New Incentive Approaches For Adherence
advertisement

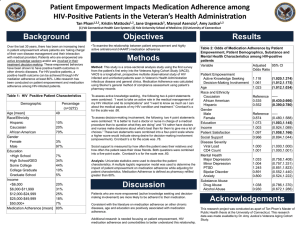
New Incentive Approaches to Adherence Stephen Kimmel, MD, MSCE Andrea Troxel, ScD Center for Clinical Epidemiology and Biostatistics The Importance of Clinical Trials to Study Adherence Interventions • Observational studies prone to bias – Patient selection – Temporal trends – Unmeasured confounders • Effects of intervention may not be “symmetrical” – e.g., increasing copayments for medications may not have the same effect as reducing copayments • Logistics – You can learn a lot just from developing an intervention Adherence worsens among those facing copayment increases…but also among patients without copays Source: Doshi, Zhu, Kimmel, Volpp et al. Circulation Reducing co-pays appears to have modest effects in quasi-experimental studies Source: Chernew ME, et al. Health Affairs 2008;27(1):103-12. $5 $0 for generics $25 $12.50 for preferred drugs, $45 22.50 for non-preferred drugs 4 But, Randomized Trial of Copay Reduction: No Impact. . . •RCT among veterans with poorly controlled blood pressure •Average SBP on study entry: 160 •Copayments reduced from $8 per month to $0 • No significant effect on blood pressure or medication adherence in either study Source: Volpp, Troxel, Kimmel , Doshi et al. 2010 Novel Approaches to Adherence • Framework: Behavioral Economics • Most commonly used approaches – Financial incentives • patients • clinicians – Reminders – Pre-commitment mechanisms Adherence to Warfarin % Population 40% of patients were >20% non-adherent Either missed or extra dose Underadherence by Under-AC Odds Ratio (CI) P<0.0001 % Missed Pills Reference group: No missed pills Kimmel et al. Arch Intern Med. 2007;167:229-235. Adherence Changes Over Time Percent of Days Non-Adherent 30% 20% 10% 0% 1 3 6 9 Month After Beginning Warfarin Use 12 Lottery-Based Incentives: Conceptual Framework • Deliver frequent feedback and rewards – ideally at the daily level, because of present-biased preferences • Lotteries give more bang for the buck, in part because people overweight small probabilities • Give frequent positive feedback plus the hope of big payout – Take advantage of time discounting – Use variable reinforcement • Utilize regret as a motivator Lottery-based financial incentive based on daily medication use • Eligible for daily lottery prize if the medication monitoring device has registered that patient took medication the previous day • If patient did not take medication s/he will be informed that s/he would have won the lottery that day had s/he taken the medication properly • High probability small reward & low probability big reward • Takes advantage of present-biased preferences (immediacy of receiving coupon/gift card), overestimation of probabilities, regret aversion, and variable reinforcement Incentives for medication adherence using daily lotteries – Warfarin is an anti-stroke medication with large benefits but non-adherence rates high (chronic, asymptomatic condition) – Designed lottery with 1 in 5 chance of winning $10 a day, 1 in 100 chance of winning $100 each day IF took warfarin previous day Volpp, Loewenstein, Troxel, Doshi & Kimmel, BMC Health Services Research, 2008 12 The Warfarin INcentives (WIN) Pilot Trial P<0.001 P=0.4 P-value for interaction=0.0016 WIN2 Trial WIN2 Trial Design • Balanced randomization, stratified by – Baseline INR status – Study site • Five comparisons of interest – Each active arm against control (3) – Combined arm against each single arm (2) – Bonferroni adjustment of alpha = 0.01 WIN2 Power/Sample Size • Binary outcome: out-of-range (OOR) INR • Detect a 30% reduction in occurrence of OOR INRs from 0.43 to 0.3 – Assume 10% drop-out by six months – Assume ICC of 0.05 – Assume 7 INR assessments per subject WIN2 Analysis Plan • Generalized linear mixed models – Logit link – Fixed effects for time, treatment, other timeinvariant covariates – Random intercepts and slopes – Exploratory modeling of shape of time effect – Time x treatment interactions – Explore adjustment for frequency of assessment Segmenting or Tailoring • How can we improve effectiveness (and costeffectiveness) of these interventions? • Should we (can we) only target non-adherent patients? • Can we tailor our interventions? - Upfront screening of RCT patients at baseline for reason for non-adherence with tailored intervention - Sequential Multiple Assignment Randomized Trials (SMART) Tailoring • Evaluate subjects at baseline regarding drivers of non-adherence (cost, distraction/forgetfulness, knowledge/beliefs/attitudes) • Develop strategy tailored to each driver (copay reduction, lottery-based reminder, education/instruction) • Consider randomizing “tailored strategy” vs “onesize-fits-all strategy” vs “usual care” SMART Designs Sequential Multiple Assignment Randomized Trials • Work by Murphy, Robins, Thall, and many others • Optimize response by varying interventions on the basis of time-dependent information - In cancer therapy, randomize patients to initial therapy; then randomize responders to maintenance therapy and non-responders to second-line therapy - In adherence, randomize subjects to primary strategy; then maintain adherent subjects on same strategy and randomize non-adherent subjects to remaining options Summary • Use ideas from behavioral economics to inform interventions • Use appropriate methodology from clinical trials to properly assess hypotheses of interest • Promising area for further development of adaptive treatment and tailoring strategies • LDI Center for Health Incentives (Kevin Volpp, Director) is leading multiple trials in diverse areas of behavioral health