July 8th Recording Presentation

ICRA AND CONSTRUCTION
Infection Control Risk Assessment
FIRST, DO NO HARM!
We are the patient Advocate!
What is an ICRA?
• It is a strategic proactive multidisciplinary organizational process to show you are considering the patient population and the potential Construction, renovation and demolition may have on patients and employees in the healthcare environment. A group should discuss this process, including
Infection Control, Engineering, the Construction group,
Safety officer, and Administration to come up with a plan.
• ICRA involves a matrix that allows you to assess how a construction project may effect the facility varying with degrees of activity versus the type of exposure risk potential for varying patient population types. This will determine the type or degree of intervention and mitigation that should happen to keep patients and employees safe. The goal is to reduce risk of infection, coordinate mitigation of potential exposure, and to establish expectations of the Construction group while they are inside your facility.
Who Recommends an ICRA
• CDC (Centers for Disease Control and Prevention)
• HICPAC (Healthcare Infection Control Practice Advisory Committee)
• APIC (Association for Professionals in Infection Control and
Epidemiology)
• AIA (American Institute of Architects)
• ASHRAE (American Society of Heating, Refrigeration, and Air
Conditioning Engineers)
• ASHE (American Society for Healthcare Engineering)
• NIOSH (National Institute for Occupational Safety and Health)
• FGI GUIDELINES (Facility Guidelines Institute)
• US Department of Health and Human Services
• The Joint Commission
• And Washington State Department of Health
….. to name a few…..
Infection Preventionists must be involved in the process
• The risk of exposure to the patient must be understood and considered.
• Avenues of mitigation of dust, looking for disturbances in air flow, and awareness of molds and water bugs that others might not consider are prominent.
• Disruption of essential services must be minimized with planning. Changes in traffic flow may help.
• Normal patient population and disease prevalence are known to IP’s.
• IP’s are focused on prevention of cross transmission and are proactive involving Environment of Care with isolation and containment in their every day duties.
How to use the ICRA
• Gather all the parties for the project in a meeting and have them all go over the assessment together.
• Once decisions are made about the Type of
Construction and Patient Risk, then the Matrix is used to determine the Class of Precautions necessary.
• Once the Class is determined, plan and agree what types of mitigation should be implemented for the phases of construction, and any other needs that will arise.
• Last, fill out a permit and have all parties initial and sign it. Review this often as meetings progress in the construction. This is only necessary if its determined the construction project is type III or type IV.
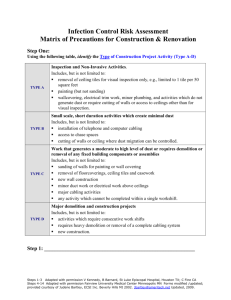
Step One- Type of Construction
What type of activities are going to be needed during the Construction
Project?
Type A - Inspection and Non invasive activities.
(individual ceiling tile removal, painting, electrical trim work, very little dust)
Type B – Small scale short duration creating minimal dust.
(installation of wires and cables, crawl spaces, cutting of walls and ceilings where dust can be controlled.)
Type C- Work with moderate to high levels of dust and demolition or removal of fixed building components.
( sanding of walls, pulling up floors, new wall construction, duct work above ceilings, major cabling or anything that may not be completed in a single shift.)
Type D – Major demolition and construction projects.
(activities with consecutive work shifts and requires heavy demolition, removal of cables, or new construction)
Step Two – Patient Risk
Determine how patients will be affected
-Low Risk – office areas, minimal patient traffic, no healthcare supplies are kept.
-Medium Risk- Ambulatory patients, for Physical Therapy, Radiology,
Respiratory Therapy, Cardiology, Non Immunocompromised.
-High Risk – ER, Labor and Delivery, Laboratory, Medical Units,
Outpatient Surgery, Surgical units, Pharmacy. Acutely ill patients at risk for contracting illnesses or facing breathing hardships.
-Highest Risk – Immunocompromised patients, Burn Units, Cardiac Cath
Lab, ICU, Sterile Supply, Oncology, Operating Room. Seriously ill patients who should not be exposed .
