2012 Stable Ischemic Heart Disease
(SIHD) Guideline Update
Jointly sponsored for CME credit by the
University of Nebraska Medical Center and
Practice Point Communications, Inc.
Supported by an independent educational
grant from Gilead Sciences Medical Affairs
Content Development Faculty
Julius M. Gardin, MD, MBA, FACC,
FACP, FAHA
Professor and Chair
Department of Medicine
Hackensack University Medical Center
Professor of Medicine
University of Medicine and Dentistry of New Jersey
New Jersey Medical School
Hackensack, NJ
2
Disclosure Information:
Content Development Faculty
Julius M. Gardin, MD, MBA, FACC, FACP, FAHA
− Honorarium
• Gilead Sciences
3
Copyright & Permissions
2012 SIHD Guidelines Update is Copyrighted
2013 by Practice Point Communications, unless
otherwise noted. All rights reserved.
Participants may use these slides for their
educational presentations but may not publish
or post online without permission from Practice
Point Communications, Inc.
4
Learning Objectives (CME/CNE/CPE)
At the completion of this educational activity, participants should be
able to:
− Apply diagnostic modalities in symptomatic patients with suspected
stable ischemic heart disease (SIHD) based on the
ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and
Management of Patients With Stable Ischemic Heart Disease
− Risk stratify my patients with SIHD for the probability of developing
complications based on the ACCF/AHA/ACP/AATS/PCNA/SCAI/STS
Guideline for the Diagnosis and Management of Patients With Stable
Ischemic Heart Disease
− Appropriately select optimal medical therapy and revascularization for
my patients with SIHD based on the
ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and
Management of Patients With Stable Ischemic Heart Disease
5
Spectrum of Ischemic Heart Disease:
Relevant Guidelines
Asymptomatic
(SIHD)
Asymptomatic,
Without Known
IHD
New-Onset
Chest Pain
Stable Angina or
Low-Risk UA*
(SIHD, UA/NSTEMI, STEMI)
(SIHD, PCI/CABG)
Known
IHD
(CV Risk)
Non-Cardiac
Chest Pain
Sudden Cardiac
Death
(VA-SCD)
Acute Coronary
Syndromes
(UA/NSTEMI, STEMI,
PCI/CABG)
Known
IHD
Relevant guidelines are in parentheses.
*UA: features of low-risk unstable angina include age <70 years, exertional pain lasting <20 minutes, pain not
rapidly accelerating, normal or unchanged ECG, no elevation of cardiac markers.
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
6
2012 ACCF/AHA Guideline for the
Diagnosis and Management of SIHD
Choices regarding diagnostic and therapeutic
options should be made through a process of
shared decision making
− Patient and provider
Explain
− Risks
− Benefits
− Costs
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
7
ACCF/AHA Classification of
Recommendations and Levels of Evidence
Size of Treatment Effect
Estimate of Certainty
(Precision) of
Treatment Effect
Level A
−
Multiple populations
evaluated
−
Multiple randomized
clinical trials or metaanalyses
Level B
−
Limited populations
evaluated
−
Single randomized or
non-randomized
studies
Level C
−
Very limited
populations evaluated
−
Expert consensus
opinion, case studies,
or standard of care
Class I
Class IIa
Class III
No Benefit or
Harm
Benefit >>> Risk
Benefit >> Risk
Benefit > Risk
(SHOULD be
performed/administered)
(IT IS REASONABLE to be
performed/administered Tx)
(Procedure/treatment
MAY BE CONSIDERED)
• Is useful/effective
• Sufficient
evidence
• Favors being
useful/effective
• Some conflicting
evidence
• Usefulness and
efficacy less well
• Is useful/effective
• Evidence from
single randomized
trial or nonrandomized
studies
• Favors being
useful/effective
• Some conflicting
evidence
• Usefulness or
efficacy less well
• Is useful or
effective
• Only expert
opinion, case
studies, or
standard of care
• Favors being
useful or effective
• Only diverging
expert opinion,
case studies, or
standard of care
• Usefulness or
efficacy less well
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
8
Class IIb
established
• Greater conflicting
evidence
established
• Greater conflicting
evidence
established
• Only diverging
expert opinion,
case studies, or
standard of care
• Not useful or
effective
• Some conflicting
evidence
• Not useful or
effective or may
be harmful
• Evidence from
single randomized
trial or nonrandomized
studies
• Not useful or
effective or may
be harmful
• Only expert
opinion, case
studies, or
standard of care
ACP Interpretation of ACCF/AHA SIHD
Guideline: Key Diagnostic Questions
Diagnosis
How should a clinician
evaluate a patient with
chest pain that is
consistent with IHD?
