Business Case for Adoption:
The Federal Perspective
1
Copyright 2009. All Rights Reserved.
Quality Improvement
Opportunities Using CONNECT
A Proof of Concept for Changing the
Traditional Methods of Data Exchange
Michael Reinhold
Acting Deputy Group Director, Information System Group,
Office of Clinical Standards and Quality,
Centers for Medicare and Medicaid Services
Copyright 2009. All Rights Reserved.
Quality Improvement
• Delivering Care in a safe, effective and
efficient manner
• Ensuring great communication between
health care providers and their patients
• Proper and effective stewardship of health
care services
• Eliminating redundancy of care
• Ensuring care is evidence-based and
outcome-driven to manage and prevent
complications from disease
• Educating consumers of health care
services
• Rewarding health care providers for quality
improvement
3
Copyright 2009. All Rights Reserved.
CMS Quality Initiatives
The Reporting Hospital
Quality Data for Annual
Payment Update
(RHQDAPU) Program
The
Medicare
Home
Health
Quality
Program
• 42 Hospital measures
• Clinical Process
• Clinical Outcome
The Physician Quality
Reporting Initiative
(PQRI) Program
The Medicare Outpatient
Prospective Payment
System (OPPS) Program
• 7 outpatient measures
• Clinical Process
• Clinical Outcome
The Medicare End
Stage Renal Disease
(ESRD) Program
• 153 Physician Office
Measures
• 26 Clinical Performance
Measures (CPM)
• Clinical Process
• Clinical Process
• Clinical Outcome
• Clinical Outcome
4
Copyright 2009. All Rights Reserved.
The
Medicare
Electronic
Prescribing
Program
Current Methods of Data Collection
for Purposes of Quality Improvement
Claims Based
Electronic Upload (EU)
• Normal CMS Claims
Processing
• Web interface
Custom
Registry or Vendor
• Web Based Single User
Interface – DE
• Sending Data to Entity to
Submit on Behalf
• Extraction Tools for
Distribution
• Usually Uses One of the Other
Identified Methods – EU
5
Copyright 2009. All Rights Reserved.
• Batch or shipped media
Looks Good to Me Why Change
Current Methods of Data Collection?
2
Vendor
Claims Method
1
3
4
Billing
Software
•
•
•
•
Various Billing Packages not all uniform and no interoperable standards
Cost to update, train, switch and maintain
Not developed for purposes of quality reporting - but billing for payment
Step for errors to occur in data transaction around quality data
Carrier/MAC
•
•
•
•
Various systems and internal processes
Costly to update, train, switch and maintain
Not developed for purposes of quality reporting – but billing for payment
Step for errors to occur in data transaction
Internal
Transactional
Processes
•
•
•
•
Various systems and internal processes
Costly to update, change and maintain
Not intended to ensure quality data is properly captured
Step for errors to occur in data transaction around quality data
•
•
•
Various systems and internal processes
Costly to update, train, switch and maintain
Not developed for purposes of quality payment– but transactional payment
•
•
•
•
Various systems and internal processes
Costly to update, change and maintain -must change based on Claims processing systems
Performed months after initial data submitted
Step for errors to occur in data transaction
•
•
•
Various systems and internal processes
Costly to update, train, switch and maintain – must change based on Claims processing systems
Performed months after the initial data submitted
Payment
Internal Quality
Processes
Quality
Decisions
5
Data lag for Quality decisions and 4-5 major steps where data errors can occur on
Quality Data – Never designed for Quality Purposes
6
Copyright 2009. All Rights Reserved.
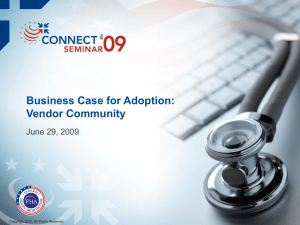
Looks Good to Me Why Change
Current Methods of Data Collection?
Electronic Upload
Vendor
2
Provider
Software
Access/System
Registration
Submit Data
•
•
•
•
•
•
• Depending on program variant file specifications
must be met
• Leaves room for duplication of data and formatting
particularly if participation in many programs/efforts
• Usually measure driven - not data driven
• Step for errors to occur in data transaction
1
Various systems and processes along with file specifications depending on program
Burden/duplication on training
Feedback submission report issues
Usually limited time for submission depending on program and data required
Usually measure driven not data driven
Step for errors to occur in data transaction around quality data
• Various systems and processes along with file
specifications depending on program
• Burden/duplication on training
• Feedback submission report issues
• Usually limited time for submission depending on
program and data required
• Usually measure driven not data driven
• Step for errors to occur in data transaction around
quality data
Data Processes
•
•
•
•
•
•
Various systems and internal processes
Duplication depending on different specifications
Costly to update, switch and maintain
Extremely resource intensive based on submission periods
Usually measure driven not data driven
Step for errors to occur in data transaction around quality data
Internal Quality
Processes
•
•
•
•
•
Various systems and internal processes
Duplication depending on different specifications
Costly to update, switch and maintain
Extremely resource intensive based on submission periods
Validation is difficult to perform efficiently
Quality
Decisions
7
• Various Packages not all uniform and no
interoperable standards
• Cost to update, train, switch and maintain
• Often not developed for purposes of quality
reporting – retro fitted or manual interaction to meet
program data out needs
3
4
• Various systems and internal processes
• Costly to update, train, switch and maintain – mostly due to duplication and lack of interoperability standards
• Often does not accommodate timely feedback and data resubmission
Data lag is far less, however, allows for duplication of data submission, training and systems
in conjunction with timely submission & feedback issues. Also generally requires a
considerable amount of end user support.
