Substance use disorders prevention & treatment among - MI-PTE
advertisement

SUBSTANCE USE DISORDERS
PREVENTION & TREATMENT;
THE ARAB AMERICAN COMMUNITY
12TH ANNUAL SUDS CONFERENCE
Ms. Manal Said, MSW, ICPS, CPC -R, Coordinator, Substance
Abuse Prevention Program
msaid@accesscommunity.org
Dr. Hakeem Lumumba, Ph.D., CAADC, CCS -M, LPC, LMSW,
Behavioral Health Director
hlumumba@accesscommunity.org
Arab Community Center for Economic & Social Services (ACCESS)
Community Health and Research Center
Maslow Hierarchy of Needs
• Please see handouts
Erickson’s Human Development
• Please see the handouts
The Arab American Community…
• Arabs and Chaldeans Defined
Who are Arabs?
•
•
•
•
US Citizens
Permanent residents
Middle-Eastern ancestry
Shared cultural heritage
Arab Ancestry in Michigan
Who Are Chaldeans?
• The history of Chaldeans can be traced to at least
the 13th centuries B.C.E. in what is now known as the
first Mesopotamia civilization. Mentioned in the
Hebrew Bible.
• A prominent city of the Chaldeans, called Ur, is the
historic homeland of the prophet Abraham
• Chaldeans belong to the Chaldean Catholic Church
which in the 15th century aligned with the Roman
Catholic Church. However, they have their own
Patriarch and the Eucharist (ordinance) differs.
Chaldean Americans
• Chaldean Americans are descendants of the
northern Tigris-Euphrates Valley, located in Iraq. Not
all Chaldeans are Iraqis and not all Christian Iraqis
are Chaldeans.
• In Iraq, there are multiple ethnicities.
• In Iraq, Chaldeans are not well known or identified.
• Chaldeans are believed to have immigrated to the
United States as early as 1880
• The majority live in Detroit, Michigan. It is
estimated that there may be as many as 150,000
Chaldeans in the metropolitan area.
• Mostly reside in Macomb and Oakland counties.
• Chaldeans prefer being called Chaldean Americans.
Chaldeans cont.
Assyrians
• Indigenous to Iraq, Syria & Iran
Kurds
• Indigenous to Iraq, Syria, Turkey & Iran
Berbers
• Indigenous to Morocco, Algeria, Tunisia & Libya
Arab Countries
Different waves of
immigration to the U.S.,
dating back to the late
1800’s
Recent waves include
refugees from violence
Highly concentrated in
metropolitan areas
Waves of Arab Immigration
• First Wave (1880s-1920s)
• Mostly single, Christian men from Greater Syria
• Came looking for jobs
• Second Wave (1950s-1960s)
• “Brain-drain phenomenon”
• 1948 and 1967- Palestinians emigrated because of
political conflict
• Third Wave (1970s-Present)
• War and political conflict
1975- Lebanese Civil War
1970s/1980s- Palestinian/Israeli wars
1980- Iran/Iraq War
1991- Gulf War
2003- War in Iraq
Some Demographics
• In all 50 States
• 2/3 in ten States
• 1/3 live in Michigan, California & New York
• 94% live in Metropolitan areas
• California has largest Arab population
• Michigan has largest concentration of Arabs
Language
عربي
• Arabic
• Several dialects
• Official language of 21 of 22 Arab countries
• Spoken by 92% of the population
•
•
•
•
•
•
English
French
Aramaic
Kurdish
Berber
Armenian
Second Language at Home 2003
Religion
• Most Arabs are Christians
• Varies by region
• Islam
•
•
•
•
Sunni
Shi’a
Belief in Allah
5 pillars of Islam
• Judaism
• Druze
Arab Religion 2003
Family
Culture
• Customs
• Clothing
• Food
Terminology
• Arab, Arabic or Arabian
• Arab American or American Arab
• Muslim or Moslem
• Middle East vs. the Arab World
Stereotypes
• Islam as violent or unfair religion
• Arabs/Muslims are terrorists
• Eye charm used as witchcraft
(hamsa) {WORN FOR PROTECTION}
• Arab women subservient to men
• Arabs are oil rich
• All Arabs are Muslim
• Arabs don’t speak English & uneducated
Arabs/Chaldeans: Acculturation
• Gender differences women more vulnerable