What is the role of noninvasive and angiographic
testing in the diagnosis of
SIHD?
Management
What should be the approach to
modifying cardiovascular risk
factors to reduce the mortality
and morbidity associated with
SIHD?
What is the role of coronary
revascularization in reducing
mortality and morbidity
associated with SIHD?
How should chronic anginal
symptoms be managed with
medications?
Qaseem A, et al. Ann Intern Med. 2012;157:729-734.
Qaseem A, et al. Ann Intern Med. 2012;157:735-745.
9
Diagnosis: Suspected IHD (or Change
in Clinical Status in Known IHD Patient)
Intermediate or High-Risk Unstable Angina
No
Comprehensive Clinical
Assessment of Risk
Yes
See ACCF/AHA
UA/NSTEMI Guidelines
Personal Characteristics
Coexisting Cardiac and Medical Conditions
Health Status
Symptoms or findings suggest high-risk lesion(s)?
OR
Prior sudden death or serious ventricular arrhythmia?
OR
Prior stent in unprotected left main coronary artery?
No
Continue Assessment
Initiate or continue Guideline-Directed
Medical Therapy
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
Qaseem A, et al. Ann Intern Med. 2012;157:729-734.
10
Yes
Initiate
Guideline-Directed
Medical Therapy
(consider coronary
revascularization to
improve survival)
Clinical Classification of Chest Pain
Typical angina (definite)
1. Substernal chest discomfort with a characteristic
quality and duration that is
2. Provoked by exertion or emotion and
3. Relieved by rest or nitroglycerin
Atypical angina (probable)
− Meets 2 of the characteristics of typical angina
Non-cardiac chest pain
− Meets <1 of the typical anginal characteristics
Cannon CP, et al. In: Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine. 9th Edition. 2012.
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
Qaseem A, et al. Ann Intern Med. 2012;157:729-734.
11
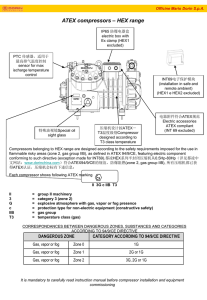
Pretest Likelihood of CAD by Cardiac Catheterization in
Symptomatic Patients (Diamond/Forrester and CASS)
Atypical
Angina
Likelihood of CAD (%)
27%
13%
2%
4% 3%
20%
14%
Likelihood of CAD (%)
100
Female
Male
Typical
Angina
100
Female
Male
80
72%
65%
60
51%
40
34%
51%
31%
22%
20
Likelihood of CAD (%)
Non-Anginal
Chest Pain
80
Female
Male 87%
76%
60
93%
94%
86%
73%
55%
40
26%
20
12%
7%
30-39 40-49 50-59 60-69
0
30-39 40-49 50-59 60-69
Age (years)
CASS: Coronary Artery Surgery Study.
Diamond GA, et al. N Engl J Med. 1979;300:1350-1358.
Chaitman BR, et al. Circulation. 1981;64:360-367.
12 Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
Age (years)
0
30-39 40-49 50-59 60-69
Age (years)
2012 ACCF/AHA Guideline Criteria for
Non-Invasive Risk Stratification
Low risk (<1% annual death or MI)
− Low-risk treadmill score (score >5) or no new ST-segment
changes or exercise-induced chest pain symptoms, when
achieving maximal levels of exercise
− Normal or small myocardial perfusion defect at rest or with
stress encumbering <5% of myocardium*
− Normal stress echocardiographic wall motion or no change of
limited resting wall motion abnormalities during stress*
− CAC <100 Agatston units
− No coronary stenosis >50% on CCTA
*Although published data are limited, patients with these findings will probably not be at low risk in the presence of
either a high-risk treadmill score or severe resting LV dysfunction (LV ejection fraction <35%).
CAC: coronary artery calcium; CCTA: coronary CT angiography.
