(FIB) - Why Develop a Competency Program for Nurses?
advertisement
 - Why Develop a Competency Program for Nurses?")
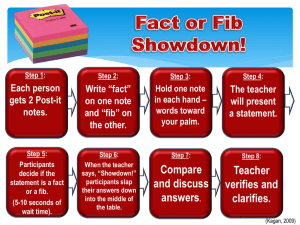
Fascia Iliaca Block (FIB) - Why Develop a Competency Programme for Nurses? Background Dr A Blackburn – Pain Nurse Specialist, Dr MK Varma – Consultant Anaesthetist Dr H Dawson – Consultant Anaesthetist Royal Victoria Infirmary, Newcastle upon Tyne Approximately 550 patients are admitted per year to our hospital with #NOF; the incidence is expected to rise along with the attendant costs to acute and on-going care. Unrelieved pain not only has physiological consequences with significant effects on mortality and morbidity but is unacceptable due to humanitarian reasons. Patients admitted with # neck of femur (NOF) are typically elderly and frail with multiple co-morbidities. There is usually a history of trauma, and generally the fracture is displaced and unstable and can cause considerable pain. The Next Phase Audit revealed that at best 50% of this patient group received the desired block. Having identified the advantage of using FIC, it became apparent that we needed to train additional practitioners to perform a regional block. Registered anaesthetic / recovery nurses and ODPs were chosen. Baseline audits: Review basic analgesia Review administration Introduce FIB Why anaesthetic / recovery Teams? Audit FIB trials Development of protocol Still only targeting 50% of potential patients An audit in 2007 identified that patients admitted with #NOF experienced severe pain pre-op and 6-12hrs post-op when the local anaesthetic block given at the time of surgery wore off. Only half had morphine prescribed, and less than a third received morphine post-op. A further audit in 2009 revealed that severe pain was again experienced pre-op and at 12 hours post-op. All analgesic groups were prescribed, but again only one third of patients received morphine. Our experience shows that #NOF causes significant pain which can be difficult to manage in this group of patients. Opioid use and under-treated pain have been shown to increase the incidence of delirium 1 and slow postoperative mobilisation and recovery 2. The safety and utility of regional nerve blocks for the relief of trauma and postoperative pain is very well established and validated in medical practice. An appropriate, safe and easily executed nerve block for #NOF is FIB. There is good evidence that FIB results in fast, effective analgesia and significantly reduces the cumulative doses of opioids in patients with #NOF 3,4,5,6. Introduction of Fascia Iliaca Catheter (FIC) Identify need for nursing role development: Competency assessment agreed PGDs approved FIC was trialled Nov 2011 – Apr 2012, and demonstrated improved comfort without impact on post-operative management. Opioid consumption decreased. Nursing staff expressed greater ease with performing cares. However there was variability in offering the service due to the limited number of clinicians who could perform the block. Audit identified that despite intensive education, inclusion of FIC on the fast track pathway of #NOF management, and an increased number of clinicians available to perform the block we still only targeted 50% of patients admitted with #NOF. Nurses have been performing FIB for a number of years, traditionally pain nurse specialists on wards. However we elected to develop an alternative service using anaesthetic / recovery teams because they are available 24/7 and can provide a service to all patients admitted with #NOF. Importantly they can be trained and supervised by experienced anaesthetists. Selection of nurses 2 yrs post-reg experience Working in anaesthetic/recovery minimum 6mth 5 per intake Educational sessions provided 10 supervised blocks culminating in competency A course of educational sessions was developed, culminating in a practical session of ultrasound use and U/S guided block in fresh cadavers. The nurses/ODPs are expected to undertake 10 supervised blocks, and after this time if competency is achieved they are permitted to perform FIB unsupervised. Revised #neck of femur protocol Fast-track from A&E via block room A comprehensive protocol standardises management of this patient group. the expected Re-audit analgesia use and pain scores of patients admitted with #NOF Outcomes Successful introduction of the programme Growing pool of expertise Improved pain scores Standardised approach to FIB