Use the Matrix to determine the Class
• Class I- minimize dust, one ceiling tile at a time
• Class II- prevent dust dispersion, mist to control dust, seal unused areas with Duct Tape, block vents, sticky mats, turn off or isolate HVAC in areas of construction
• Class III- remove or isolate HVAC so the system won’t be contaminated, create and seal barriers, HEPA vacuum, filtered air, negative pressure, cover transport carts
• Class IV- isolate HVAC, create and seal barriers, vacuum and filter air, negative pressure seal holes, create an anteroom for workers to be vacuumed with a
HEPA filter, require PPE, Shoe covers donned and doffed when entering and leaving work area.
Step 4 through 8 - Questions
4. Questions about adjacent areas to construction to assess impact. Do they need to be considered?
5. Type of area under construction (patient room, med room, etc.). Each area could need different treatment.
6. Identify areas of ventilation, plumbing and electrical power outages as a potential. Preparedness is key.
7. Identify containment barriers such as solid walls, and will HEPA filtration be required? The construction should be isolated from occupied areas and should be negatively pressurized
8. Is there risk of water damage or compromising structural integrity of walls, ceiling or roof?
Step 9 through 14 – Questions
9. Is it possible to complete this during non-patient care hours?
10. Do plans allow for an adequate number of isolation or negative airflow rooms? May just do a little at a time.
11. Do plans allow for the required number and type of Hand washing sinks? Hand Hygiene can’t be compromised.
12. Does IC agree with the minimum number of sinks for this project?
13. Does IC agree with plans relative to clean and soiled utility rooms? Storage in areas may need to be altered.
14. Discuss containment issues with the project team, such as traffic flow, housekeeping and debris removal.
Does an ICRA form need to be signed?
Once all parties feel the whole project and potential have been discussed, was a Class III or Class IV determined to be the case?
If so, signatures should be obtained and the paperwork should be kept on file.
Infection Control and other members of the committee should help do periodic surveillance of the construction area to ensure compliance with the established plan.
Focus of the ICRA
• Design – project planning for the IC future
• Mitigation – knowledge of barriers and isolation
• Airflow – pressure needs and requirements are considered.
• Water- Knowledge that disruption of the system allows for microbe entry, and stagnant water leads to biofilm buildup
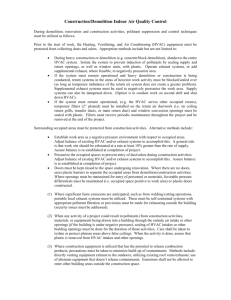
Clean Up is Important
• Carry out waste in covered bins.
• Waste must be addressed every day of the construction project, as well as after it is completed.
• Construction crews better understand their role in this area, it is not up to your housekeeping to clean up their mess.
Why is Construction the norm ?
• Who doesn’t want a fancy shiny new hospital? If its new equipment, the care is better isn’t it? Expansion.
• Baby boomers, aging and acuity changes. More of them to care for, so are we equipped to handle them?
Decentralized nursing stations to be closer to patient rooms and affecting the care the patient recieves.
• Single occupancy rooms are better for Infection Control needs, less contamination, bathroom in the room, sink accessible only to those in room, patient sleeps better, etc. Patient Centered Care in acute care settings now finds ways to accommodate families and visitors.
• Surge capacity indicates rooms should have multiple uses, so new equipment must be brought in are there enough amenities for two in each room if needed?.
What does technology bring?
• New technology is needing requirements. WIFI and Cable in rooms now, Patient Portals to look at their health records.
• Sustainability programs and “going green” have effected Healthcare. Grants are available if designed to improve efficiency of heating, ventilation and air flow.
• LEAPT, LEAN and Six Sigma methods and principals trying to create maximum value and reducing waste through improved quality, efficiency and safety.
New ideas – are they good?
• Sink basins, should be to where they don’t splash, and water should not hit directly on the drain.
• Automatic sinks- is the temperature and water pressure correct? Will it have enough force to wash contaminants down the sink?
• New flooring and finnishes – are they compatible with hospital grade cleaners?
Wrap Up
• Get involved with new construction, in the planning and execution of it. Take authority.
• Know your patient population, and how the needs of your facility may be different then the last hospital the construction crew worked.
• Be prepared to change plans at any time.
• Do surveillance, make yourself known.
• Remember, patients and safety come first!
Any Questions or Comments?
Tara Dockery, MT (ASCP), IP, BS
Infection Prevention Consultant
TaraD@wsha.org