• Religious differences
• Loss of the family unit & role reversal
• Discrimination
• Racial profiling post 9/11
• Generational gaps 1st, 2nd & 3rd
• Marginalization
Prevalence of Substance Abuse
Smoking rates among Arab American
Adolescents (14 -18 yrs)
100%
80%
60%
Cigarette
40%
Arghile
20%
0%
Tried smoking Smoked in Smoked Daily
past 30 days
Binge Drinking Indicate Need for Culturally-specific Interventions
*
* p<.05
Michigan BRFS, 2007-2009
Arab Americans entering substance abuse
treatment over time, Michigan
0.5
FY 2007 had 62% increase over FY 2001
Race of Arab American
% of total admissions
0.4
0.3
Ethnicity of
Arab/Chaldean
168
187
201
2002
2003
2004
222
246
223
2006
2007
138
0.2
0.1
59
0
2000
Fiscal years
2001
2005
Numbers of admissions by Arab Americans noted above the bars.
Social Consequences
• Perspectives
•
•
•
•
Legal
School
Religious
Family
Arab American Youth
Immigration & Acculturation
• Immigration involves psychological stress &
loss
• Acculturation
1. 1st generation – grieve losses while
adjusting to new country and environment
2. 2nd generation – emotional turmoil & family
conflict due to difference in parent-child
assimilation levels
3. Since 9/11, 3rd and 4th generation Arabs
reconnect to Arab culture & ancestry and
preservation of cultural identity
Arab American Youth
Trauma & Arab American Youth
• Immigration as a result of war &
displacement
• Possibility for self-medicating through drugs
or alcohol
• Parental Trauma makes parents emotionally
unavailable to their children → negatively
impacts the youth and creates instability
Stigma
Cultural stereotypes and family honor
Mental illness sometimes seen as sign of
punishment from God
Mental illness considered by some as
possession by Jin (devil)
Belief that the mentally ill are dangerous,
unpredictable and untreatable
Hard to communicate or work with and
hopeless
Effects of stigma
• Research shows that stigma of mental illness, can be as
•
•
•
•
•
•
harmful as the illness itself.
It may aggravate or increase symptoms.
It diminishes social and work functioning.
It depletes support networks and increase isolation in the
community.
It reduces chances of marriage or healthy relationships.
May even cause divorce or family destruction.
It reduces chances of getting jobs.
Shunned by community.
Prevention Methods
ACCESS Substance Abuse Prevention Program
• Environmental and Community Based Strategies
•
•
•
•
•
Advocacy and policy change- legislator education
Vendor education and compliance checks
Provide bilingual educational community & school presentations and technical assistance
Life skills curriculum
Bilingual printed informational material
ACCESS Community Substance Abuse Coalition (ACSAC)
• Coalition capacity building
• Provides forum for community stakeholders to share resources and information
Primary focus on Hookah and Tobacco Prevention
• Second-hand smoke exposure
•
Smoking cessation
Goals
• Increase awareness, change community norms and reduce accessibility
HOOKAH
ARGILEH
• Hookah aka, Argileh or Shisha, is
a single or multi-stemmed (often
glass-based) water pipe for
smoking flavored tobacco.
• It has a long hose attached to the
pipe from which the smoke is
drawn. The charcoal is used to
heat and smoke the tobacco.
When the smoke passes through
the water it cools smoke of
tobacco.
Flavored moist Hookah tobacco
Some Concerns…
• Misperception that carcinogens are filtered during the
smoking process
• Many do not consider themselves as smokers if they
only smoke hookah
• Many view it as a social activity, non addictive and not
as harmful.
• Hookah is normally shared and poses sanitation
hazards i.e. TB, H1N1, Herpes exposure
• Social acceptance of smoking hookah is high.