Copyright 2009. All Rights Reserved.
Looks Good to Me Why Change
Current Methods of Data Collection?
Registry or Vendor
Provider
Software
•
•
•
•
•
•
Various Packages not all uniform and no interoperable standards
Cost to update, train, switch and maintain
Often not developed for purposes of quality reporting – retro fitted or manual interaction to meet program data out needs
Depending on program variant file specifications must be met
Leaves room for duplication of data and formatting particularly if participation in many programs/efforts
Step for errors to occur in data transaction
Registry or
Vendor
•
•
•
•
•
Various Packages not all uniform and no interoperable standards
Cost to update, train, switch and maintain
Depending on program variant file specifications must be met
Quality control issues
Usually measure driven - not data driven
Access/System
Registration
Submit
Data
Data
Processes
Internal Quality
Processes
Quality
Decisions
8
Usually disconnected
from the Registry system
1
2
• Various systems and processes to follow depending on what program participation is in
• Burden/duplication on training
• Can create confusion depending on reporting periods and programs in in more than one
•
•
•
•
•
•
Various systems and processes along with file specifications depending on program
Burden/duplication on training
Feedback submission report issues
Usually limited time for submission depending on program and data required
Usually measure driven not data driven
Step for errors to occur in data transaction around quality data
•
•
•
•
•
•
Various systems and internal processes
Duplication depending on different specifications
Costly to update, switch and maintain
Extremely resource intensive based on submission periods
Usually measure driven not data driven
Step for errors to occur in data transaction around quality data
•
•
•
•
•
Various systems and internal processes
Duplication depending on different specifications
Costly to update, switch and maintain
Extremely resource intensive based on submission periods
Validation is difficult to perform efficiently
3
4
• Various systems and internal processes
• Costly to update, train, switch and maintain – mostly due to duplication and lack of interoperability standards
• Often does not accommodate timely feedback and data resubmission
Data lag is far less, however, allows for duplication of data submission, training and systems
in conjunction with timely submission & feedback issues. Also generally requires a
considerable amount of end user support.
Copyright 2009. All Rights Reserved.
Looks Good to Me Why Change
Current Methods of Data Collection?
Custom
Provider
Software
Access/System
Registration
Provider Uses
System Interface
Data Processes
Internal Quality
Processes
Quality
Decisions
9
Usually disconnected from
• Various Packages not all uniform and no interoperable standards
• Usually does not interact with Custom interface for data entry
the Custom interface
• Cost to update, train, switch and maintain
• Leaves room for duplication of data entry – The provider system and the Custom interface
• Various Packages not all uniform and no interoperable standards
• Usually does not interact with Custom interface for data entry
• Cost to update, train, switch and maintain
• Leaves room for duplication of data entry – The provider system and the Custom interface
• Various systems and processes – may collect duplicate data
• Burden/duplication on training
• Data entry errors
• Performance factors may arise
• Usually limited time for submission depending on program and data required –manual burden
• Usually measure driven not data driven
1
2
Usually requires increased
• Various systems and internal processes
• Duplication depending on different specifications
security requirements
• Costly to update, switch and maintain
• Extremely resource intensive based on submission requirements
• Usually measure driven not data driven
• Step for errors to occur in data transaction thus leading to end user frustration and increased inquiry support
• Various systems and internal processes
• Duplication depending on different specifications
• Costly to update, switch and maintain
• Extremely resource intensive based on submission periods
• Validation is difficult to perform efficiently thus leading to enormous inquiry support efforts
• Various systems and internal processes
• Costly to update, train, switch and maintain – mostly due to duplication and lack of interoperability standards
• Often does not accommodate timely feedback and data resubmission
Usually no data lag, however allows for duplication of data submission, training and systems. Also
generally requires a considerable amount of end user support to include detailed inquiry support. The
biggest con is in most cases the provider still has to enter the data into their system – duplicate data entry
Copyright 2009. All Rights Reserved.