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
13
2012 ACCF/AHA Guideline Criteria for
Non-Invasive Risk Stratification
Intermediate risk (1% to 3% annual mortality rate)
− Mild/moderate resting LV dysfunction (LVEF 35% to 49%) not readily
explained by non-coronary causes
− Resting perfusion abnormalities in 5% to 9.9% of the myocardium in
patients without a history or prior evidence of MI
− >1 mm of ST-segment depression occurring with exertional symptoms
− Stress-induced perfusion abnormalities encumbering 5% to 9.9% of the
myocardium or stress segmental scores (in multiple segments)
indicating 1 vascular territory with abnormalities but without LV dilation
− Small wall motion abnormality involving 1 to 2 segments and only 1
coronary bed
− CAC score 100 to 399 Agatston units
− 1-vessel CAD with >70% stenosis or moderate CAD stenosis (50% to
69% stenosis) in >2 arteries on CCTA
CAC: coronary artery calcium; CCTA: coronary CT angiography.
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
14
2012 ACCF/AHA Guideline Criteria for
Non-Invasive Risk Stratification
High risk (>3% annual mortality rate)
−
Severe resting LV dysfunction (LVEF <35%) not readily explained by non-coronary causes
−
Resting perfusion abnormalities >10% of the myocardium in patients without prior history or
evidence of MI
−
Stress-induced
• Stress ECG findings including >2 mm of ST-segment depression at low workload or persisting into
recovery, exercise-induced ST-segment elevation, or exercise-induced VT/VF
• Severe stress-induced LV dysfunction (peak exercise LVEF <45% or drop in LVEF with stress >10%)
• Stress-induced perfusion abnormalities encumbering >10% of myocardium or stress segmental scores
indicating multiple vascular territories with abnormalities
• Stress-induced LV dilation
• Inducible wall motion abnormality (involving >2 segments or 2 coronary beds)
• Wall motion abnormality developing at a low dose of dobutamine (<10 mg/kg/min) or at a low heart rate
(<120 beats/min)
−
CAC score >400 Agatston units
−
Multivessel obstructive CAD (>70% stenosis) or left main stenosis (>50% stenosis) on CCTA
CAC: coronary artery calcium; CCTA: coronary CT angiography.
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
15
Initial Cardiac Test for Diagnosis:
Able to Exercise*
No Contraindications
to Stress Testing
Previous Revascularization or
Resting ECG Not Interpretable
MPI or Echocardiogram
With Exercise
No Previous Revascularization
Interpretable Resting ECG
Likelihood of IHD
Low
Intermediate
Standard
Exercise ECG
Standard
Exercise ECG
I
IIb III
Intermediate
to High
MPI or
Echocardiogram
With Exercise
IIa IIb III
I
IIb III
*Suspected IHD or change in clinical status in known IHD patients.
MPI: myocardial perfusion imaging.
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
Qaseem A, et al. Ann Intern Med. 2012;157:729-734.
16
IIa IIb III
Initial Cardiac Test for Diagnosis:
Not Able to Exercise*
No Contraindications
to Stress Testing
Low
Likelihood of IHD
Intermediate-to-High
Likelihood of IHD
Pharmacologic Stress
Echocardiogram
OR
I
IIb III
Pharmacologic Stress
MPI or Echocardiogram
IIa IIb III
Pharmacologic Stress
CMR or CCTA†
I
IIb III
I
*Suspected IHD or change in clinical status in known IHD patients.
†CMR (recommendation: intermediate-to-high probability); CCTA (recommendation: intermediate probability).
MPI: myocardial perfusion imaging; CMR: cardiac magnetic resonance; CCTA: coronary CT angiography.
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
Qaseem A, et al. Ann Intern Med. 2012;157:729-734.
17
IIb III
Initial Cardiac Test for Diagnosis:
Contraindications to Stress Testing*
Contraindications
to Stress Testing
OR
CCTA
I
IIb III
Initiate GuidelineDirected Medical
Therapy
(If treatment is
unsuccessful, consider
coronary angiography
and revascularization to
improve symptoms)
*Suspected IHD or change in clinical status in known IHD patients.
CCTA: coronary CT angiography.
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
Qaseem A, et al. Ann Intern Med. 2012;157:729-734.
18
Risk Assessment in Patients With
Known SIHD
Able to Exercise
Resting ECG
Not Interpretable
Resting ECG
Interpretable
OR
OR
MPI or
Echocardiogram
With Exercise
IIa IIb III
Pharmacologic
Stress
CMR or CCTA
I
IIb III
I IIa
III
Standard
Exercise
Test
IIa IIb III
MPI or
Echocardiogram
With Exercise
I
IIb III
MPI: myocardial perfusion imaging; CMR: cardiac magnetic resonance; CCTA: coronary CT angiography.
