PowerPoint slides

Understanding the Hospital
Value-Based Purchasing (VBP)
Program
July, 2011
Goals of VBP Webinar
• Overview of ACA’s delivery system reforms and implications
• What is VBP, Who Participates, and What’s at Stake
• Review of the FFY 2013 VBP program
– Measures
– Data Collection Timeframes
– National Performance Standards
– VBP Scoring Methodology
– Unresolved Issues
• Look ahead to 2014 VBP program
• Questions
VBP in Context – ACA’s Mandatory Delivery
System Reforms for Hospitals
FFY 2013 FFY 2015
VBP Readmissions HACs EHR Meaningful
Use (ARRA)
• Begins October 1, 2012
(FFY 2013)
• Begins October 1, 2012
(FFY 2013)
• Redistributes inpatient payments
• Budget neutral
• Cuts Medicare inpatient payments
• $7 billion cut /10 years nationwide
• Begins October 1, 2014
(FFY 2015)
• Incentives for qualifying hospitals now
• Cuts Medicare inpatient payments
• $1.4 billion cut / 10 years nationwide.
• Cuts Medicare inpatient payments in
FFY 2015 for hospitals that do not meet
“meaningful use” standard
Implications of Mandatory Delivery System
Reforms
• Hospitals will be competing against each other
• Play or pay
VBP
• Best performers win
• Others break even or lose
Readmissions/HACs
• No winners, only losers
EHR Program
• Carrot and stick
VBP in Context – ACA’s Voluntary Delivery System
Reforms for Hospitals and Other Providers
FFY 2011 FFY 2013
Center for
Medicare/Medicaid
Innovation (CMMI)
ACO Program
• Begins January 2012
• RFPs to be released soon • Medicare FFS payments continue
• Develop test new/innovative delivery models
• $10 billion in new funding / 10 years
• Savings/losses shared by groups of providers and
CMS
Bundling Pilots
• Begin January 2013 (or sooner)
• Testing of global payment for an episode of care that may not exceed current FFS payment
• Must save Medicare program money
What is VBP?
• Established by the Affordable Care Act of 2011 (ACA)
• Transition hospitals from P4R to P4P under Medicare
• Medicare payment incentives/penalties to promote
– Achievement of high quality care
– Improvement in care quality
• Adjusts Medicare IPPS payments starting Oct. 1, 2012
(FFY 2013) based on quality performance
• Program details left to CMS
Who is Subject to the Hospital VBP Program?
• Acute care hospitals participating in the IQR Program
• Excluded hospitals:
– CAHs
– Specialty hospitals (psychiatric, rehabilitation, children’s, cancer, LTCH)
– Hospitals cited for “immediate jeopardy”
– Hospitals not participating in the IQR program
– Hospitals with small numbers of applicable measures/cases as determined by CMS
• Demos to be established for CAHs and small rural hospitals
What’s at Stake Under VBP?
• Program is self-funded by hospital “contributions”
• Contribution based on Medicare FFS payments*
– 1.0% reduction in FFY 2013
– Reduction increased by 0.25% each year
– 2.0% reduction for FFY 2017 and beyond
• VBP performance determines P4P amount
• Budget-neutral
– Redistributive
– Best performers win, others break even or lose
– VBP payments are netted against contributions
* Payment reductions exclude IME, DSH low-volume hospitals and outliers.