Summary:
Current
• Current methods are not wrong. They were the best way of doing
business with the resources and technologies available
• Until new technologies and/or architectures are created we have to live
with them
• This means cost increases as quality initiatives and data populations
increases
How do we move from here to there ?
Quality
initiatives
Improving
quality
Cost
Cost
10
Copyright 2009. All Rights Reserved.
ONE Answer is develop an New
Architecture and Method for Data
Collection
Nationwide Health Information Network (NHIN) and CONNECT Architecture
Mission
To achieve better quality, value, and affordability of health and wellness services by
establishing the Nationwide Health Information Network as the common, secure,
nationwide, interoperable network for exchanging health information, and provide
this infrastructure with low adoption barriers.
Provides
• Ability to look up, retrieve and securely exchange health information
• Ability to apply consumer preferences for sharing information
• Ability to apply and use the NHIN for other business capabilities as authorized by
the health care consumer
• Interoperability Architecture
In short provides a single architecture/method for health care data exchange
11
Copyright 2009. All Rights Reserved.
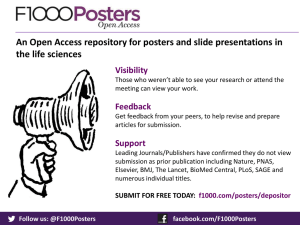
Use Test Case/Proof of Concept
HIE DEV Instance
Test QRDA
Documents
QRDA
NHIN
Gateway
QRDA
NHIN
A Perfect Business
Use Test Case in
Practice
NHIN CONNECT
or other Gateway
CMS
NHIN Gateway
EHR Application
(Data/Structural Validation)
The Physician Quality Reporting
Initiative (PQRI) program
ALS ESB (existing)
Currently uses all four current methods
of data exchange–
EHR Data Application
(Data Parsing and Storage)
1.Claims
2.Electronic Upload (EU)
Phase out EU and Custom
3.Registry through EU
4.Custom Data Entry App
Develop new NHIN method to retrieve
data required as needed eliminating or
simplifying other methods
12
Copyright 2009. All Rights Reserved.
Database
QRDA
Document Processor
Connect Proof of Concept Goals
• Embark upon a 4 step proof-of-concept:
– Increase/accelerate exposure to NHIN technology and overall business
process framework and direction within CMS
• Increase business understanding to better influence future design and business
process/policy use considerations
• Increase functional and technical system design – including security and
scalability considerations to reduce possible future implementation risk
– Simulation of submission of QRDA data from an EMR, through an HIE,
over the NHIN to CMS
• Four steps are planned during the POC:
– Test gateway-to-gateway communication
– Test QRDA exchange
– Enhance gateway to integrate and comply with current Quality systems
components
– Pilot test with other HIEs and possibly other relevant stakeholders
13
Copyright 2009. All Rights Reserved.
Important Points
• Following NHIN Interoperable standards CMS should be able to integrate
and enhance gateway to comply with current Quality systems
components and increase overall functionality with other Quality
systems/programs
• Once integration is complete and data exchange is proven from an HIE
CMS can :
– Pilot test with other HIEs and possibly other relevant stakeholders
– Provide feedback on any NHIN improvement areas
– Expand testing to other Quality Programs
– Obtain and provide feedback on quality data sooner
– Lessen the burden on external stakeholders that belong to HIE’s or are an
HIE that have adopted the NHIN architecture standards
– Reduce redundancy in systems and data request
– Expand quality measurement data specifications to EHR vendors
– Continue to work with standards organizations such as HL7 to expand or
modify CDA templates
14
Copyright 2009. All Rights Reserved.
In Summary
“Technology does not drive
change – it enables change”
Following NHIN Interoperable standards
and architecture around new technology
areas, CMS believes that current
methods of Quality Data collection could
be simplified to achieve better quality,
value, and affordability. As CMS and
other organizations adopt the NHIN
architecture it will help lessen the burden
of data exchange to all stakeholders and
help increase quality improvement. CMS
is working on enabling change through its
various Quality, Medicare, and Medicaid
programs!
15
Copyright 2009. All Rights Reserved.
“Believe you can and
you're halfway there”
“Far and away the best
prize that life has to offer
is the chance to work hard
at work worth doing”
Quotes by
Theodore Roosevelt
Q: WHAT CAN THE
SYSTEM DO?
A: WHAT DO YOU
WANT IT TO DO?
Enhanced Care Delivery by
CONNECTing to the NHIN:
Improving Disaster Medical Care
Robert Bencic, DDS, MBA
CAPT USPHS
Director, QA
National Disaster Medical System
Copyright 2009. All Rights Reserved.
Problems Caused by
Disconnected Systems
Patients are removed from their typical medical
providers and care plan
Inability to acquire patient care information from
other Federal partners (DoD, VA, SSA, IHS, CMS)
Inability to share information among various
response locations in a federally declared disaster
Inability to quickly send data to other healthcare
providers
17
Copyright 2009. All Rights Reserved.