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
Qaseem A, et al. Ann Intern Med. 2012;157:729-734.
19
Risk Assessment in Patients With
Known SIHD
Unable to
Exercise
OR
Pharmacologic Stress
MPI or Echocardiogram
IIa IIb III
Pharmacologic Stress
CMR or CCTA
I
IIb III
I
IIb III
MPI: myocardial perfusion imaging; CMR: cardiac magnetic resonance; CCTA: coronary CT angiography.
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
Qaseem A, et al. Ann Intern Med. 2012;157:729-734.
20
Risk Assessment in Patients With Known SIHD
and Special Circumstances or High-Risk Lesions
Risk Assessment Tests
Risk Assessment Tests
Special Circumstances
Standard Exercise ECG
MPI or Echocardiogram With Exercise
Pharmacologic CMR or CCTA
Pharmacologic Stress MPI or Echocardiogram
(irrespective of exercise ability)
LBBB on ECG
No
Known stenosis of
unclear significance
being considered for
revascularization
Pharmacologic
MPI or Echo
With Exercise
(I-B)
Pharmacologic
MPI, Echo,
CCTA, or CMR
(I-B)
Yes
No
Indeterminant
results from
functional testing
Non-Invasive Tests
Suggest High-Risk
Coronary Lesion
CCTA
(IIa-C)
Consider Coronary
Revascularization to
Improve Survival
No
Observe Response to
Guideline-Directed
Medical Therapy
(based on patient preferences,
anatomy, other clinical factors, and
local resources and expertise)
MPI: myocardial perfusion imaging; CMR: cardiac magnetic resonance; CCTA: coronary CT angiography.
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
Qaseem A, et al. Ann Intern Med. 2012;157:729-734.
21
ACP Interpretation of ACCF/AHA SIHD
Guideline: Key Management Questions
Diagnosis
How should a clinician
evaluate a patient with chest
pain that is consistent with
IHD?
What is the role of noninvasive testing in the
diagnosis of SIHD?
Management
What should be the approach
to modifying cardiovascular
risk factors to reduce the
mortality and morbidity
associated with SIHD?
What is the role of coronary
revascularization in reducing
mortality and morbidity
associated with SIHD?
How should chronic anginal
symptoms be managed with
medications?
Qaseem A, et al. Ann Intern Med. 2012;157:729-734.
Qaseem A, et al. Ann Intern Med. 2012;157:735-743.
22
Goals of Therapy
Minimize the likelihood of death while maximizing health
and function
− Reduce premature cardiovascular death
− Prevent complications of SIHD that directly or indirectly impair
patients’ functional well-being
• Including non-fatal AMI and heart failure
− Maintain or restore a level of activity, functional capacity, and
quality of life that is satisfactory to the patient
− Completely, or nearly completely, eliminate ischemic symptoms
− Minimize costs of health care
• Eliminate avoidable adverse effects of tests and treatments by preventing
hospital admissions, and by eliminating unnecessary tests and treatments
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
Qaseem A, et al. Ann Intern Med. 2012;157:729-734.
23
Strategies to Achieve Goals
Educate and engage patients in treatment decisions
− Etiology, clinical manifestations, treatment options, and IHD prognosis
Identify and treat conditions that contribute to, worsen, or
complicate IHD
Effectively modify risk factors for IHD
− Pharmacologic and non-pharmacologic methods
Use evidence-based pharmacological treatments to improve
patients’ health status and survival
− Avoid drug interactions and side effects
Use revascularization (PCI or CABG) when there is clear evidence of
the potential to improve patients’ health status and survival
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
Qaseem A, et al. Ann Intern Med. 2012;157:729-734.
24
PCI Versus Medical Therapy: Findings From
Studies and Systematic Reviews
PCI reduces the incidence of angina
No study has demonstrated that PCI improves
survival rates in SIHD
PCI may increase the short-term risk of MI
PCI does not lower the long-term risk of MI
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
25
COURAGE Trial: Optimal Medical
Therapy + PCI for Stable Coronary Disease
Randomization
1:1
Follow-Up: 2.5 to 7 Years
Patients (n=2287)
AHA/ACC Class I/II indications for PCI
Suitable coronary artery anatomy
>70% stenosis in >1 proximal epicardial vessel
Objective evidence of ischemia
Optimal Medical Therapy + PCI
(n=1149)
Optimal Medical Therapy
(n=1138)
(or >80% stenosis + CCS class III angina
without provocation testing)
Primary Outcome:
All-cause mortality, non-fatal MI
Secondary Outcomes:
Death, MI, stroke, ACS hospitalization
Median follow-up: 4.6 years
CCS: Canadian Cardiovascular Society; ACS: acute coronary syndrome.