Ultrasound guidance to increase efficacy of FIB Growing pool of competent staff to provide 24/7 cover, currently targeting more than 50% of #NOF population The NOF fast-track from A&E to ward includes referral to the block room for FIB ideally within 2 hours of admission. Future Work Comprehensive educational package Improved analgesia for frail elderly group, avoiding opioids Role Development A competency based assessment was developed by the consultant anaesthetists and the acute pain service, incorporating knowledge of consent, technique, the drugs used and PGDs, plus professional approach. Key Points FIB included in #NOF fast-track FIB as a single shot technique has been endorsed by the AAGBI 9 for delivery by non-medical healthcare practitioners. The technique involves the introduction of a regional block needle in the upper thigh under ultrasound guidance and subsequent injection of local anaesthetic solution in the fascia iliaca plane to anaesthetise the femoral and adjacent nerves which supply the hip joint. Analgesic effect from a single injection usually lasts between 8 to 12 hours, but may be present for up to 24 hours10. FIB is simple, fast acting, reliable and safe as the position of the injection site is at a distance from the femoral artery. Ultrasound guidance improves the target and efficacy of FIB. Approval was granted by the role development group within the Trust. References 1. Morrison et al, Relationship between pain and opioid analgesics on the development of delirium following hip fracture. Journal of Gerontology, 2003, Vol. 58A, No. 1, 76-81. 2. Morrison et al, The impact of post-operative pain on outcomes following hip fracture. Pain, 2003, 103, 30311. 3. Finlayson & Underhill, Femoral nerve block for analgesia in fractures of the femoral neck. Archives of Emergency Medicine, 1988, 5, 173-6. 4. Haddad & Williams, Femoral nerve block in extracapsular femoral neck fractures. The Journal of Bone and Joint Surgery, Nov 1995, Vol. 77-B, No.6, 922-3. 5. Fletcher, Rigby & Heyes, Three-in-one femoral nerve block as analgesia for fractured neck of femur in the emergency department: A randomized, controlled trial. Annals of Emergency Medicine, Feb 2003, 41:2, 22733. 6. Kullenberg et al, Femoral nerve block as pain relief in hip fracture. A good alternative in perioperative treatment proved by a prospective study. Lakartidningen, June 2004, Vol. 101, No. 24, 2104-7. 7. AAGBI RA-UK Fascia iliaca blocks & non-physician practitioners position statement 2013. 8. British National Formulary (2014) BMJ Group, London Successful introduction of competency based assessment Providing a nurse led service will deliver a high standard of care to patients as expertise can be developed and accumulated. The presence of a dedicated group of staff will be able to prioritise the administration of FIBs – single shot technique not catheter placement, and the net result will be more patients receiving effective analgesia. Why FIB? A hip fracture fast-track proforma was developed which included initiation of analgesia and referral for FIC whilst in A&E. National Hip fracture Database report (2013)7 in response to NICE guidance (2011) 8 quality standard 16 advocates prompt and effective pain management. A protocol was developed advocating the pre-operative placement of a catheter within a few hours of admission by the on-call anaesthetic team, and 12hrly injection of levobupivacaine by the acute pain service/ on-call team. This could be continued post-op if deemed appropriate by the anaesthetist. Traditionally nerve blocks are performed by doctors in anaesthesia or A&E. The majority of patients with #NOF are admitted out of hours. Trainee doctors who invariably would perform this procedure are transient in the hospital, and the time and resources required to train and monitor such a group is a sizeable undertaking and not always feasible. The A&E doctors or on-call anaesthetists have duties which take priority over what can be a time consuming technique, and frequently are not available at the time of admission. Re-audit Jan 2015 One year after 1st cohort Audit outcomes and satisfaction of competency based programme Continue to roll out programme, and develop round the clock provision of FIB, ultimately targeting 100% of #NOF population Review time from admission to block, duration of FIB, and if further block required. Consider the need to develop the role further to include catheter placement