Expected Benefits from
CONNECTing to the NHIN
• Access to medical data from other
deployment locations
• Enable the acquisition of patient
information from other federal departments
(VA, CMS)
• Lay groundwork for future information
sharing with non-federal government
entities (hospitals, pharmacies, urgent care
centers, and state programs)
• Enhance the usability of NDMS Disaster
Medical Information System (DMIS)
18
Copyright 2009. All Rights Reserved.
DMIS Continuum of Care
19
Copyright 2009. All Rights Reserved.
What This Means for the Rest
of the Healthcare Industry
• NDMS can leverage ONC’s
standards and achieve its goal of
having a standard framework for
retrieving and sending patient
data to other healthcare providers
• CONNECT software will minimize
the in-house development time
and costs
• Leveraging standard CONNECT
software enhances patient care
while minimizing limited
implementation resources
20
Copyright 2009. All Rights Reserved.
CONNECTing the
Indian Health System
James Garvie, CAPT, USPHS
Deputy Director, Division of Information Resources
Indian Health Service
Copyright 2009. All Rights Reserved.
IHS as a Provider of Health Services
American Indian and Alaska Native Healthcare
CHALLENGES
• Information tends to be
facility-based and is generally
not available to staff at other
IHS, Tribal or Urban Indian
facilities.
• There is no central registry of
Indian health system
patients, providers and other
resources.
• Secure messaging is not
available among Indian
health system facilities.
22
Copyright 2009. All Rights Reserved.
SECURE EXCHANGE
OF INTEROPERABLE
HEALTH INFORMATION
Patients
Providers
Population
Health
CONNECT Solution
EXPECTED
OUTCOMES
• Information at the point of
care from all Indian health
system sources.
• Immediate access to
patient, provider and
essential health resource
information.
• Secure messaging
throughout the Indian
health system.
IHS as a Payor for Health Services
American Indian and Alaska Native Healthcare
CHALLENGES
• IHS and Tribal programs
purchase health services that
are not available within the
Indian health system.
• Information regarding
purchased care conforms to
financial formats and is often
clinically incomplete.
• Purchased care providers
generally do not have
electronic health record
systems.
23
Copyright 2009. All Rights Reserved.
SECURE EXCHANGE
OF INTEROPERABLE
HEALTH INFORMATION
Patients
Providers
Population
Health
CONNECT Solution
EXPECTED
OUTCOMES
• Information at the point of
care from all health system
sources.
• Complete, clinically
relevant information.
• Seamless sharing of health
information by all
healthcare providers.
IHS and Population Health
American Indian and Alaska Native Healthcare
CHALLENGES
• Notifiable disease reporting
capabilities vary considerably
among states.
• Immunization and disease
registry functionality is
inconsistent among collecting
organizations.
• Reporting is usually paperbased, sometimes via web
portal and rarely from an
electronic health record
system.
24
Copyright 2009. All Rights Reserved.
SECURE EXCHANGE
OF INTEROPERABLE
HEALTH INFORMATION
Patients
Providers
Population
Health
CONNECT Solution
EXPECTED
OUTCOMES
• Increased standardization
among states for notifiable
disease reporting.
• Increased standardization
among registry
oganizations.
• Direct, bidirectional
exchange of information
between EHRs and
reporting, registry
organizations.
CONNECTing the Indian Health System
Facilities
MPI
Integration
Engine
IHS
Adapter/
Gateway
Facilities
MPI
Integration
Engine
Tribal
Adapter/
Gateway
Internet
25
Copyright 2009. All Rights Reserved.
Facilities
MPI
Integration
Engine
Urban
Adapter/
Gateway
A Snapshot of Success:
CONNECT’s Demonstrated
Achievements
Dr. Taha Kass-Hout, MD, MS
BioSense Program Manager
US Centers for Disease Control and Prevention
Copyright 2009. All Rights Reserved.
Web Search Volume Screenshot
27
Copyright 2009. All Rights Reserved.
Source: GI4S
Web Search Volume Screenshot
28
Copyright 2009. All Rights Reserved.
Source: GI4S
Web Search Volume Screenshot
29
Copyright 2009. All Rights Reserved.
Source: GI4S
iPhone App Store Analogy
Photos Credits: Raven Zachary and Scott Janousek
30
Copyright 2009. All Rights Reserved.
Enhanced Care Delivery:
Problems Caused by
Disconnected Systems
• Critical data needed for surveillance is
not captured in many instances
• Acquired information is not received in a
timely manner
• Public health interventions are delayed
• Ability to communicate critical messages
to the medical community is impaired
• Community health programs are not
designed and monitored effectively
31
Copyright 2009. All Rights Reserved.
