ACRIN 6657 Extension Trial
advertisement

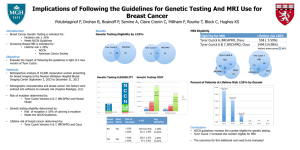
ACRIN Breast Committee Fall Meeting 2010 6657 Extension-CONTRAST-ENHANCED BREAST MRI and MRS FOR EVALUATION OF PATIENTS UNDERGOING NEOADJUVANT TREATMENT FOR LOCALLY ADVANCED BREAST CANCER Nola Hylton ,PhD Constantine Gatsonis, PhD Pat Bolan, PhD 6657 Trial Team ACRIN Breast Committee ACRIN 6657 Trial Extension Clinical Study Anthracycline MRI/MRS Taxane Surgery MRI/MRS MRI/MRS Core biopsy • Both CALGB 150007 and ACRIN 6657 were amended and re-opened in September 2007; additional target accrual of 140 patients • Same treatment paradigm as in original trials • ACRIN 6657 amended to add single voxel 1H MR spectroscopy to the imaging protocol; testing MRS [choline] as a marker of early response • Short term endpoint used (pCR) ACRIN Breast Committee 6657 Extension Aims • New aims are testing total choline concentration [tCho] measured by single voxel 1H MR spectroscopy following 1 cycle of chemotherapy for distinguishing responsive and non-responsive tumors. Includes: Reproducibility testing 1.5 T versus 3.0 T comparison Acute (20-28 hour) versus persistent (48-96 hours) post treatment time point comparison ACRIN Breast Committee 6657 Extension Aims • Accrual to-date: 114 patients accrued 96 enrolled at 1.5 T 16 enrolled at 3.0 T 44 enrolled at 20-28 hr 26 enrolled at 48-96 hr 28 enrolled outside of protocol time points 14 – time point data missing • Analysis to-date ACRIN Breast Committee Quality Control Phantom Scans Design (ISMRM 2008 poster) • Standard phantoms • Entry and Weekly scanning Motivation • Set entry threshold • Monitor site consistency • Acquire data for retrospective analysis - measurement precision (SE) - compare fitting methods - detection thresholds - identify technical problems ACRIN Breast Committee 2 liter bottle Vegetable oil 40 mm ø sphere w/ 1 mM PCho 20 mm voxel ACRIN Breast Committee Subject MRS Data Status withdrew / ineligible (9) acquisition error (7) Pending Data (13) • 112 subjects as of 9/15 • Status is per-subject no cho (20) • both MR1 and MR2 must be good • No cho: Pending Analysis (9) • low snr (1.5T), difficult voxel placements, too fatty no data acquired / submitted (22) Good (32) ACRIN Breast Committee • No data • Some lost • Some not acq’d: why? Example: Good quality ACRIN Breast Committee Example: No choline ACRIN Breast Committee Example: Acquisition error ACRIN Breast Committee Example: Analysis Pending Choline peak is over-fit ACRIN Breast Committee MRS Data Quality, per-subject by Quartile 100% 90% 80% 70% 60% no choline 50% acq. error 40% Good 30% 20% 10% 0% Q1 ACRIN Breast Committee Q2 Q3 Q4 MRS Data by Field Strength 1.5T 3T 96 (86%) 16 (14%) Good data rate 48% 89% Acq. error rate 14% 0% No choline rate 38% 11% # subjects ACRIN Breast Committee 6657 MRS Summary Accrual ongoing Early termination? • Competing with ISPY2 • Stopping pt analysis: • need 43 subjects with a drop in [tCho] and final path • have 14 responders, 9 non-responders by [tCho] with path MRS Analysis work • Better fitting (SVD, magnitude fitting, detection thresholds) • Voxel placement grading ACRIN Breast Committee ACRIN Breast Committee Fall Meeting 2010 6693 MR Imaging Biomarkers for Assessment of Breast Cancer Response to Neoadjuvant Treatment Nola Hylton ,PhD Mark Rosen, MD, PhD Eunhee Kim, PhD Pat Bolan, PhD Savannah Partridge, PhD 6657 Trial Team ACRIN Breast Committee ISPY-2 Adaptive Trial Design AC (4 