A3 Training Resnick Neuropsychiatric Hospital
advertisement

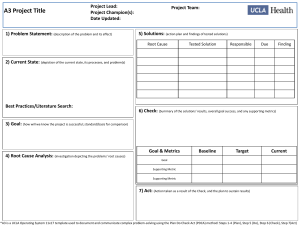
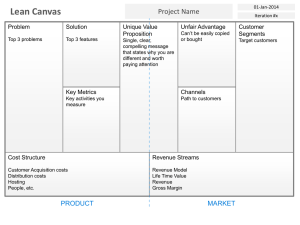
A3 Training DGSOM BEI HR Sphere 1 Agenda Topic • • • Intro to Lean Project Charter Plan • • • • Duration 10 min 5 min 45 min Clarify the Problem Analyze the Current State Develop Goals Analyze Root Causes Total: 60 min Learning Objectives At the end of the session you should be able to: • Broad understanding of key principles and tools • Be able to use the DOWNTIME model to identify waste • Develop a project charter with your team • Explain why PDCA is an effective method for problem solving • Understand the components of PDCA • Document your PDCA process on an A3 Taking a Different Approach… “I’ve got too much work to do to stop and listen to you” “The Tools Are Available” 4 Lean Definition • Discuss what is lean What is Lean? • A management system and culture designed as a way we work by adding value for our patients and eliminating waste, where every employee is empowered to continuously improve their processes Lean is Not: • • • The flavor of the month Concepts that apply only to manufacturing A collection of tools and methods 5 History of Lean Late 1800’s Frederick Taylor (standard Work) Late 1800’s Early 1900’s Frank & Lillian Gilbreth (Time & Motion Study/ Process Mapping) Early 1900’s Early 1900’s Henry Ford (Flow Production) 1930’s Kiichiro Toyoda (Just in Time) 1930’s 1950’s W. Edwards Deming (PDCA) 1950’s Taiichi Ohno (Toyota Production System) 1950’s 1950’s Joseph Juran (TQM) 2009 UCLA Operating System 2009 1950’s Shigeo Shingo (SMED, ZQC) 2009 Mark Graban Shingo Research Award Lean Hospitals 6 UCLA Health Operating System Mission - Delivering leading edge patient care, education and research Vision - Healing humankind one patient at a time, by improving health, alleviating suffering, and delivering acts of kindness Values - Compassion, Respect, Excellence, Discovery, Integrity, Teamwork Lean Benefits How Will Lean Help Me? • • Solving problems and recognizing lasting results Establishes an environment that has controlled process, repeatable outcomes and delighted staff/patients What are the Benefits of Lean? Higher quality, safety & efficiency • Giving patients what they want when they want it • Increased staff satisfaction • More time with patients and business growth • 1. What are some more examples? In your area? 8 How we teach lean at UCLA Health Understand Value, Waste, & PDCA Current State Analysis SIPOC Root Cause Analysis Implement & Sustain Improvements Effective Solutions Pareto Process Mapping Standard Work Fishbone Time Obs. Project Lead: Veronica Corcoran Project Champion(s): Brad Rogers Facilitator: William Taylor SM Orthopaedics Clinic: Call Center Problem Statement: 53% of calls to the call center are for non appointment related issues Current State: Calls Patients Uses phone tree to triage call to scheduling New UCLA Pt? Schedulers and AAs YES To Pt Check-in Complete Forms Register Pt Identify Reason for Visit Does Pt Have Films? NO NO Verify Pt Info YES HMO Insurance? YES Auth for Clinic Visit? Redirect Pt to Their Referring MD or Medical Group NO PPO Insurance? NO YES Determine Correct MD •Use MD protocols •If HMO & no films schedule with general ortho Schedule Appt •Scheduling notes are entered Create Encounter & Link to Appt Provide Pt Instructions Create and Mail Packet •Parking •X-ray •Arrival time •Address •Co-pay •Docs to bring •Website... •Confirmation letter •Map of location •MD questionnaire •Consent for treatment Verify Correct Scheduling & Authorizations Print MD Schedule AAs YES Front Desk Print MD Schedule (if charts are in clinic) MAs Pull Existing Charts or Create New Chart Submit Radiology Orders if Needed •Write Pt name on chart •Include tabs, films, & auths •Sometimes new Pt questionnaire •Fax hardcopy or submit in IDX Send Charts to Clinic if Needed Print Encounter Sheet Add Encounter Sheet to Chart Print MD Schedule •Demographics •Labels •Charge Doc Pull Existing Charts or Create New Chart •Too much