Enhanced Care Delivery:
Expected PH Benefits from
CONNECTing to the NHIN
• Enhanced surveillance capabilities to support situational
awareness and notifiable disease scenarios in a timely
manner
• Integration of relevant public health information into
decision support processes effective response
• Improved community health intervention and evaluation
processes
Reduce Morbidity and Mortality and Improve Outcomes
32
Copyright 2009. All Rights Reserved.
BioSense Strategy Overview
Next Generation:
Present Strategy:
• Situational awareness
• Syndromic monitoring and
electronic laboratory reporting pilots
• Centralized model with CDC
stewardship of data
• State systems, national sources, &
individual hospitals
• Sharing of aggregated (summary)
data across jurisdictions
• Social networking model Trust
• Federated model with joint state &
CDC stewardship Feasibility
• Service Oriented Infrastructure
• Supports many surveillance needs
(e.g. ELR)
• State systems, national data sources,
NHIN
33
Copyright 2009. All Rights Reserved.
Biosurveillance using Summary Data
Geocoded Interoperable Population Summary
Exchange (GIPSE) Services
Value of Aggregate Data
– Public Health surveillance/quality monitoring
– Response to natural/manmade disaster
– Cross-jurisdictional situational awareness
GIPSE Format
– Provides access to data by leveraging service oriented architecture or grid methods
to expose summaries of data within state and local systems
– Each service returns a set of aggregate counts that map to a common geographic
data structure
– Supports aggregation
– Supports computation and testing using spatio-temporal anomaly (e.g., SatScan)
methods
– Developed as CDC-hosted open source project
34
Copyright 2009. All Rights Reserved.
Biosurveillance using Summary Data
Geocoded Interoperable Population Summary
Exchange (GIPSE) Services
• CDC uses NHIN Gateway to subscribe to summarized Biosurveillance data
from State Health Departments (SHD)
• SHD’s publish summarized biosurveillance data via NHIN Gateway
• CDC aggregates and visualizes summarized data using Quicksilver or other
summary data viewers
3. Quicksilver Viewer
CONNECT
Gateway
CONNECT
Gateway
CONNECT
Gateway
35
Copyright 2009. All Rights Reserved.
GIPSE
A set of matrices
Aggregates (e.g.; counts, rates, or alerts)
Zip codes
Date range
1,2,3,5,0,6,…
2,1,4,7,0,3,…
….
….
….
ILI
36
Copyright 2009. All Rights Reserved.
Abdominal
Rash
GIPSE
+ adds cross tabulation on age category
and gender
Date range
+
ILI
37
Copyright 2009. All Rights Reserved.
Zip codes
Zip codes
Date range
National Biosurveillance Model:
Summary Perspective
Systems
Partners
DISTRIBUTE
State Health Departments
RODS
State Health Departments
ESSENSE
BIOSENSE
CDC
NEDSS
National Poison Control Center
Regional HIE
Local Health Departments
Hospitals, Clinics, etc.
NHIN Gateway
38
Copyright 2009. All Rights Reserved.
POISON DATA
Summary Data Source
Summary Data Source
Clinical Data Source
Summary Data Bus
State Health Departments
GIPSE SERVICES
REGISTRY
CLIENT VIEWER
Authenticated
Cardea
Cardea is a platform and a set of services that build
a general purpose interface to support message
transformation and workflow intelligence between a
healthcare system/laboratory/health information
exchange and public health
BioSense Integrator Pilot in GA, 2009
39
Copyright 2009. All Rights Reserved.
What This Means for the Rest of the
Healthcare Industry?
• Enhanced surveillance capabilities are an important
component in improving the overall health of the
population, serving to reduce health care costs
• Quality of care can be positively impacted when clinicians
have easy access to important public health information
• Health disparities can be recognized, assessed and
evaluated more effectively with more robust surveillance
capabilities
Enhanced Care Delivery
40
Copyright 2009. All Rights Reserved.
Thank You!
Taha Kass-Hout, MD, MS
BioSense Program Manager
Centers for Disease Control and Prevention
Les Lenert, MD, MS, FACMI
Director, National Center for Public Health Informatics
Centers for Disease Control and Prevention
Barry Rhodes, PhD
Division of Emergency Preparedness and Response (DEPR) Director (Acting)
Centers for Disease Control and Prevention
41
Copyright 2009. All Rights Reserved.
Business Case for Adoption:
National Cancer Institute/caBIG
George A. Komatsoulis, Ph.D.
Deputy Director
NCI Center for Biomedical Informatics and
Information Technology (CBIIT)
Copyright 2009. All Rights Reserved.
Individualized, Targeted Cancer Care
43
Copyright 2009. All Rights Reserved.