• Able to resist smoking for longer periods of time when
they are in an environment where smoking is not
allowed
• Family and guests smoking in the home and offered as
sign of hospitality contribute significantly to the
smoking behavior
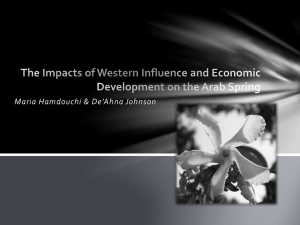
Current hookah smoker by gender among Arab & Chaldean compared to non
Arab Americans
60%
A&C Americans
Comparison group
50%
41.6%
40%
33.6%
30%
24.7%
20%
10%
3.2%
1.9%
2.5%
0%
Male
Female
Total
DSM-IV Definition of Substance Abuse and
Chemical Dependency
• Substance Abuse-A Maladaptive Pattern of Substance Use
Leading to Clinically Significant Impairment or distress as
manifested by one or more of the following within a 12 month
period, poor performances at work, with family and school,
high risk behaviors (driving under the influence), legal
encounters, and the inability to stop despite negative
outcomes
• Substance Dependence-Maladaptive Pattern of Substance
Use, Leading to Clinically Significant Impairment or distress, as
manifested by either tolerance, withdrawals, abuse, inability
to control use, or preoccupation to obtain substance(s) (APA,
2000)
DSM-IV Co-Occurring Disorders among Arab
Americans and Chaldean Americans
•Besides Opiate Addiction, Cocaine Addiction,
Sedative Addiction, Marijuana Addiction, and
Tobacco Dependency, many members of this
group also suffer from Bi-Polar I and II
Disorders, Anxiety Disorders (PTSD, Panic
Attacks), Major Depressive Disorders, and
Adjustment Disorders with Mixed Anxiety and
Depression
DSM-IV Co-Occurring Disorders among Arab
Americans and Chaldean Americans
• Sexual Abuse, Paranoid Personality Disorder,
Paranoid Type of Schizophrenia, and Bereavement.
Treatment Methods
• Engagement Techniques-There needs to be a sensitivity to the
client’s need to feel safe. The Arab American and Chaldean
American Communities are very closed knitted community and the
concern for strict confidentiality is of the utmost importance.
• Language Barriers-There is a preference for the health care
provider to be bilingual (English and Arabic), depending upon if the
client is a member of the first, second, or third generation.
• Family/Couple Therapy-is important, however, it maybe difficult to
include the husband. Many men in the Arab American and Chaldean
Communities are entrepreneurs and may not be available. In
addition, depending upon certain Arab Americans, the man is
viewed as the ultimate authority. Therefore, it is essential to keep
the father or male guardian in loop of the therapy
Treatment Methods continue
•Psycho-Education-There needs to be an
emphasis on educating the client on the
purpose of therapy. Many Arab Americans and
Chaldean Americans have never engaged in
therapy, so therefore, there maybe a high level
of apprehensiveness. In addition, the client
may need to be educated on the difference
between a Psychiatrist, Psychologist, Social
Worker, and Counselor.
Theoretical Models
•Affective Intervention Model-This model
stresses the importance of feelings, more
importantly the sorting out of feelings.
•Cognitive Intervention Model-This model
stresses the importance of the thought
process and the client’s belief system.
Theoretical Model continue
•Behavioral Intervention Model-This model
stresses the importance of assisting the client
with identifying their maladaptive behaviors as
well as their adaptive behaviors. In addition,
this model stresses identifying the enforcer of
certain behaviors. Ultimately, this model
emphasizes helping the client change their
behaviors.
Theoretical Model continue
•Systemic Intervention Model-Stresses the
influence of the client’s systems. This includes
their culture, gender, spirituality, and social
environment. Systemic clinicians hypothesize
that the client’s problems are rooted in their
system. Most often this is due to either
miscommunication or lack of communication.
In addition to a difference in values and moral
among members of the system.
