Lung Volume Reduction Surgery
advertisement

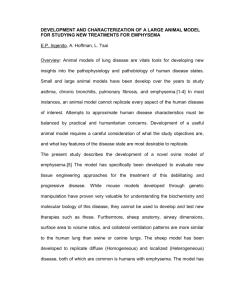
Current Concepts in Lung Volume Reduction November 18, 2013 James Canfield MBA/RPFT Interventional Pulmonary Service Emphysema • Emphysema, along with chronic bronchitis, together are referred to as Chronic Obstructive Lung Disease • Characterized by increase beyond normal in the size of air spaces distal to the terminal bronchiole containing alveoli • Destructive changes in their walls and reduction in their number • "Heterogeneous" and "homogenous“ - Heterogeneous is when emphysema is more isolated to certain areas of the lungs and the extent of emphysema varies between segments of the lungs. - Homogenous is when emphysema has a more diffuse pattern and it is distributed more evenly throughout the lungs Morphological Types of Emphysema • Centriacinar - Begins in the respiratory bronchioles and spreads peripherally - Also termed centrilobular emphysema - Associated with long-standing cigarette smoking - Predominantly involves the upper half of the lungs. • Panacinar - Destroys the entire alveolus uniformly - Predominant in the lower half of the lungs - Generally observed in patients with homozygous alpha1-antitrypsin (AAT) deficiency • Paraseptal - Preferentially involves the distal airway structures, alveolar ducts, and alveolar sacs - Localized around the septae of the lungs or pleura - Apical bullae may lead to spontaneous pneumothorax 3 Emphysema Clinical Manifestation • Breathlessness on exertion - Reduction of alveolar surface for gas exchange - Collapse of smaller airways with trapping of alveolar gas in expiration • Causes the chest to be held in the position of inspiration • Prolonged expiration and increased residual volume 4 Possible Complications of Emphysema • Pneumothorax - Can be fatal in patients with severe emphysema because the lungs have become so weak • Cor pulmonale - Happens when pressure in the arteries that connect the lungs and heart increases • Giant bullae - Sometimes half the size of the lung - Lungs have a much smaller surface area - The bullae can become infected - More likely to develop pneumothorax • Recurring infections - Chest infections, pneumonia, influenza, cold and the common cold are like to occur more often • Pulmonary hypertension 5 Lung Volume Reduction Surgery • Many people who suffer with emphysema have portions of the lung which are more affected than others • This finding led to the development of a surgical approach to treat emphysema - Lung volume reduction surgery (LVRS) is a procedure which removes approximately 20-35% of the poorly functioning, space occupying lung tissue from each lung - By reducing the lung size, the remaining lung and surrounding muscles (intercostals and diaphragm) are able to work more efficiently • This makes breathing easier and helps patients achieve greater quality of life 6 Lung Volume Reduction Surgery • Good Candidates - Has stopped smoking for at least 4 months - Has disabling emphysema despite complete compliance with optimum medical therapy - Must be able to participate in a pulmonary rehabilitation program prior to and after surgery - Other medical conditions must be well controlled and must not present unacceptable risks for complications from the procedure - Must have a pattern of emphysema that is amenable to surgical management • There are space occupying, poorly functioning areas of the lung which can be removed to improve lung function - Chest x-ray, CAT scan, and lung perfusion studies 7 Lung Volume Reduction Surgery • The National Emphysema Treatment Trial (NETT) - Group 1: Patients with predominantly upper lobe emphysema and low exercise capacity • Have improved survival and functional outcomes after LVRS compared to medical therapy. - Group 2: Patients with predominantly upper lobe emphysema and high exercise capacity • Have improved functional outcomes after LVRS but no difference in survival compared to medical therapy. - Group 3: Patients with non-upper lobe emphysema and low exercise capacity • Have improved survival after LVRS but no difference in survival compared to medical therapy. 