cycles) Paclitaxel * (12 weekly cycles) Screening R A N D O M I Z E O N S T U D Y MRI Biopsy Blood Draw MUGA/ECHO CT/PET Paclitaxel* + Investigational Agent A (12 weekly cycles) AC (4 cycles) Paclitaxel* + Investigational Agent B (12 weekly cycles) AC (4 cycles) MRI Biopsy Blood Draw Consent #2 Treatment Consent MRI Blood Draw S U R G E R Y MRI Blood Draw * HER2 positive participants will also receive Trastuzumab. An investigational agent may be used instead of Trastuzumab. • Target accrual: 800 patients over 4 years, 20 sites • ISPY-2 opened in March 2010; 4 sites open (~15 patients enrolled) ACRIN Breast Committee Tissue Overall Objective for ACRIN 6693 • Evaluate tumor apparent diffusion coefficient (ADC), alone and in combination with SER as a marker of early response • Multi-parametric MRI biomarkers will be evaluated in the setting of the ISPY-2 adaptive neoadjuvant breast cancer trial testing targeted agents in combination with paclitaxel ACRIN Breast Committee Diffusion-Weighted MRI (DWI) • Measures the mobility of water diffusing in tissue • Sensitive to restriction of water motion – cell density/cellularity – membrane integrity, microstructure • Reduced diffusion in tumors • Sensitive to cell death and necrosis associated with response to treatment ACRIN Breast Committee Cancer Imaging. 2006; 6(1): 135–143. DWI Studies in ACRIN 6657 • DWI optional in 6657 • DWI data collected: – Original 6657: 16 cases with visit 1 and 2 – Extension: 26 cases with visit 1 and 2 • Sample sizes too small for meaningful analysis – original and extension treated separately because of differing visit 2 timepoints ACRIN Breast Committee Prior Breast DWI Studies • ADC increases over the course of neoadjuvant chemotherapy in breast tumors [1, 2] • ADC change occurs earlier than changes in size (volume or LD) [1,2] • Predictive value of ADC – Baseline ADC lower in clinical responders [3] – Change in ADC significantly greater in responders [2,3] 1. 2. 3. Pickles et al. Magn Reson Img 2006; 24:843–847. Sharma et al. NMR Biomed 2008; 22(1):104-13. Iacconi et al. Eur Radiol 2010; 20(2):303-8. ACRIN Breast Committee Recent Findings UW/SCCA • 17 patients with invasive breast cancer • Neoadjuvant treatment – Metronomic - weekly doxorubicin/daily cyclophosphamide followed by paclitaxel • Imaged with DWI – Prior to treatment, mid-, post-treatment DCE ACRIN Breast Committee DWI ADC Recent Findings UW/SCCA • Significant increases in ADC observed over the course of chemotherapy (p<0.05, pre-post) Pre-treatment • Serial tumor ADC histograms in a responding patient Mid-treatment Post-treatment ADC (x10-3mm2/s) ACRIN Breast Committee Recent Findings UW/SCCA • Baseline ADCmin lower in • Change in ADCmin midpCR patients (p=0.038) treatment greater in pCR patients (p=0.044) Change in ADCmin Baseline ADCmin by Path Response 0.6 1 0.4 0.4 * 0.2 * 0.2 mm2/s) 0.6 ADC (x10-3 1.2 0.8 ADC 0.8 0 0 1 -0.4 0 ADCminResidual pre pCR Disease -0.6 Treatment Timepoint Presented at the ISMRM Workshop on Improving Cancer Treatment with Advanced MR, Santa Cruz, CA, Sept. 20, 2010. ACRIN Breast Committee 2 pCR Residual -0.2 Status of ACRIN 6693 • approved by ACRIN Steering Committee – Sept 2009 • Protocol submitted to CTEP – June 2010 • Protocol concept disapproved by CTEP – August 2010 • Revisions and re-submission planned – November 2010 – More clearly defined objectives for evaluating ADC, integration with ISPY-2, results from ISPY-1 ACRIN Breast Committee