Common Pediatric Psychiatric Presentations to the Emergency Room.
advertisement

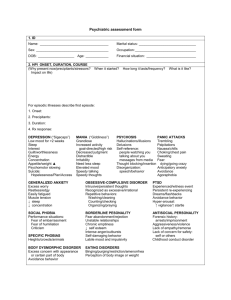
Common Pediatric Psychiatric Presentations to the Emergency Room. Zaid B. Malik, MD Asst. Professor Director C&L Asst. Residency Program Director. Child psychiatric emergencies presenting in the hospital setting are most often characterized by intense symptoms, perceived danger, and a sense of urgency complicated by the perception of imminent catastrophic outcome and frequent conflict among the parties involved. Despite this acuity, child psychiatric emergencies are usually the outcome of complex, ongoing processes rather than sudden, discrete events. (this is true most of the times) Occasionally, a previously well functioning child with some underlying vulnerabilities may abruptly decompensate and display psychiatric symptoms in the presence of some critical or traumatic event or organic process. The goal of child psychiatric emergency services evaluation is then to clarify the nature and the cause of the imbalance that has arisen and to identify the resources needed (safe environment, psychoeducation, psychopharmacotherapy, outpatient therapist, family support services) to restore equilibrium. The primary goals of the child psychiatric emergency evaluation are, as expeditiously as possible: To obtain each informant's account of the reason for referral To develop a working alliance, if possible, with the patient and other involved parties around the assessment and disposition planning To obtain a focused developmental history of the child's current difficulties and prior functioning against the backdrop of the child's family, current living situation, and any involved clinicians or agencies, with particular attention to the possible precipitants of the current crisis To perform a mental status examination, with particular attention to evidence of suicidal or homicidal ideation, hallucinations, delusions, or thought disorder; evidence of confusion, disorientation, or other signs of delirium; and intense anxiety To develop a differential diagnosis, including a formulation of what changing factors have precipitated the need for emergency evaluation at the present time To arrive at a judgment regarding the degree of probable risk to the patient's safety or that of others To identify interventions that will help to contain and ameliorate the patient's difficulties To plan and implement a disposition To collaborate effectively with other clinicians and care providers involved in the case, both within and beyond the hospital setting The clinician must be alert to and explicitly note the presence of the following: Disorientation, confusion, and fluctuating levels of consciousness Incoherence of thought or speech Evidence of hallucinations or delusions Impaired memory Slurred speech, ataxia, or apraxia Assessment of safety additionally requires explicit attention to the following: The presence of suicidal or homicidal ideation Aggressive threats or ideation Impulsivity Proneness to regression or agitation during the interview Poor judgment and insight and limited intelligence Mood lability Case 1 CJ was a 5 year old who had just started KG. He had no experience with preschool and had never been away from home in a group situation. He presented to an outpatient psychiatry clinic after hitting his teacher and biting the principal. No history of previous evaluation or treatment of developmental, behavioral, or emotional disorder. He was healthy and active. His mother had moderately severe anxiety disorder and stayed mostly at home. He lived with his father, mother and older brothers. On MSE he was a small, compliant child with poor eye contact. He responded to questions with monosyllables that were hard to hear. Case 2 ST was a very bright 12 yr old twin. He presented to a residential treatment unit with a history of severe aggression and rages at home and school when he did not get his way. His ability to tolerate frustration varied considerably; at times he was able to accept limits and consequences; at other times he would become explosive, hyperactive, and destructive. His family was not able to go into public spaces for fear that he would become angry. He had been treated for ADHD and ODD since early childhood. He was healthy, without chronic illness and although a twin his pregnancy and perinatal history was unremarkable. On MSE, he was a well developed 12 yr old with poor eye contact. He was sulky and irritable with angry affect. Family history was positive for bipolar disorder. His parents were divorced due to his father’s mood instability. He was being reared in a single mother household. His mother was genuinely frightened of his rages. Case 3 HJ was a developmentally delayed 7 year old with an IQ of 60 and a diagnosis of autism. When frustrated he had a history of aggression with peers, caregivers and himself (head banging and biting his forearm until it bled). He was rigid with poor tolerance of over stimulating environments and transitions. He lived with his mother and father in an intact home and attended a behavioral classroom in a public school. Case 4 LC was a 10 yr old boy in a single mother household presenting at the insistence of the school. His academic and behavioral problems at school started in KG. Behaviors included fighting, talking back, vandalism, lying, truancy, and stealing from other students. He was diagnosed with ADHD in KG and had been treated with psycho stimulants off and on since then. He did not know his father. Throughout his childhood his mother’s boyfriends moved in and out of the house. He had little supervision or monitoring. Discipline at times was excessively harsh. The family had had involvement in the Department of Children and Family Services before following a substantiated case of physical abuse. Family history was positive for substance abuse, depression, and poor anger management. Differential Diagnosis of Aggression Symptoms of Aggression are common in a wide