Boden WE, et al. Am Heart J. 2006;151:1173-1179.
Boden WE, et al. N Engl J Med. 2007;356:1503-1516.
26
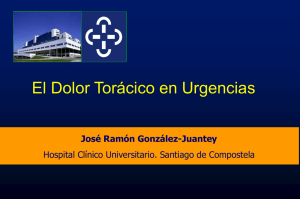
COURAGE Study:
All-Cause Mortality/Non-Fatal MI
Survival Free of Primary Outcome
Death From Any Cause and Non-Fatal MI
1
OMT + PCI
OMT
0.9
0.8
0.7
Unadjusted Hazard Ratio
1.05 (95% CI 0.87-1.27)
P=0.62
0.6
0.5
0
1
2
3
4
Follow-Up (years)
OMT: optimal medical therapy.
Boden WE, et al. N Engl J Med. 2007;356:1503-1516.
27
5
6
7
COURAGE Study:
Impact of Treatment on Angina
Angina Free
100
OMT + PCI (n=1149)
OMT (n=1138)
Patients (%)
80
74%
72%†
67%
66%*
58%
60
40
20
12%
0
13%
Baseline
1
3
Follow-Up (years)
*P<0.001 and †P=0.02 versus OMT (optimal medical therapy).
Boden WE, et al. N Engl J Med. 2007;356:1503-1516.
28
72%
5
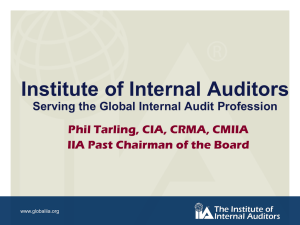
BARI 2D Study: Medical Therapy
Versus Revascularization
Primary Outcome (All-Cause Death)
CABG
PCI
100
100
89.9%
89.2%
P=0.48
60
40
Medical therapy
Revascularization
20
0
1
2
3
83.6%
P=0.33
60
40
Medical therapy
Revascularization
20
4
5
Follow-Up (Years)
BARI 2D Study Group. N Engl J Med. 2009;360:2503-2515.
29
80
Survival (%)
Survival (%)
80
0
86.4%
0
0
1
2
3
Follow-Up (Years)
4
5
CABG Versus Medical Therapy: Findings
From Studies and Systematic Reviews
Surgical techniques and medical therapy have improved
substantially over the years
− Uncertain if the relative benefits for survival and angina relief observed
several decades ago with CABG might no longer be observed
− Concurrent administration of GDMT with CABG may substantially
improve long-term outcomes compared with GDMT alone
ISCHEMIA trial (International Study of Comparative Health Effectiveness
With Medical and Invasive Approaches)
− Goal: elimination or reduction of at least moderate myocardial ischemia
• Usual care (optimal medical therapy and prompt revascularization when feasible) versus
optimal medical therapy alone with deferred revascularization when clinically indicated
(excluding left main disease detected by cardiac CT angiography)
− Outcome: hard cardiac events
− Follow-up: average 4 years (results expected in 2019)
− Patients (n=8000)
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
Available at: https://www.ischemiatrial.org/.
30
Coronary Revascularization to
Improve Survival
Clinical Setting
Method
Grade
No anatomic or physiologic criteria for revascularization
CABG or PCI
III-B HARM
1-vessel disease without proximal LAD artery involvement
CABG or PCI
III-B HARM
PCI (versus
CABG)
III-B HARM
Significant (>50%) left main coronary artery stenosis
CABG
PCI
I-B
IIa-IIb*
Significant (>70%) stenosis in 3-vessel disease with or without
proximal LAD artery disease
CABG
PCI
I-B
IIb-B
Survivors of sudden cardiac death with presumed ischemic-mediated
ventricular tachycardia caused by significant (>70%) stenosis in a
major coronary artery
CABG
PCI
I-B
I-C
2-vessel disease with proximal LAD artery disease
CABG
PCI
I-B
II-B
CABG (with LIMA)
PCI
IIa-B
IIb-B
CABG
CABG
IIa-B
IIb-B
Significant (>50%) unprotected left main CAD who have
unfavorable anatomy for PCI and are good candidates for CABG
1-vessel proximal LAD artery disease
Left ventricular dysfunction
Ejection fraction 35% to 50%
Ejection fraction <35% without significant left main CAD
31
*For certain circumstances, there are IIa and IIb (LOE B or C) indications for PCI for left main CAD.
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
Qaseem A, et al. Ann Intern Med. 2012;157:729-734.
Revascularization to Improve Persistent
Symptoms in Patients With SIHD
Persistent Symptoms Despite Adequate Trial
of Guideline-Directed Medical Therapy
Is potential revascularization warranted based on assessment of
coexisting cardiac and non-cardiac factors and patient preferences?
Yes
No
Perform
Coronary Angiography
Do results indicate that
revascularization may
improve symptoms?
Yes
Do lesions correlate with
evidence of ischemia?
Yes
Determine PCI or CABG
Guideline-Directed Medical Therapy
Continued in All Patients
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
Qaseem A, et al. Ann Intern Med. 2012;157:729-734.
32
No
No
Guideline-Directed
Medical Therapy
Coronary Revascularization to
Improve Symptoms
Significant Anatomic (>50% Left Main or >70% Non-Left Main CAD)
or Physiologic (FFR <0.80) Coronary Artery Stenosis
Clinical Setting
Method
Grade
No anatomic or physiologic criteria for revascularization
CABG or PCI
III-C
HARM
>1 significant stenosis (>70%) amenable to revascularization and
unacceptable angina despite GDMT
CABG or PCI
I-A
>1 significant stenosis (>70%) and unacceptable angina in whom
GDMT cannot be implemented (medical contraindication, adverse
events, preference)
CABG or PCI
IIa-C
Previous CABG with >1 significant stenosis (>70%) associated with
ischemia and unacceptable angina despite GDMT
PCI
CABG
IIa-C
IIa-B
Complex 3-vessel CAD (eg, SYNTAX score >22) with or without
involvement of proximal LAD artery and a good candidate for CABG
CABG preferred
over PCI
IIa-B
Viable ischemic myocardium that is perfused by coronary arteries
that are not amenable to grafting
TMR as an
adjunct to CABG
IIb-B
TMR: transmyocardial revascularization.
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
33
Guideline-Directed Medical Therapy
for Patients With SIHD
Risk factor modification
Additional medical therapy to prevent MI and
death
Medical therapy for relief of symptoms
Alternative therapies for relief of symptoms in
patients with refractory angina
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
Qaseem A, et al. Ann Intern Med. 2012;157:729-734.
34
Risk Factor Modification
Not Modifiable
Modifiable
Smoking
Gender
Hypertension
Age
Hyperlipidemia
Family history
Diabetes, glycemic control
Obesity, sedentary lifestyle
Hyperuricemia
Psychosocial factors
−
Stress, type A behavior
Medications
−
Progestins, corticosteroids
Environmental influences
−
Climate, air pollution, trace metals
in drinking water
Kones R. Vasc Health Risk Manag. 2010;6:749-774.
35
Lifestyle Modification for Patients With
SIHD: Additional Risk Factor Modification
Grade
Risk Factor
Goal
IIa IIb III
Physical
activity
Moderate-intensity aerobic activity 30-60 minutes, 7 days/week
(minimum 5 days/week)
IIa IIb III
Weight
management
Smoking
IIa IIb III
I
I IIa
I
IIb III
III
IIb III
Body mass index: 18.5 to 24.9 kg/m2
Waist circumference: men (<40 inches), women (<35 inches)
Complete cessation
No exposure to environmental tobacco smoke
Psychologic
factors
Consider screening for depression
Alcohol
consumption
Non-pregnant women: 1 drink/day (4 oz wine, 12 oz beer, 1 oz spirits)
Men: 1 to 2 drinks/day
Exposure to
air pollution
Avoid
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
36
Guideline-Directed Medical Therapy for
SIHD: Risk Factor Modification
Lipid
Management
Blood Pressure
>140/90 mm Hg
Diabetes
Management
Lifestyle modification
Dietary therapy
Lifestyle modification
Antihypertensive drug therapy
HbA1c goal: <7%†
Saturated fats: <7%
Trans fatty acids: <1%*
Cholesterol: <200 mg/dL
IIa IIb III
Moderate-to-High Dose Statin
IIa IIb III
IIa IIb III
Choice of BP medication
based on specific
patient characteristics
Initiate pharmacotherapy
to achieve goal HbA1c
I
IIb III
IIa IIb III
IIa IIb III
For Patients Intolerant to
Statins, Bile Acid Sequestrant
and/or Niacin
Rosiglitazone should
not be initiated
I IIa IIb
HARM
I
IIb III
*Percent of total calories.
