsaicin, Mustard Oil) Small Fiber Inputs to Spinal Cord Touch and pain fibers project to distinct spinal laminae Referred Pain: Wide Dynamic Range Neurons Touch and Pain Ascend in Separate Tracts Visceral pain transmitted in the dorsal columns T10 Willis WD, et al. PNAS 96: 7675-7679, 1999 Central gray matter Pain Pathways to Thalamus and Cortex II Parallel Processing of Pain in Cortex • VPL/VPM —> SI Cortex – Pain localization to particular body site • VMpo —> Dorsal Insular Cortex – Pain sensation experienced (cold, heat, stab) • MDvc —> Anterior Cingulate Cortex – Pain emotional reaction • Hypothalamus and Limbic Cortex – Body physical response to pain – Subjective memory of pain Pain Centers in the Brain Apkarian et al. Eur J Pain 9: 463-484, 2005 How Can We Reduce Pain? • Remove the painful stimulus – Flexion reflex (hard-wired circuit to avoid pain) – Treat injury or pathology – Analgesics and/or antihistamines • Block impulse conduction in peripheral nerve – Local anesthetics, epidural anesthesia • Block synaptic transmission in CNS – General anesthesia – Narcotic analgesics (e.g. morphine) • Activate body’s own pain control system Gate Control of Pain Emotions Modulate Pain Transmission (nucleus cuneiformis) (periaqueductal gray) (dorsolateral pontine tegmentum) Endogenous Pain Inhibition Endogenous Opioid Peptides • Leucine-enkephalin – Tyr-Gly-Gly-Phe-Leu-OH • Methionine-enkephalin – Tyr-Gly-Gly-Phe-Met-OH • b-endorphin – Tyr-Gly-Gly-Phe-[26 amino acids]-OH • Dynorphin – Tyr-Gly-Gly-Phe-[13 amino acids]-OH Opiates & Opioids Modulate Pain Pain Prevention • Local anesthetics as supplements or • • • • alternatives to general anesthesia Intrathecal morphine intraoperatively Postoperative pain relief Physical therapy to stimulate large fibers Psychotherapy to optimize use of descending pain control pathways and improve pain tolerance Pain Perception Involves Multiple Processes Nociceptive Pain: Somatosensory response Inflammatory pain: trauma or disease Two Classes of Pain • Nociceptive or Inflammatory Pain (Acute) – Sensation transmitted by free nerve endings – Stimulus provided by noxious (harmful) mechanical, thermal or chemical input – Protective function • Neuropathic Pain (Chronic) – Abnormal firing pattern in PNS or CNS – Caused by lesion or trauma to nerve or CNS – Sensitization of central pathways due to excessive painful input Neuropathic Pain • Elicited by prolonged strong activation of nociceptors • Result of major injury – Trauma – Severe burns – Major surgery – Limb amputation – Peripheral nerve injury or neuroma – Postherpetic neuralgia Neuropathic pain: Nerve injury or CNS lesion Peripheral Sensitization Peripheral nerve injury Injured Schwann cells sensitize nociceptors DRG neurons respond to cytokines and ATP Central Sensitization … and Neuropathic Pain • Nociceptor synapses are glutaminergic • Strong stimulation activates NMDA receptors • LTP-like process increases synaptic efficacy through protein synthesis • Spinal synapses become more responsive to pain (hyperalgesia) and touch (allodynia) Glutamate receptor mechanisms Silent synapses and LTP Central Sensitization Mechanisms Pain begets pain (Pro-nociception pathways) Dysfunctional Pain: unknown cause Recommended additional readings (optional) Patapoutian A, Tate S, Woolf CJ. Transient receptor potential channels: targeting pain at the source. Nature Reviews: Drug Discovery 8: 55-68, 2009 Craig AD. How do you feel? Intero-ception: the sense of the physiological condition of the body. Nature Reviews Neuroscience 3: 655-666, 2002 Apkarian AV, Bushnell MC, Treede R-D, Zubieta J-K. Human brain mechanisms of pain perception and regulation in health and disease. Eur J Pain 9: 463-484, 2005 Tracey I, Mantyh PW. The cerebral signature for pain perception and its modulation. Neuron 55: 377-391, 2007 Porreca F, Ossipov MH, Gebhart GF. Chronic pain and medullary descending facilitation. Trends Neuroscience 25: 319-325, 2002 Costigan M, Scholz J, Woolf CJ. Neuropathic pain: A maladaptive response of the nervous system to damage. Annu Rev Neurosci 32: 1-32, 2009 Pain vocabulary • Hyperalgesia – Sensitization: enhanced sensation to noxious stimuli following injury – Stimulus provided by noxious mechanical, thermal or chemical input • Allodynia – Sensitization: abnormal response to touch – Caused by lesion or trauma to nerve or CNS • Analgesia – Pain relief and/or attenuation