Updates to the VBP Program
• Continuously updated as part of annual rulemaking
• ACA requires notification of each year’s rules prior to quality data collection used for scoring
– FFY 2013 program rules established
– FFY 2014 program rules are nearly in place
– FFY 2015 program rules likely to start dropping in 2012
VBP’s Quality Measures
• Law requirements
– Must be measures reported under IQR program
– Measures must be publicly available Hospital Compare for at least one year prior to use in VBP
– CMS must publish measures and national performance standards for each measure 60 days before start of the performance measurement period
– Must categorize measures (domains)
• CMS discretion
– What measures to include/exclude
Domain
Process of Care
HCAHPS
(Patient Experience of Care)
Outcomes
(mortality/AHRQ/HACs)
Efficiency
Other TBD
Totals
(2 domains)
* Only some aspects of 2014 program are final
VBP Domains
FFY 2013 Program
Measure
Count
12
Domain
Weight
70%
Proposed FFY 2014
Program *
Measure
Count
Domain
Weight
13 20%
1
(using 8 HCAHPS
30% dimensions)
1
(using 8 HCAHPS
30% dimensions)
N/A N/A 13 30%
N/A
N/A
N/A
N/A
1
N/A
20%
N/A
(4 domains)
Process Domain Measures – FFY 2013 Program
Acute Myocardial Infarction
AMI-7a Fibrinolytic Therapy Received Within 30 Minutes of Hospital Arrival
AMI-8a Primary Percutaneous Coronary Intervention (PCI) Received Within 90 Minutes of Hospital Arrival
Heart Failure
HF-1
Pneumonia
PN-3b
Discharge Instructions
Blood Cultures Performed in the Emergency Department Prior to Initial Antibiotic Received in
Hospital
PN-6 Initial Antibiotic Selection for CAP in Immunocompetent Patient
Surgeries (as measured by Surgical Care Improvement (SCIP) measures)
SCIP-Card-2
Surgery Patients on a Beta Blocker Prior to Arrival That Received a Beta Blocker During the
Perioperative Period
SCIP-VTE-1 Surgery Patients with Recommended Venous Thromboembolism Prophylaxis Ordered
SCIP-VTE-2
Surgery Patients Who Received Appropriate Venous Thromboembolism Prophylaxis Within 24
Hours Prior to Surgery to 24 Hours After Surgery
Healthcare-Associated Infections (as measured by SCIP measures)
SCIP-Inf-1 Prophylactic Antibiotic Received Within One Hour Prior to Surgical Incision
SCIP-Inf-2
SCIP-Inf-3
SCIP-Inf-4
Prophylactic Antibiotic Selection for Surgical Patients
Prophylactic Antibiotics Discontinued Within 24 Hours After Surgery End Time
Cardiac Surgery Patients with Controlled 6 AM Postoperative Serum Glucose
HCAHPs Domain Measures – FFY 2013 Program
Patient Satisfaction Survey
HCAHPS
Eight Dimensions (using the most positive responses, “top box” responses for each question used within the HCAHPS dimension):
• Communication with Nurses
• Communication with Doctors
• Responsiveness of Hospital Staff
• Pain Management
• Communication About Medicines
• Cleanliness and Quietness of Hospital Environment
• Discharge Information
• Overall Rating of Hospital
Modifications to HCAHPS on Hospital Compare:
• “cleanliness and quietness” – combined
• “would you recommend this hospital?”- not included
VBP National Performance Standards –
FFY 2013 Program
• National Benchmarks
– Highest achievement levels
– Average performance score for the top 10% of all hospitals
• National Thresholds
– Minimum achievement levels
– Median performance score for all hospitals
• Established from baseline period data
• Vary by measure:
Measure
AMI-7a - Fibrinolytic Therapy Received Within 30
Minutes of Hospital Arrival
Benchmark Threshold
92% 65%
SCIP-Inf-1 - Prophylactic Antibiotic Received Within
One Hour Prior to Surgical Incision
100% 97%
Data Collection Timeframes – FFY 2013 Program
• Baseline Period
– Used to establish performance standards and to measure performance improvement
– July 1, 2009 – March 31, 2010 (9 months)
– Data already reported to CMS
• Performance Period
– Used to measure/calculate VBP scores
– July 1, 2011 – March 31, 2012 (9 months)
– Just started and will continue into Spring
• Applies to both Process and HCAHPS measures
Data Collection and Processing Timeframes –
FFY 2013 VBP Program
Oct.
Nov.
Dec.
Jan.
Feb.
Mar.
Apr.
May June July Aug.
Sept.