NCI Cancer Research Enterprise
The cancer Biomedical Informatics Grid (caBIG)
was initiated in 2004 to connect the disparate parts
of the cancer community via a semantically
Interoperable Service Oriented Architecture (SOA)
44
Copyright 2009. All Rights Reserved.
= NCI-Designated Cancer Centers
= CCOPs
= NCI Community Cancer Centers
caBIG® Enables All Major Functions
Needed to Link Research to Care
Clinical Research
Molecular Biology
45
Copyright 2009. All Rights Reserved.
Imaging
Pathology
caBIG® Enables All Major Functions
Needed to Link Research to Care
• Track clinical trial
registrations
• Utilize the National
Cancer Imaging Archive
repository for medical
images including CAT
scans and MRIs
• Facilitate automatic
capture of clinical
laboratory data
• Visualize images using
DICOM-compliant tools
• Manage reports
describing adverse
events during clinical
trials
Clinical Research
Imaging
• Annotated Images with
distributed tools
• Combine proteomics,
gene expression, and
other basic research data
• Access a library of well
characterized, clinically
annotated biospecimens
• Submit and annotate
microarray data
• Use tools to keep an
inventory of a user’s
own samples
• Integrate microarray data
from multiple
manufacturers and permit
analysis and visualization
of data
46
Copyright 2009. All Rights Reserved.
Molecular Biology
Pathology
• Track the storage,
distribution, and quality
assurance of specimens
NCI caGrid Portal Screenshot
47
Copyright 2009. All Rights Reserved.
December caBIG/NHIN Demonstration:
Partnership that Promotes Child Care
Demonstration illustrated:
• Methods for physicians conducting clinical trials to obtain health
history and treatment information
• Methods for sharing details about care received during trial
• Ways to share care information with future healthcare providers
• How continuity of care can be achieved through partnerships
between federal and private care providers
48
Copyright 2009. All Rights Reserved.
Integrating with the NHIN
NHIN Services
(WSDL)
caBIG® Services
(WSRF and WSDL)
Subject
Discovery
Subject
Discovery
Document
Query
Document
Query
Document
Retrieval
Document
Retrieval
INTRODUCE Generated caGrid Service Wrappers
49
Copyright 2009. All Rights Reserved.
NHIN and caBIG® Moving Forward
• A caBIG® compatible NHIN solution is simply a matter of capturing
the semantics of the service
– Provides both a Grid Service and a conventional Web Service
• A “caBIG® compatible” NHIN gateway could be deployed at
caBIG® participating institutions (that have significant expertise in
deploying caBIG® technology)
• Similarly, caBIG® could become “NHIN compatible” by supplying
caBIG® compatible versions of NHIN services
50
Copyright 2009. All Rights Reserved.
Leveraging the NHIN to Improve the
Disability Determination Process
Authorized Release of Information
Justine Piereman
Senior Advisor to the Office of the
Deputy Commissioner for Systems
Social Security Administration
Copyright 2009. All Rights Reserved.
An American First: The Telegraph
Human-to-Human Transmission
of Text Over Wire
• Innovation supported by the
Congress
• First test - Baltimore to
Washington – 38 miles
• Standardized language
(Morse Code)
• Rapid expansion by private sector
• Benefits to citizens
52
Copyright 2009. All Rights Reserved.
–
Expansion of commerce
–
Immediate access to news
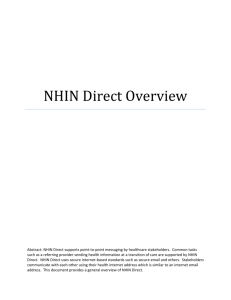
Another American First:
Live patient transfer across the NHIN
NHIN
Patient
Information
Patient
Information
This one-way electronic transfer of patient data between MedVirginia,
a regional health group, and the Social Security Administration will
enable SSA, with the patient’s authorization, to obtain medical
records for the disability review process in minutes instead of the
current weeks and months.
53
Copyright 2009. All Rights Reserved.
The Face of Disability
54
Copyright 2009. All Rights Reserved.
Nationwide Health Information
Network
State
Agency
Phone, Web,
In-Person
Med Records
Labs
Background
DETERMINATION
RECOMMENDATION
St. Francis Medical
Center
St. Mary’s Hospital
NHIN
SSA
Field
Office
Demographic
Information
DECISION
MADE
55
Copyright 2009. All Rights Reserved.
SSA National
Computer System
Med Records
Labs
Background
Claimant Electronic Folder
Memorial Regional
Medical Center
+
CONNECT
Auth. To Release
Medical Records
Richmond Community
Hospital
Information
Available
About Claimant
Additional Providers
brought to the
NHIN through
ARRA and other
mechanisms in
FY2009 and beyond
Enhanced Care Delivery
by CONNECTING to the NHIN
Dr. Steve Steffensen
Chief Medical Information Officer
Telemedicine & Advanced Technology
Research Center
Copyright 2009. All Rights Reserved.