time spent on non-appointment issues •Time wasted looking for authorizations • Lack of trauma appt escalation process leads to 15+ minute phone calls for needs • Call abandonment rate: 8.6% (4Q-FY11) • Mothly call volume: 8,000+ Action Plan: Day Main Menu Option "3" Billing Inquiries Option "3" Return to Main Menu Option "1" Physician Bill Inquiries Option "2" Santa Monica Clinic Task Spine Phone Tree Edit script & send to Debbie Reduce the number of non-appointment incoming calls by 50% by December 2011. Spine Phone Tree Program new script PDCA / A3 Methodology Spine Phone Tree Record script Spine Phone Tree Go live UCLA Orthopaedic Day Menu •Phone options tree out of order •Callers automatically sent to appt line if they wait more than 4 seconds to make choice •Lack of consistent discharge process •Unable to reach AA •AA voicemail directions unclear •Clienttell may be confusing FPG Option "4" Orthopaedic Pediatric Clinic Option "5" Appointment Scheduling Pediatric Appointment Line Call Center Option "2" Ronald Reagan UCLA Medical Center Hospital Option "3" Santa Monica UCLA Medical Center and Orthopaedic Hospital Ronald Reagan Billing Santa Monica Billing Option "6" Physician Directory Physician Directory Attached Option "4" Return to Main Menu Call 310-319-1234 Do Option "1": Repeat Option "2": Return to Main Menu Act Solution/Initiative Daily Huddles Call 310-319-1234 Option "2" Medical Records Medical Records Westwood Clinic Goals and Dashboard Metrics: Analysis: Date: 12/2/11 UCLA Orthopaedic Day Menu Option "1" Address and Directions Option "1" Plan NO Are Charts Located in Project Team: Karen Meyers, Tina Nguyen, Stephanie Ngo, Kelley WestGrant Potential Solutions: •Redesign options on phone tree •Repeat main menu •Include physician directory on tree •Standardize AA voicemails across dept to include more information •Set expectation for same business day voicemail return (before 3pm) •Update Clienttell message to include x-ray info Active Daily Management Check Who Start ECD Done Stephanie 11/18/2011 11/21/2011 100% Debbie 11/18/2011 11/29/2011 100% Veronica TBD 12/9/2011 TBD 12/12/2011 11/18/2011 11/30/2011 Debbie Spaghetti Diagram 5 Why Operational Planning Day Main Menu Option "1" Appointments Option "2" Hospital, MD office, referring MD Option "3" Address & Directions Option "4" Orthopaedic Pediatric Clinic AA Same Day Callback New voicemail script Stephanie AA Same Day Callback Email instructions to AA Tina 11/18/2011 12/1/2011 AA Same Day Callback Record new voicemails AA's 12/1/2011 12/6/2011 Call Center Option "1" Westwood Clinic Option "2" Option "1" Physician Bill Santa Monica Clinic FPG Option "2" Ronald Reagan UCLA Medical Center Hospital Option "3" Santa Monica UCLA Medical Center and Orthopaedic Hospital Billing Inquiries Ronald Reagan Billing Santa Monica Billing Dashboard Metrics % of non appointment related calls Abandonment Rate Baseline 53% 8% Sustain the Results and Next Steps: Target 26.5% 6% Current 30% 5.8% •Daily monitoring of metrics during huddle •CICARE rounding •Identify new phone system that would allow manager to interject in calls whne the call needs to be escalated •Evaluate phone tree monthly for glitches or new suggestions Change Mgmt Seeing With New Eyes 10 Seeing with new eyes requires an understanding that activities either add value or waste… Why? This allows you to focus your resources (to eliminate waste, increase value, or support value) • Waiting in general • Waiting for orders to be written • Late/missing callback for tests • Clinical or operational errors • Unnecessary documentation • Unnecessary approvals Activities that are Wasteful (any can be true) • The patient is not willing to pay for • That do not move the care process forward • That are not done right the first time WASTE VALUE • Comforting a patient • Examining a patient • Diagnosing a patient • Treating a patient • Educating a patient Intro Value Analysis Waste Analysis Activities that add Value (all must be true) • The patient is willing to pay for • That moves the care process