8 Lung Volume Reduction Surgery • Anticipated Benefits - As overall hyperinflation decreases, diaphragm and chest wall mechanics would improve and WOB would decrease - Increase in elastic recoil thereby restoring the outward pull on bronchioles and increase expiratory flow - Increase flow would decrease dynamic hyperinflation - Improvement in ventilation and profusion matching improves alveolar gas exchange which in turn may decrease need for supplemental oxygen thoracicsurgery.stanford.edu 9 Lung Volume Reduction Surgery thoracicsurgery.stanford.edu 10 Lung Volume Reduction Surgery • Poor Candidates - Patients with non-upper lobe emphysema and high exercise capacity. - Patients with extremely poor pulmonary function (FEV1 20% or less than predicted) and either homogenous distribution of emphysema on CT scan or extremely poor carbon monoxide diffusing capacity (DLCO 20% or less than predicted). 11 Potential Complications • Prolonged air leakage is the most common complication after LVRS, Air leaks with a median 7-day duration have also been reported in 90% of patients • Intraoperative complications (9%) • Postoperative complications (50%) - Pneumonia (18.2%) can occur in emphysema patients, especially in patients who have a history of recurrent bouts - Reintubation (21.8%) - Arrthymias (18.6%) - Bleeding (2-5%) - Death: The chance of dying after LVRS is approximately 3-8% Lessons learned from the National Emphysema Treatment Trial. Ann Thorac Surg 82:197-207, 2006 12 Bronchoscopic Lung Volume Reduction (bLVR) LVRS application is limited by high postoperative morbidity and stringent selection criteria that effectively exclude many patients. This has been the impetus for the development of less-invasive approaches to lung volume reduction In the last decade bronchoscopic approaches have been developed to reproduce the effects of LVRS: • Valves that allow unidirectional airflow in exhalation to collapse target lung lobe • Biological lung volume reduction with biodegradable gel into bronchi • Creation of airway bypass tracts • Coils • Thermal vapor ablation 13 Rationale for bLVR • Use of endoscopic methods to collapse of hyperinflation would have the beneficial effects similar to resecting these areas without the morbidity of surgery • Patients not a good surgical candidates might be able to undergo bLVR 14 Active Randomized Clinical Trials of Bronchoscopic Lung Volume Reduction FDA-Approved TRIALS ASPIRE RENEW LIBERATE LVR Coil EBV, Chartis Device(s) Aeriseal Sample Size 300 315 183 Randomization Schema 3:2 1:1 2:1 Treatment Bilateral Bilateral-staged Unilateral Primary Endpoint FEV1 6-minute walk FEV1 Sponsor Aeris PneumRx Pulmonx (foam) Therapeutics 15 Bronchoscopic Lung Volume Reduction • Bronchial Valves - The intrabronchial valve (Spiration Inc., Redmond, WA, USA) has six struts made of nitinol covered by polyurethane membrane in the shape of an umbrella Thorac Surg Clin 19:247-253, 2009 16 Bronchoscpic Lung Volume Reduction • The Zephyr endobronchial valve (Pulmonx Inc., Palo Alto, CA, USA) is a one way valve that is mounted on a self-expanding nitinol stent. The endobronchial valve (EBV) allows unidirectional airflow mucus clearance in expiration and is available in various sizes N Engl J Med 363:1233-1244, 2010 17 The RePneu® LVRC • A minimally invasive medical implant designed to treat the symptoms of severe emphysema • Unlike Lung Volume Reduction Surgery, the RePneu LVRC is intended to treat a broad range of emphysema patients • Is designed to reduce lung volume and restore elastic recoil to improve lung function, exercise capacity, and quality of life for patients with emphysema • Made from shape-memory Nitinol • The Coils are straightened for insertion into your airways, and then reform their coiled shape once they are released from the bronchoscope, gently compressing the surrounding diseased lung tissue and tethering the small airways open 18 The RePneu® LVRC 19 The RePneu® LVRC 20 The RePneu® LVRC 21 RENEW • This Study is a randomized, controlled study in which half of the patients (Coil group) will receive LVRC. Half of the patients will not receive Coils (Control group) • All participants will continue to receive Standard Medical Care and will be followed by the study staff for 12 months • Up to 315 patients will participate in this study. The study will be conducted in over 25 medical centers across North America, with a smaller number of sites in Europe 22 The RePneu® LVRC 23 EL CAMINO HOSPITAL INTERVENTIONAL PULMONARY SERVICE 24 25