Baseline Period
[quality data from Dec. 2010 update to Hospital Compare]
FFY 2009 2008 2008 2008 2009 2009 2009 2009 2009 2009 2009 2009 2009
FFY 2010 2009 2009 2009 2010 2010 2010 2010 2010 2010 2010 2010 2010
FFY 2011 2010 2010 2010 2011 2011 2011 2011 2011 2011 2011 2011 2011
FFY 2012 2011 2011 2011 2012 2012 2012 2012 2012 2012 2012 2012 2012
Performance Period
[will reflect quality data from
Dec. 2012 update Hospital
Compare release]
FFY 2013 2012
Medicare IPPS payments
adjusted based on performance under VBP
Release of VBP final rule
[60 days prior to start of performance period as required by law]
Release of FFY 2013 IPPS final rule
[will include preliminary VBP scores, allowing CMS 4 months to process quality data reported during performance period]
VBP Scoring Methodology
• Hospital performance for each measure is compared to national performance standards
• Points are awarded for:
– Achieving high quality goals
– Improving towards high quality goals
• Maximum = 10 points / measure
• Points scored for each measure are used to calculate domain scores
• Domain scores are weighted to calculate a Total
Performance Score
Achievement
Points
(same for process and
HCAHPS measures)
VBP Scoring – FFY 2013 Program
• 10 point maximum / measure
• Performance (during performance period) compared to:
• National threshold (minimum performance level)
• National benchmark (high attainment level)
• Below the threshold = 0 points
• At or above the benchmark = 10 points
• Between threshold and benchmark = between 1 and 9 points
Improvement
Points
(same for process and
HCAHPS measures)
• 9 point maximum / measure
• Performance (during performance period) compared to:
• Prior performance (baseline period)
• National benchmark (high attainment level)
• At or below baseline period score = 0 points
• Above baseline period score = between 1 and 9
Consistency
Points
(HCAHPS only)
• 20 point maximum
• Lowest HCAHPS measure score (during performance period) compared to:
• National floor (lowest score in the country)
• National threshold (minimum performance level)
• Lowest HCAHPS score at national floor = 0 points
• Lowest HCAHPS score at or above threshold = 20 points
• Lowest HCAHPS score between floor and threshold = between 1 and 19 points
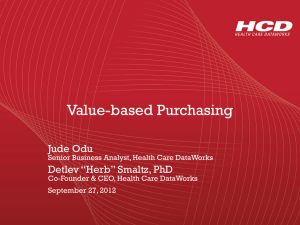
Process Score Calculation – FFY 2013 VBP Program
National - Baseline Period
Achievement
Threshold
Hospital - Baseline Period Hospital - Performance Period
Case Count
Process
Measure Score Case Count
Process
Measure Score
Achievement
Points
Improvement
Points
Final Points
(Higher of
Achievement or
Improvement
Points) Indicator
Heart Attack Patients Given
Fibrinolytic Medication Within 30
Minutes Of Arrival
Heart Attack Patients Given PCI
Within 90 Minutes Of Arrival
Heart Failure Patients Given
Discharge Instructions
Pneumonia Patients Whose Initial
Emergency Room Blood Culture
Was Performed Prior To The
Administration Of The First Hospital
Dose Of Antibiotics
Benchmark
91.91%
100.00%
100.00%
100.00%
Pneumonia Patients Given the
Most Appropriate Initial Antibiotic(s)
Surgery Patients Given Preventative
Antibiotic(s) Within One Hour
Before Surgery
Surgery Patients Given the
Appropriate Preventative
Antibiotic(s) for Surgery
Surgery Patients Whose
Preventative Antibiotic(s) Were
Stopped Within 24 Hours After
Surgery
Heart Surgery Patients Whose
Blood Sugar Was Kept Under Good
Control
Surgery Patients Whose Doctors
Ordered Treatments to Prevent
Blood Clots for Certain Types of
Surgeries
Surgery Patients Given Treatment to Prevent Blood Clots within 24
Hours Before or After Selected
Surgeries
Surgery Patients Who Were Kept on Their Beta Blockers Before and
After Surgery
99.58%
99.98%
100.00%
99.68%
99.63%
100.00%
99.85%
100.00%
65.48%
91.86%
90.77%
96.43%
92.77%
97.35%
97.66%
95.07%
94.28%
95.00%
93.07%
93.99%
0