forward • That are done right the first time RCA RCA Causes RCA – Pareto RCA – Cause & Effect RCA – 5 Whys 11 Value-Added & Non-Value Added Example Value-added Actions 1 3 Pt checks in, pays co-pay 2 8 MA takes vitals and rooms pt Pt waits in waiting area 4 5 MD completes consult Pt waits for MD in room 6 Pt receives AVS and schedules f/u appt if necessary Pt waits 7 Pt waits to nurse/MA to checkout come and complete visit Non-Value-added Actions 12 Waste models can help you identify/find waste For “non-value added” activities, next you find/identify waste; this is made easier by using a model such as DOWNTIME* Mistakes, errors, resulting rework Producing too much, too soon, or excessive setup Actual downtime (patient, service, or production) Poor use of skills and talents, knowledge loss Moving things around Too much inventory, or too little People moving around, searching, etc. Duplication, unnecessary: refinements, approvals - •D efects •O verproduction •W aiting •N ot utilizing Talent •T ransport •I nventory •M otion •E xtra Processing *Different systems classify wastes into different amounts of categories. Most use 7 (same as above but without N) or 8 but some use up to 11! ** There are different types of waste – Type 1 and Type 2. Type 1 adds no value and can be removed easily. Type 2 adds no value but is necessary in the current system and/or is very difficult to remove. This distinction will become more important when focusing on solutions Intro Value vs Waste Waste Analysis RCA RCA Causes RCA – Pareto RCA – Cause & Effect RCA – 5 Whys 13 Eight Wastes in Ambulatory Processes… Defects Overproduction Waiting Not Utilizing Talent ▪ Incomplete Specialty referrals ▪ Full sheet of labels printed when only one is needed ▪ Pt waits in exam room for MD ▪ Numerous ideas are “lost” only to be rediscovered later ▪ MD/Nurse time spent on clerical tasks Transport Inventory Motion Extra-Processing ▪ Patients are taken from waiting room -> vitals intake -> waiting room -> exam room ▪ Expired supplies because of excess ordering ▪ MA/Nurse spends time looking in multiple places for a particular supply ▪ Patients asked the same questions multiple times 14 Waste Waste 15 A3s and A4s are used to communicate progress A4 Problem-Solving (8.5 x 11) A3-Problem Solving (11 x 17) Everyday problem-solving, consensus & communication tool used by staff Complex problem-solving, consensus, communication tool Known root-causes and solutions Unknown root-causes and solutions Quick and easy to use Requires Planning (PDCA) and usually data Example: Peanut butter and jelly sandwiches in the RR. Example: A unit wants to improve poor patient satisfaction scores but they do not understand why the scores are so poor or how to improve them 16 We will be working with A3s today A4 Problem-Solving (8.5 x 11) A3-Problem Solving (11 x 17) Everyday problem-solving, consensus & communication tool used by staff Complex problem-solving, consensus, communication tool and project management tool Known root-causes and solutions Unknown root-causes and solutions Quick and easy to use Requires Planning (PDCA) and usually data Example: Peanut butter and jelly sandwiches in the SMH. Example: A unit wants to improve poor patient satisfaction scores but they do not understand why the scores are so poor or how to improve them 17 Project Charter Project Charter 4W UPC Assaults A3 Vision Statement The staff on the 4 West Child/Adolescent psychiatry unit will have resources, tools, and evidence-based protocols necessary to minimize the assault rate. At a minimum, the unit will maintain assault rates lower than the NDNQI assault and assault with injury benchmarks. This will allow staff to deliver the highest quality of care to all patients and minimize disruptions to the milieu caused by aggressive patients. Staff will feel safe while providing care to all patients and staff, patients, and visitors on the 4 West unit will remain free from injury related to patient assaults. Problem Statement During the month of January, 4W recorded 38.2 assaults per 1000 patient days, and similar figures for the past two quarters (July-Sept= 58.3, Oct-Dec= 29.5), which are well above the NDNQI of 18.6assaults/1000 patient days. Objective Statement Objectives Criteria for Evaluation 1. Reduce the assault rate to 0 and maintain assault rates below the NDNQI 1. Assault rate benchmark. 