Clinicians Characteristics
Bilingual (Arabic/English) Preferred
Good Working Knowledge of the Arab and Chaldean culture
Warm Disposition
Strong Rapport Building Skills
Strong Listing Skills
Sensitivity to Non-Verbal Cues
Resourceful
Respectful of Client’s Uniqueness
Patience
Clinicians Characteristics continue
• Some Arab Americans and Chaldean Americans have
a preference for clinicians of their own race and
culture.
• Some clients actually have a preference for clinicians
of their own race. For example, a Lebanese client
may have preference for a Lebanese clinician.
However, in some cases, there is a preference for a
clinician of the same race but from a different
culture. For example, an Iraqi client may request an
Arab American clinician but stipulate that the clinician
be non-Iraqi.
Arab Community Center for
Economic Social Services (ACCESS)
• Historical Aspects
• Services-See Handouts
ACCESS Ambulatory Chemical Dependency Program
• Aim and purpose is to provide individual therapy to substance
abuse and substance dependence clients as part of their
continuing care treatment.
• Clients will receive comprehensive screening, psychiatric care
on an as needed basis, medical care on an as needed basis,
breathalyzer and random urine drug screens. Clients will be
admitted based on the ASAM Admission Criteria. Clients will
be treated by Certified Addiction Counselors and they will be
required to attend a minimum of 3 documented Alcoholics
Anonymous and Narcotics Anonymous meetings per week.
Resources
• Arab Community Center for Economic and Social Services (ACCESS) Accesscommunity.org
• National Institute on Drug Abuse (NIDA) nih.gov
• National Institute on Alcohol Abuse and Alcoholism nih.gov
• Substance Abuse and Mental Health Services Administration (SAMHSA) samhsa.gov
• Community Anti-Drug Coalitions of America (CADCA) www.cadca.org
• Tobacco Free Michigan (TFM) www.tobaccoofreemichigan.org
• Michigan Dept. of Community Health Tobacco Section www.michigan.gov/tobacco
• Southeast Michigan Community Alliance (SEMCA) www.semca.org
• Partnership for Drug Free America www.drugfree.org
• American Cancer Society (ACS) www.cancer.org/Healthy/StayAwayfromTobacco
• The Knopf Co. www.mi-pte.org
• Macomb County Office of Substance Abuse CMH www.mcosa.net
• Ingham County Tobacco Information www.hd.ingham.org/Home/OtherServices/TobaccoInformation
• Brighton Addiction Treatment Hospital www.brightonhospital.org
• Prosecuting Attorneys Association of Michigan www.paamtrafficsafety.com
• Michigan Multicultural Network (MCN) www.michiganmulticulturalnetwork.org
• Centers for Disease Control (CDC) www.cdc.gov/tobacco
• Addiction Technology Transfer Center Network (ATTC) www.attcnetwork.org
• Bureau of Substance Abuse and Addiction Services (BSAAS) www.michigan.gov/mdch -bsaas
Reference page
• Beck, A. T. (1976). Cognitive therapy and emotional disorders. New York:
International Universities Press.
• Bowen, M. (1978). Family therapy in clinical practice. New York: Jason Aronson.
• Foley, V. D. (1989). Family Therapy. In R.J. Corsini & D. Wedding (Eds.), Current
psychology therapies (4 th ed.). Itasca, IL: F.E. Peacock.
• Hackney, H and Cormier, S (2005). The professional counselor a process guide
to helping (5th ed.). Boston: MA.
• Lazarus, A. A. (1989). The Practice of Multimodal Therapy. Baltimore: Johns
Hopkins
•
University Press.
• Wolpe, J. (1990). The practice of behavior therapy (4th ed.). New York:
Pergamon.
Final Thoughts…
• Each consumer is unique
• Different ethnicity/race has different beliefs
• Watch for consumer cues/body language/facial expressions and
respond appropriately
• Be patient and honest
• Appreciate and respect differences
• Build trust and rapport overtime
• Provide culturally competent and bilingual services when
appropriate
• Always ask if you’re not sure and include the consumers input,
they know themselves best
Acknowledgements
• Southeast Michigan Community Alliance (SEMCA)
• MDCH Tobacco Section
• Dr. Cynthia Arfken, WSU
THANK YOU