Capnography: The Window Into Your Patient
advertisement

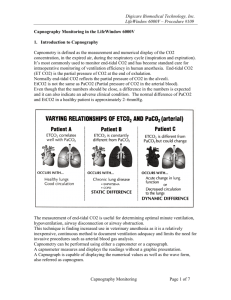
Capnography: The Window Into Your Patient Talk Code 682 Mike McEvoy, PhD, RN, CCRN, REMT-P Senior Staff RN – Cardiothoracic Surgical ICUs – Albany Medical Ctr EMS Coordinator – Saratoga County, New York EMS Editor – Fire Engineering Magazine EMS Director – New York State Association of Fire Chiefs mikemcevoy.com SpO2 versus EtCO2 Physiology Oxygen lungs alveoli blood Oxygen breath CO2 muscles + organs lungs Oxygen CO2 energy blood CO2 cells Oxygen + Glucose Contrasting Pulse Ox with Capnography Pulse oximetry measure oxygen going OUT from the heart Capnography measures what is coming BACK from the periphery Two Different Concepts Oxygenation and Ventilation Oxygenation (Pulse Ox) – O2 for metabolism – SpO2 measures % of O2 in RBCs – Reflects changes in oxygenation within 5 minutes Ventilation (Capnography) – CO2 from metabolism – EtCO2 measures exhaled CO2 at point of exit – Reflects changes in ventilation within 10 seconds What is Capnography? • “Capnos” = Greek for smoke – From the “fire of life” metabolism – CO2 is the waste product of metabolism • Carbon Dioxide is a compound molecule – 2 oxygen + 1 carbon – Odorless; heavier than atmospheric air – Green plants scavenge excess CO2 – 0.03% concentration in room air – Resting adults produce 2.5 mg/kg/min Capnography Basics Carbon Dioxide (CO2) – Produced by all living cells – Diffused into the bloodstream – Transported to the lungs – Perfused into the alveoli – Exhaled through the airway Measuring Exhaled CO2 Colorimetric Capnometry Capnography Measuring Exhaled CO2 Colorimetric Capnometry Capnography Measuring Exhaled CO2 Colorimetric Capnometry Capnography Waveform Capnography • Available for spontaneously breathing and for intubated patients Capnography is the window INTO the patient Normal Capnography Waveform 45 0 • Normal range is 35-45 mmHg • Height = total CO2 • Length = time/rate Capnogram Phases C A B D End-tidal E Inhale Capnogram Phases C A B D End-tidal E Exhale (dead space) Capnogram Phases C A B D End-tidal E Exhale (rapid rise) Capnogram Phases C A B D End-tidal E Exhale (plateau) Capnogram Phases C A B D End-tidal E End of the wave of exhalation How Capnography Can Help • Airway • Breathing • Circulation What Happened? The endotracheal tube became dislodged! Apnea Airway Obstruction Displaced airway (esophageal) Airway or vent disconnection Vent malfunction Cardiac Arrest What about the Pulse Ox? Sp02 98 Normal: Esophageal tube: Breathing Capnography Waveforms 45 Normal 0 45 Hyperventilation 0 45 0 Hypoventilation Rebreathing Possible causes: Faulty expiratory valve Inadequate inspiratory flow Breath stacking (wrong mode, undersedated) Malfunction of CO2 absorber system What’s the SHAPE? The Shark Fin Possible causes: Partially kinked or occluded artificial airway Presence of foreign body in the airway Obstruction in expiratory limb of vent circuit Bronchospasm Bronchospasm (asthma) Mild Moderate Marked bronchospasm Airway: Leaking tube cuff “Curare Cleft” Appears when NMBAs begin to wear off Depth of cleft inversely proportional to degree of blockade Circulation The lungs and the heart are inextricably tied together CO2 clearance reflects perfusion In other words: CO2 production is largely dependent on oxygen consumption! Cardiac Arrest • Little O2 delivery or consumption • Little CO2 production or venous return …Little Need to Ventilate! 1. Use EtCO2 as guide to avoid overventilation during resuscitation: < 20: slooooow down > 40: increase breaths 2. Increased CO2 may = ROSC Decision to Call the Code • 120 prehospital patients in nontraumatic cardiac arrest • EtCO2 had 90% sensitivity in predicting ROSC • Maximal level of <10mmHg during the first 20 minutes after intubation was never associated with ROSC Source: Canitneau J. P. 1996. End-tidal carbon dioxide during cardiopulmonary resuscitation in humans presenting mostly with asystole, Critical Care Medicine 24: 791-796 What about other shock states? “These data suggest that respiratory rate alone cannot be used to predict measured capnography levels.” R. Fowler, P. Pepe September, 2007 Wide a-A gradient: EtCO2 = 11 PaCO2 = 28 Something is blocking gas exchange: • Pulmonary embolism • PNA, ALI or ARDS • Shunting • Low CO state • Very low HCO3 Test: your patient is seizing Thank You ! Talk Code: 682