2. Documentation of protocols in CareConnect 2. Develop protocols for: 3. The number of patient groups canceled or relocated due to an aggressive patient a. Handling aggressive patients 4. The number of times nonaggressive patients are relocated due to an aggressive b. Staffing assignments for aggressive patients patient c. Lead RN rounding & Standard Work for aggressive patients 5. The number of times visitors are impacted by assaultive patients d. Handoff consistency 6. Staff perception of safety on the unit 3. Improve staff safety on the unit as evidence by absence of staff injuries related to 7. Staff perception of lead nurse support related to care of the aggressive patient assaultive behavior 8. Satisfaction/unit culture survey, nurse burnout 4. Improve staff moral as evidenced in the staff satisfaction/unit culture survey 9. Staff perception of interdisciplinary communication and collaboration related to 5. Improve interdisciplinary communication and collaboration related to treatment treatment and management of aggressive patients and management of aggressive patients 10. Information related to aggressive patients and assaults is communicated in huddles Project Scope Boundaries In Scope Out of Scope Deliverables Process Starts: When assignments CareConnect smart text New CareConnect build Evidence-based protocols for handling are made by the off-going charge Leader Standard Work & Assignments Staffing ratios aggressive patient, staffing assignments nurse Plan of care & medications Relocation of the seclusion room for aggressive patients, lead RN Huddles & Performance Boards Patient placement/admissions standard work and rounds, handoffs Process Ends: End of Shift handoff Assaultive patients room placement LOS: acute vs long term care CareConnect Smart Texts Major Milestones What Fishbone Diagram Complete Root Cause Analysis Mtg Team: Sponsor/Process Owner: Scott Grosz, MSN, RN Sponsor/Physician: Mark De Antonio, MD Team Leader: Kandace Whiting, MSN, RN-BC Facilitators: William Taylor Team Members: Jonathan, PhD, RN Quan Phan, BSN, RN, Joyce Reinholdt, BSN, RN Lin, Brittany, MSN, RN Alaina Burns, MD, Galya Rees, MD, Miranda Daniel, MSW Other Stakeholders: Pat Matos, DNP, RN, NEA-BC Who Unit Staff A3 Team When 4/22/14 4/23/14 Team Roles: Sponsor/Process Owner: (2-5 hr/wk) Provides leadership support; validates project objective and approach; ensures availability of appropriate resources and support; helps to remove cross-functional barriers. Sponsor/Physician: (min 1 hr/wk) Provide feedback on project direction and plans, build consensus with other physicians, promote open environment for change, foster 2-way communication between all stakeholders Facilitator: Partners with champion and team leader to manage scope, issues, and risk; works side by side with team; provides lean coaching and consulting for project, challenges traditional thinking Team Leader: (10-20 hr/wk) Partners with facilitator for the planning and the development of all project deliverables; responsible for managing team members, implementation and sustaining gains Members: (5-10 hr/wk) Participate in project as requested by team leader and facilitator – including: completing assigned work ; informing the project leader of issues, scope changes, risk and quality concerns; communicating changes to peers 18 19 PDCA – Continuous Improvement • A structured guide and method for problem solving • The way by which we should be practicing continuous improvement in our daily work Plan Step 1 Step 2 Clarify the Problem Analyze Current State Do Step 3 Step 4 Step 5 Check Step 6 Develop Analyze Implement Evaluate Goals Root Cause Solutions Results Plan Do Act Check Act Step 7 Adjust, Standardize & Sustain