†HbA
1c goal of 7% to 9% is reasonable for certain patients according to age, history of hypoglycemia, presence of
microvascular or macrovascular complications, or presence of coexisting medical conditions
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
37
Additional Medical Therapy:
Prevention of MI in Patients With SIHD
Aspirin
Beta-Blocker
No Contraindications
Aspirin 75-162 mg/day
Normal LV Function
After MI or ACS
(continue indefinitely)
Start, continue for 3 years
Renin-AngiotensinAldosterone Blocker
Hypertension, Diabetes
Mellitus, LVEF <40%, or
Chronic Kidney Disease
ACE inhibitor
IIa IIb III
IIa IIb III
Aspirin 75-162 mg/day +
clopidogrel 75 mg/day
(certain high-risk patients)
LV Systolic Dysfunction
(EF <40%) With Heart
Failure or Prior MI
Carvedilol, metoprolol
succinate, bisoprolol
I IIa
III
IIa IIb III
ARB inhibitor
(if intolerant to ACE inhibitor)
(shown to reduce risk of death)
IIa IIb III
Contraindications
II IIb III
a
Clopidogrel 75 mg/day
Other Patients With Coronary
or Vascular Disease
SIHD or Other
Vascular Disease
ACE inhibitors
IIa IIb III
I IIa
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
Qaseem A, et al. Ann Intern Med. 2012;157:729-734.
38
III
I
IIb III
Additional Medical Therapy:
Prevention of MI in Patients With SIHD
Grade
II IIb III
a
Medical Therapy
Influenza
vaccination
Estrogen therapy
I IIa IIb
Comments (Patients With SIHD)
Annually
Postmenopausal women: not recommended for reducing
cardiovascular risk or improving clinical outcomes
NO BENEFIT
I IIa IIb
NO BENEFIT
I IIa IIb
Vitamin C
Vitamin E
Beta-carotene
All patients: not recommended for reducing cardiovascular
risk or improving clinical outcomes
Folate
Vitamin B6 or B12
Elevated homocysteine: not recommended for reducing
cardiovascular risk or improving clinical outcomes
Chelation therapy
All patients: not recommended for improving symptoms or
reducing cardiovascular risk
Garlic
Coenzyme Q10
Selenium
Chromium
All patients: not recommended for improving symptoms or
reducing cardiovascular risk
NO BENEFIT
I IIa IIb
NO BENEFIT
I IIa IIb
NO BENEFIT
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
39
Guideline-Directed Medical Therapy:
Relief of Symptoms
Angina
Initial Therapy
Sublingual
Nitroglycerin or
Nitroglycerin Spray
(for immediate relief)
Beta Blocker
Contraindication
(especially if prior MI, heart
failure, or other indication)
Unacceptable
side effects
Add/Substitute
CCB and/or
Long-Acting Nitrate
Contraindication
Unacceptable
side effects
Add/Substitute
Ranolazine
I
IIa IIb III
IIa IIb III
Persistent Symptoms Despite Adequate
Trial of Guideline-Directed Medical Therapy
Consider Revascularization
to Improve Symptoms
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
Qaseem A, et al. Ann Intern Med. 2012;157:729-734.