Department of Defense
Commitment to Care
Military Beneficiaries: 9.3 million
Military Bases in US: 202
Military hospitals
63
Medical/Dental Clinics
Encounters/month
9 million
Average outpatient visits/year/patient
826
4
1:4 military families move in a given year
<50% of network consults make it back to the PCM
CONUS Military Bases
74%
57
Copyright 2009. All Rights Reserved.
70%
59%
56%
Federal and Private Partnership
Dr. Tim Cromwell
Director, Standards and Interoperability
Office of Health Information
Veterans Health Administration
Jamie Ferguson
Executive Director of Health IT Strategy
and Policy Kaiser Permanente
Copyright 2009. All Rights Reserved.
Introduction
• The US Department of Veterans Affairs (VA) and
Kaiser Permanente (KP) have collaborated on
clinical standards development and other
interoperability issues prior to NHIN
• Our limited production implementation sharing
standardized health information for patient care will
go live late in 2009
• Our teams have been meeting regularly, working to
resolve a myriad of issues in three main areas:
– Technical capability
– Operational preparedness
– Policy
• We think we have a story to tell about what we have
done so far
– Lessons learned
– Challenges remaining
59
Copyright 2009. All Rights Reserved.
Outline
Introduction
Business Case
VA
|
KP
Challenges
Technical
|
Operational
Conclusion
60
Copyright 2009. All Rights Reserved.
|
Policy
Business Cases
Veterans Affairs
Kaiser Permanente
• 3 out of 4 Veterans receive care in the
private sector
• Many thousands of KP members receive
care from VA
• More and more private sector providers
will use EHRs
• Improved information can help clinical
decision-making
• Complete set of data will lead to better
quality of care
• Complete set of data will lead to better
quality of care
• Veteran satisfaction with overall care will
be higher
• Opportunity to avoid duplicate or
conflicting clinical orders
• Executive Order 13410 mandates use of
recognized standards for Agencies
• Additional cost reduction from automation
of manual processes
• Executive Order 13410 mandates use of
recognized standards for FEHB carriers
61
Copyright 2009. All Rights Reserved.
Technical:
Physical Environments
VA
• KP
• Lab environment in 2008 Trial
Implementation
• Test environment remains from
2008 NHIN Trial Implementation
• Internal development environment
• Internal development environment
• CONNECT Gateway received
from FHA
• Adapter developed internally
• Test
• Test databases, test systems, test
patients
• Production environment
• TBD
62
Copyright 2009. All Rights Reserved.
• Internally-developed NHIN
Gateway (not using FHA
CONNECT software)
• Shared environments with EHR
systems and other internal
systems
• Production environment
• TBD
Technical:
Interfaces to Existing Systems
VA
• KP
• Viewer: VistAWeb
• Web services interface to EHR
• Data sources: 128 VistA instances
• Terminology translation services
• Translation to HITSP specified
terminology
• CPP for consumer permissions &
enterprise policies
• Will enforce authorization, auditing,
authentication
63
Copyright 2009. All Rights Reserved.
•
Patient demographics
•
Clinical data
• Separate interface for document
storage subsystem
• Separate interfaces for enterprise
services, e.g. audit logs, system
monitoring
Technical:
Content Payload
VA and KP
HITSP C32 patient health summary
• Version 2.1 - Minimum data set
• Personal information
• Contacts
• Allergies
• Medications
• Problems
• Source of information
All required data elements in the
specified HITSP terminologies to the
extent possible, others optional
(pending NHIN certification criteria)
64
Copyright 2009. All Rights Reserved.
Policy:
DURSA
VA and KP
• 2008 test patient data
DURSA signed
• 2009 live patient DURSA finalized/
in clearance, and under review by
VA and KP management
• DURSA overview (plain English)
available
65
Copyright 2009. All Rights Reserved.
Policy:
Shared Patient Population in the
San Diego Area
VA and KP
• Oversight by our legal and privacy officers
• Analysis indicates approximately 1400 patients
• seen within last year at VA
• a standing appointment for next year
• With a secondary insurance indicating KP
• No sensitive diagnoses
• Confirmation of the list of potential shared
patients among our two organizations is
working its way through permissions to share
66
Copyright 2009. All Rights Reserved.
Operational:
Patient Consent
VA and KP
• Emulating existing manual/paper workflow
•
•
•
•
1 letter
2 authorizations
1 return envelope
1 help desk
67
Copyright 2009. All Rights Reserved.