41
254
193
129
539
549
511
59
189
189
141
Insufficient Data
100%
98%
99%
98%
100%
99%
99%
97%
95%
93%
99%
0
41
247
178
115
515
525
496
54
184
184
143
Insufficient Data Not Computed
100%
98%
98%
98%
100%
99%
99%
94%
97%
94%
98%
10
8
4
7
10
6
8
0
4
2
7
Not Computed
Does Not Apply
0
0
0
Does Not Apply
0
0
0
4
1
0
Not Computed
10
8
4
7
10
6
8
0
4
2
7
Overall Domain Score (Sum of Final Points Earned / Maximum Possible Points) 60.00%
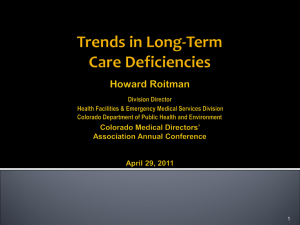
HCAHPS Score Calculations – FFY 2013 Program
National - Baseline Period
Indicator
Nurses always communicated well
Benchmark
84.70%
Achievement
Threshold
75.18%
Floor
38.98%
Hospital -
Baseline Period
Hospital -
Performance
Period
HCAHPS Measure
Score
HCAHPS Measure
Score
Consistency
Points Multiplier
Achievement
Points
75% 76% 1.00
1
Improvement
Points
Final Points
(Higher of
Achievement or
Improvement
Points)
1 1
Doctors always communicated well 88.95% 79.42% 51.51% 80% 79% 0.98
Patients always received help quickly from hospital staff
77.69% 61.82% 30.25% 64% 64% 1.00
Patients' pain was always well controlled
Staff always explained about medicines before giving them to patients
Patients' rooms and bathrooms were always kept clean and quiet
77.90%
70.42%
77.64%
68.75%
59.28%
62.80%
34.76%
29.27%
36.88%
71%
65%
68%
73%
64%
67.00%
1.00
1.00
1.00
Patients were definitely given information about what to do during their recovery at home
Patients who gave their hospital a rating of 9 or higher on a scale of 0 to 10
89.09%
82.52%
81.93%
66.02%
50.47%
29.32%
82%
69%
83%
71%
1.00
1.00
Minimum
Consistency
Points Multiplier
0.98
Overall Domain Score (Sum of Final Points Earned / Maximum Possible Points)
0
2
5
4
3
2
3
0
0
2
0
0
1
1
Consistency
Points
39.00%
0
2
5
4
3
19
3
2
Concerns with Process and HCAHPS Measures
• Process measures
– The full range of Achievement is not possible
– Minimum case size is 10
– Small hospitals may fall in and out of the program from year to year
– CMS exclusion method for “topped out” measures
• HCAHPS measures
– Bias based on region, hospital size and type
– Weight is too high
• Resulting scores are not evenly distributed, skewed low
Which Measure is Topped Out?
1,200
1,000
800
600
400
200
0
Heart Attack Patients Given ACE Inhibitor or ARB for Left Ventricular
Systolic Dysfunction (LVSD)
Score Range
2,500
2,000
1,500
1,000
500
0
Surgery Patients Who Received Preventative Antibiotic(s) One Hour Before
Incision
Score Range
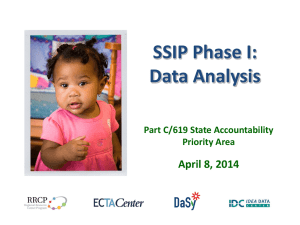
How VBP Scores Translate into Payment Adjustments
• Overall VBP score is calculated by combining domain scores
– 70% Process, 30% HCAHPS
• VBP score is entered into an equation to determine a payment percentage
• Total payments into and out of the pool must be equal
(budget neutral)
340%
320%
300%
280%
260%
240%
220%
200%
180%
160%
140%
120%
100%
80%
60%
40%
20%
0%
0%
VBP Payment Incentive Calculation
Process Domain Score:
HCAHPS Domain Score:
Overall VBP Score:
60.00%
39.00%
53.70%
CURRENT ESTIMATE - Prior to Start of
Performance Period
Payment Percentage: 174.13%
CONSERVATIVE ESTIMATE - Assumes
Scores Improve Nationally
Payment Percentage: 107.40%
Dollars Contributed to VBP
FFY 2013
1% Carve-Out
$272,000
Expected Payment from VBP $473,627
FFY 2014
1.25% Carve-Out
$340,000
FFY 2015 FFY 2016
1.5% Carve-Out 1.75% Carve-Out
$408,000 $476,000
$592,034 $710,441 $828,847
FFY 2017
2% Carve-Out
$544,000
$947,254
Net VBP Gain $201,627 $252,034 $302,441 $352,847 $403,254
Estimated Payment from VBP $292,128 $365,160
Net VBP Gain $20,128 $25,160
Payment Conversion Line
$438,192
$30,192
$511,224
$35,224
$584,256
$40,256
As more current data for the performance period become available, VBP scores are expected to improve nationwide. As scores improve, the slope of the payment conversion line will move towards the conservative estimate line.