40
IIb III
Therapeutic Targets of FDA-Approved
Agents for Myocardial Ischemia
Development
of Ischemia
Consequences
of Ischemia
Increased oxygen demand
Tachycardia
Hypertension
Preload
Contractility
Decreased oxygen supply
Ca2+ overload
Electrical instability
Myocardial dysfunction
Myocardial
Ischemia
(decreased systolic function/
increased diastolic stiffness)
Ranolazine
(reduces late Na+ current)
β-blockers
Nitrates
Calcium Channel Blockers
41
Chronic Stable Angina: Ideal Candidates for
β-Blockers and Calcium Channel Blockers
β-Blockers
Physical activity figures
prominently in anginal attacks
Coexistent hypertension
(combined α-/β-blockers)
History of
− Supraventricular arrhythmias
− Ventricular tachycardia
− Congestive heart failure
Post-MI angina or LV
dysfunction
Anxiety associated with angina
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
42
Calcium Channel Blockers
Coexistent hypertension
Contraindications/intolerance
to β-blockers
Coexisting conduction system
disease
− Except verapamil, diltiazem
Prinzmetal angina
Peripheral vascular disease
Traditional Anti-Anginal Therapy:
Conditions That May Limit Their Uses
β-Blockers
Asthma
Severe bradycardia
AV block
Severe depression
Raynaud’s syndrome
Nitrates
Severe aortic
stenosis
Hypertrophic
obstructive
cardiomyopathy
Erectile dysfunction*
Sick sinus syndrome
*Treated with PDE5 inhibitors.
†Non-dihydropyridine.
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
43
Calcium
Channel Blockers†
AV block
Bradycardia
Heart failure
LV dysfunction
Sinus node
dysfunction
Ranolazine in Chronic Stable Angina
MARISA (n=191)
CARISA (n=823)
Exercise-Limiting Angina
Ranolazine Monotherapy
Exercise-Induced Angina
Ranolazine Add-On to BB or CCB
†
Time (seconds)
550
525
Placebo
Ranolazine (bid)
500 mg
1000 mg
1500 mg
†
*
†
500
†
475
†
†
†
450
‡
‡
Placebo
Ranolazine (bid)
750 mg
1000 mg
425
Time (seconds)
575
400
375
‡
‡
350
325
450
*
300
425
400
Exercise
Duration
Onset of
Onset of
Angina ST-Segment
Depression
*P<0.005; †P<0.001, ‡P<0.05 versus placebo.
Chaitman BR, et al. J Am Coll Cardiol. 2004;43:1375-1382.
Chaitman BR, et al. JAMA. 2004;291:309-316.
44
275
Exercise
Duration
Onset of
Angina
Onset of
ECG
Ischemia
ERICA Study: Angina Frequency and
Nitrate Consumption
Nitrate Use
Angina Frequency
7
5.59
5
4
3.31
2.88*
3
2
Baseline
Week 7
Both groups received amlodipine 10 mg/day bid.
*P=0.028 and †P=0.014 versus placebo.
Stone PH, et al. J Am Coll Cardiol. 2006;48:566-575.
45
5.02
5
4.43
4
3
2.68
2.03†
2
1
1
0
Ranolazine (n=277)
Placebo (n=281)
6
5.68
Number per Week
Number per Week
6
7
Ranolazine (n=277)
Placebo (n=281)
0
Baseline
Week 7
Ranolazine Drug Interactions
Avoid using ranolazine with strong CYP3A4 inhibitors
(ketoconazole, itraconazole, clarithromycin, ritonavir,
indinavir, saquinavir, nefazodone)
Limit the dose of ranolazine to 500 mg bid with moderate
CYP3A4 inhibitors (diltiazem, verapamil, erythromycin,
fluconazole)
P-gp inhibitors (cyclosporine) may require a dose
reduction of ranolazine
Drugs transported by P-gp or metabolized by CYP2D6
(digoxin) may need a reduced dose when used in
combination with ranolazine
Ranolazine full prescribing information.
46
Alternative Therapies: Relief of Symptoms
in Patients With Refractory Angina
Grade
I IIa
III
I IIa
III
I IIa
III
Medical Therapy
Comments (Patients With Refractory Angina)
Enhanced
external
counterpulsation
May be considered an option
Transmyocardial
revascularization
May be considered an option
Spinal cord
stimulation
May be considered an option
Acupuncture
Not recommended
I IIa IIb
NO
BENEFIT
Fihn SD, et al. J Am Coll Cardiol. 2012;60:e44-e164.
47
Summary
Diagnostic and therapeutic choices in SIHD should be made through
a process of shared decision making with patient and provider
− Explain the risks, benefits, and costs
All patients with angina
− Aggressive risk factor modification and optimized medical management
must be instituted
− β-blocker is a likely first-line agent, however most patients require
multiple medications with different mechanisms of action for symptom
control
Revascularization for high-risk patients or patients with persistent
symptoms
Angina persists for many patients despite medical therapy and/or
revascularization
48