• Processing of return envelopes at local San
Diego VAMC
• Final workflows subject to approval
Operational:
Authority To Operate
• VA
• KP
• VA has formal process for
certification and accreditation
• KP not subject to internal federal
agency requirements
• 600 Enterprise Requirements
reviewed to assess which ones
apply to VA NHIN solution
• KP process addresses similar
points somewhat differently
• Document compliance traceability
• Design reviews
• Project reviews
• Requirements analyses and
documentation
• Solutions analyses and
documentation
68
Copyright 2009. All Rights Reserved.
Operation:
VA-KP Schedule
Item
Title
KP date
VA date
Agreed date
-
6/12
6/12
1
VA and KP validate initial shared patients under active care
2
Forms and letter defined
6/19
6/19
6/19
3
Patient authorization processing process defined
6/26
6/26
6/26
5
VA and KP validate final shared patients under active care
7/03
-
7/03
7
Gateway 2.1 certification by NHINC (connection to FHA) soap 1.2
-
7/17
7/17
8
Regression test of KP/VA CCD exchange across NHIN soap 1.2 complete
7/15
7/20
7/20
9
Forms and letters ready for mailing
7/24
7/24
7/24
11
KP/VA doc exchange across NHIN Kaiser C32s generated on demand
6/30
7/29
7/29
12
Patient authorizations mailed
7/31
7/31
7/31
13
KP/VA subject discovery inter-gateway integration test complete (using test
patients from forum)
8/14
8/14
8/14
14
San Diego face-to-face demos with KP and VA local clinical staff
8/24
8/24
8/24
15
End-to-end integration test complete (using test patients)
8/28
8/28
8/28
19
Patient authorization returns processing complete
TBD
TBD
TBD
21
Pre-prod verification of both KP and VA environments (setup for UAT)
TBD
TBD
TBD
22
Deployment to production
TBD
TBD
TBD
23
KP/VA UAT begins (end-to-end using shared patients that opted-in*)
9/28
TBD
TBD
24
KP/VA GO LIVE (Full Deployment)
TBD
TBD
TBD
69
Copyright 2009. All Rights Reserved.
Operational:
Local Sites Involvement
• VA
• KP
• San Diego VA Medical Center &
Clinics
• San Diego KP Medical Center &
Clinics
• Support from Chief of Staff and
Director of informatics
• Assist with patient consent
• Assist with clinicians training (little
training required as same GUI is
used to access remote VA sites or
NHIN ‘sites’)
70
Copyright 2009. All Rights Reserved.
• Support from Assistant Medical
Director, Chief Medical Information
Officer and Regional Director KP
HealthConnect, local physician lead
• Clinician involvement in screen
design
• Assist with patient consent
• Assist with clinicians training
Operational:
Measures of Success
VA
KP
• Pilot in San Diego must help
refine national rollout plan
• NHIN membership
• Usage metrics will be
incorporated in software
• Patients count
• Pilot in San Diego will inform
national rollout plan
• Measures under development
•
Care Quality
•
Clinical Workflows
• C32s content stats
•
Financial
• Impact on workflow
•
Other
• Clinicians count
• C32s exchanged count
• Impact on quality
• Cost of system
71
Copyright 2009. All Rights Reserved.
Operational:
NHIN/FHA Support
VA and KP
• NHIN participation
• Varying roles:
• HITSP, IHE, SDOs;
• NHIN (spec factory/testing criteria);
• NIST (tools);
• CCHIT
• NHIN Cooperative workgroups
• DURSA, Specification Factory,
Testing, …
• NHIN/ONC/FHA staff support
• Vanessa/Virginia, Craig/Dave,
Mariann/Jeff, etc.
72
Copyright 2009. All Rights Reserved.
Operational:
Stakeholders Buy In
VA
KP
• Presentations and
demonstrations
• Senior leadership support
• VSO, IDMC, CPRS WG, etc.
• Regular stakeholders status
report
• Business, clinical, and
technical staff kept informed
from national office and local
San Diego VAMC
• CIO, CEO, SVP’s
• Physician leaders
• Presentations to Regional
Operations staff & managers
• Governance groups
• IT
• Business
• Clinical
73
Copyright 2009. All Rights Reserved.
Next Steps:
VA and KP
TESTING & CERTIFICATION
Limited Production Roll Out in San Diego
Training and Communication
Measurements
Lessons learned
SECOND, THIRD, … ADDITIONAL SITES
SCALABILITY PLAN – TOWARD NATIONAL RELEASE
74
Copyright 2009. All Rights Reserved.
Contact Information
VA contact
KP contact
Tim Cromwell, RN, PhD
Jamie Ferguson
Director, Standards & Interoperability
Executive Director, HIT Strategy & Policy
Office of Health Information
Jamie.Ferguson@kp.org
Tim.Cromwell@va.gov
510-271-5639
801-588-5022
75
Copyright 2009. All Rights Reserved.
CONNECT Seminar
Presentations are Available
for Download Online at
http://www.connectopensource.org
76
Copyright 2009. All Rights Reserved.