10% 20% 30%
Payment Conversion Line - Current Estimate Using National Data
40% 50% 60%
Score
Baylor Medical Center at Irving
70% 80% 90%
Payment Conversion Line - Conservative Estimate
100%
New Measures/Domains for the FFY 2014 VBP
Program
Domain
FFY 2013 Program
Measure
Count
Domain
Weight
Proposed FFY 2014
Program *
Measure
Count
Domain
Weight
Process of Care 12 70% 13 20%
HCAHPS
(Patient Experience of Care)
1
(using 8 HCAHPS
30% dimensions)
1
(using 8 HCAHPS
30% dimensions)
Outcomes
(mortality/AHRQ/HACs)
Efficiency
Other TBD
N/A
N/A
N/A
Totals
(2 domains)
* Only some aspects of 2014 program are final
N/A
N/A
N/A
13
1
N/A
(4 domains)
30%
20%
N/A
Outcomes Domain Measures – FFY 2014 Program
Mortality Measures
Mort-30-AMI AMI 30-day mortality (Medicare patients)
Mort-30-HF HF 30-day mortality (Medicare patients)
Mort-30-PN PN 30-day mortality (Medicare patients)
AHRQ Composite Measures
AHRQ Complication/patient safety for selected indicators (composite)
AHRQ
HAC Measures
Mortality for selected medical conditions (composite)
HACs
• Foreign Object Retained After Surgery
• Air Embolism
• Blood Incompatibility
• Pressure Ulcer Stages III & IV
• Falls and Trauma
(includes fracture, dislocation, intracranial injury, crushing injury, burn, electric shock)
• Vascular Catheter-Associated Infections
• Catheter-Associated Urinary Tract Infection (UTI)
• Manifestations of Poor Glycemic Control
Concerns with Outcomes Measures
•
Mortality measures
– Rates are tightly distributed
– Size matters (i.e., law of small numbers)
– What will a “survival rate” measure do for public perception?
– Rates cannot be duplicated/checked
•
HAC measures
– The ACA already mandates a separate payment penalty
– Law of small numbers
Proposed Efficiency Domain Measure – FFY
2014 Program
• Medicare Spending per Beneficiary
– ACA requires use of efficiency measures in FFY 2014 or thereafter
– Must include total Part A and Part B spending per beneficiary
– Must include Medicare spending per beneficiary adjusted for age, sex, race, severity, and other factors as determined by the
Secretary
– CMS is also considering measures of hospital internal efficiency
Proposed Efficiency Measure
One Episode
Three Days Prior:
Pre-op lab work
Dr.
Visit
Inpatient Stay
Ninety Days
Post:
Dr.
Visit
Dr.
Visit
Rehab
ED
Visit
Dr.
Visit
Proposed Efficiency Measure
Average Payment per Episode
Concerns with Proposed Efficiency Measure
• Does proposal satisfy ACA mandate for a measure of
“spending per beneficiary”?
• Holds hospitals accountable for all providers’ practice patterns
• Should consider future IOM report and proposal for
Medicare bundling demonstrations
• Methodology cannot be replicated
– No-one can check/audit CMS’ calculations
– Industry does not have access to the data
Data Collection Timeframes – FFY 2014 Program
• Process of Care and Patient Experience of Care Domains *
– Baseline Period: April 1, 2010 through December 31, 2010 (9-months)
– Performance Period: April 1, 2012 through December 31, 2012 (9-months)
• Outcomes Domain – Mortality Measures
– Baseline Period: July 1, 2009 through June 30, 2010 (12-months)
– Performance Period: July 1, 2011 through June 30, 2012 (12-months)
• Outcomes Domain – AHRQ composite and HAC Measures *
– Baseline Period: March 3, 2010 through September 30, 2010 (7-months)
– Performance Period: March 3, 2012 through September 30, 2012 (7-months)
• Efficiency Domain *
– Baseline Period: May 15, 2010 through 90 days prior to February 14, 2011 (9-months)
– Performance Period: May 15, 2012 through February 14, 2013 (9-months)
* Proposed
National Performance Standards and Scoring
Methodology – FFY 2014 Program
• Same or similar to methods used for process and
HCAHPS measures under FFY 2013 program
• Variations to accommodate
– Efficiency measure
– HAC measures
• Adopted and proposed national performance standards for 2014 program have been published
– CY 2012 OPPS proposed rule, Federal Register pages
42,359 - 42,362
Resources
•
Contact your State Hospital Association
• VBP final rule
(includes FFY 2013 and FFY 2014 VBP policies)
– http://www.gpo.gov/fdsys/pkg/FR-2011-05-06/pdf/2011-10568.pdf
• FFY 2012 IPPS proposed rule
(includes FFY 2014 VBP polices)
– http://www.cms.gov/AcuteInpatientPPS/IPPS2012/
• CY 2012 OPPS proposed rule
(includes FFY 2014 VBP policies)
– http://www.gpo.gov/fdsys/pkg/FR-2011-07-18/pdf/2011-16949.pdf