range of psychiatric conditions. – – – – – – – – Conduct Disorder Oppositional Defiant Disorder Mood Disorder ADHD Anxiety Disorder Psychotic disorders (especially those including paranoia) Developmental Disorders Anxiety Treatment Options Medications – – – – Antipsychotics Mood stabilizers Serotonin Reuptake Inhibitors Stimulants Case 5 A. 16 yr girl, considered generally well adjusted, without psychiatric history presents to the ED at 11p. She is drowsy and nauseated. Her mother says that her daughter has been seeing a boy for the past 2 years. He broke up with her last week. Since then she has been sad and tearful, uninterested in her usual activities. Tonight, after seeing her ex-BF at a restaurant with another girl. She came home and took a bottle of aspirin. An hour later she came to her mother and told her what she had done. Family history is negative for psychiatric illness and completed suicide. On MSE she is sleepy and feeling sick. She denies longstanding depressive symptoms and says that she does not want to die now. She says that she never wanted to die but wanted people to understand how sad she is. She also said that she hoped her BF would come back to her. Case 6 MH A seventeen year old boy, who recently graduated from HS, is found barely conscious in his bedroom by his mother when she goes in to wake him up. She takes him to the ED where a tox screen reveals that he has taken an overdose of Depakote. The Depakote was his mother’s. On the floor he is extremely quiet and uncommunicative. He says that he wants to go home. There is no previous psychiatric history but his mother says that he has been “acting different for the past year”. He has been staying in his room with less and less interest in doing things with friends. She is not aware of any traumatic events. There is a family history of schizophrenia. This patient has no past psychiatric history. On interview he is quiet with a blunt affect. He denies any problems, cannot explain his overdose, but feels that he has to get out of the hospital b/c the people there are getting on his nerves. He denies AH but is suspicious and guarded when questioned about them. He does talk about his graduation ceremony and says that when he walked across the stage the other students laughed at him. When asked about that his mother says that that did not occur and he has always been well-liked at school. Leading Causes of Death in 15-19 Year-Olds Accidents Homicide Suicide Cancer/Leukemia Heart Disease Congenital Anomalies (NCHS 2001) 12-Month Prevalence of Suicidal Ideation and Behavior U.S. High School Students- Youth Risk Behavior Surveillance CDC 2000 Ideation 17-19% Ideation w/ plan 11-14% Attempt 5-8% Attempt requiring 1-3% medical attention Suicide (age 15-19) .008% 2.7 million 1.9 million 1.0 million 296,000 1,600 Ratio of Teen Attempts to Teen Suicides Deaths* Attempts* Ratio Males Females YRBS CDC 2000 14 all numbers/100,000 3 5,700 10,900 1:400 1:3,900 Suicide Methods United States 1999, 15-19 Year-olds Firearms Hanging/Suffocation Ingestions CO poisoning Jumping In 1998 suicide rates were highest among white males of all ages, followed by nonwhite males, white females, and non-white females. Biological factors Low Serotonin levels Genetic Predisposition Types of Stress Events Preceding A Suicide Disciplinary Crises 48% Relationship Problem 36% Humiliation 16% Most Common Teen Suicide Diagnoses ANY Mood Disorder Antisocial Disorder Substance Abuse Anxiety Disorder Shaffer et al 1996, Brent et al 1999 MALE 50% 43% 38% 19% FEMALE 69% 24% 17% 48% Imminent Risk in Suicide Attempters Agitation Intense Anxiety Recent Discontinuation of Medications High-Risk Attempters Male Abnormal mental state Previous attempt Family history of suicidality History of aggressive outbursts and substance and alcohol abuse Method other than ingestion Clinical Risk Factors 1/3 of Teenage suicide victims have made a previous attempt ½ have persistent thoughts of hopelessness Aggressive/impulsive behavior is increased in both sexes ½ of teenagers who commit suicide have had contact with a PCP or MHP Clinical risk factors (continued) Alcohol and cocaine abuse are present in 2/3 of 1819 year old males but uncommon in younger males and females Schizophrenia and bipolar illness each represent fewer than 10 % of suicides but are relatively infrequent conditions Increased Frequency of suicide attempts and completions in relatives of suicide victims Decreased family support Emergency Room Management of the Suicidal Adolescent Medical Care To Admit or not to admit Sedation ?? Contract for Safety Hospitalizing a Teen Attempter Sufficient – – – – Medical Necessity Abnormal Mental State Persistent Wish to Die Highly Lethal or Unusual Method Hospitalization (continued) Adds weight but not Sufficient – – – – – Prior Attempt(s) Male gender Family history of suicide Inadequate care and supervision at home Over age sixteen Contract for Safety Thought to improve compliance Thought to reduce likelihood of further suicidal behavior A probe to assess patients willingness to assist in treatment efforts No evidence for any of the above. Etiology Suicidal Behavior is complex. The factors involved are outlined in accordance with five axis. Primary psychiatric disorders Developmental and personality disorders Biological factors Stress Social functioning It is important to assess and document the following in the child or adolescent: The degree of premeditation and planning versus impulsiveness (22) Ego syntonicity or dystonicity Consistency with the patient's past behaviors or style (including chronic bullying) Extraordinary or uncontrolled rage and use of weapons The validity of perceived self-defense Evidence of grossly impaired judgment or consciousness Bizarre or delusional behavior or thought content Risk of self-injury during the violent episode The extent to which the child can remember the details of the episode (including his actions and their consequence), accept responsibility, or express remorse Conclusion: