Advocacy Initiatives

Overview
Ipas South Africa
Providers as Advocates
Values Clarification and Attitude Transformation
Community Based Advocacy
Advocacy Work – the Past
Advocacy Work – Current
Questions
2
Ipas
Non-Governmental Not for Profit Organisation that has been working in South Africa since 1995.
Only NGO focusing exclusively on Termination of
Pregnancy
Ipas is a non-profit organization that works around the world to increase women's ability to exercise their sexual and reproductive rights, especially the right to safe abortion. Ipas believes that no woman should have to risk her life, her health, her fertility, her well-being or the well-being of her family because she lacks reproductive health care and reproductive choice
3
What is Advocacy and why do we need to advocate?
Advocacy is the strategic use of information to change policies that affect people’s lives.
1. to expand the supply of quality, affordable, acceptable and accessible services for safe abortion
2. to increase the demand from women and societies for more accessible and non-judgemental care for women seeking abortion care
3. to defend the law and ensure SRH and R remain inviolate
5
Advocacy perspective
An advocacy perspective is one that sees many opportunities for influencing the community positively about the need for safe abortion care it helps us communicate with…
Our family and friends
During or private encounters with our clients
To our leaders and colleagues
In more public arenas e.g. speaking at conferences, in community meetings,
6
Some risks
Public confrontation
Political stigma
Being harassed or threatened
7
Some benefits
Helping clients access much needed services and care
Respect in the community
Successful influence on policy makers and other providers
8
Things to remember
Presenting too much or too little information to substantiate our position
Using out-dated information or information that is irrelevant or mismatched
Too much emotion can create problems
Assumptions about who is and who is not on our side
9
Advocacy roles
EDUCATOR: providers are subject matter experts, they have knowledge and experience:
we find relevant information, we communicate our knowledge and we discuss
REPRESENTATIVE: providers are witnesses, their experiences have taught them about specific issues and struggles:
We tell stories we seek compassion and we speak in public about our experiences
PERSUADER: persuaders use tools such as the latest research data, they organise community members, they deliberately manage specific topics, policies that need change
10
What is VCAT?
Both a theory and an intervention
People discovering their values through a process of honest self-examination and open-minded search for life’s truths
(Maslow, 1959 & Rogers, 1961)
Interdependent processes of reasoning, emoting and behaving
“VCAT” is the process of examining one’s basic values and reasoning for the purpose of understanding oneself, to discover what is important and meaningful”
“Valuing occurs when the head and heart…unite in the direction of action”
(John Dewey, 1939)
Values Clarification a proven method to inform people and to create a safe space for people to evaluate their beliefs and values
Not a magic bullet – needs committed leadership and follow through
12
Central Focus of VCAT
Helping people to use rational thinking and emotional awareness to examine personal behavioral patterns and to clarify and actualize their values
Thoughtful reflection, honest self-examination, and critical analysis of values and value conflicts
Structured, facilitated opportunity for people to experience new or reframed information that is designed to be accessible and relevant
13
Values Clarification and Attitude Transformation
Theoretical Framework for Personal Change
14
Commitment statements
Didactic
CTOP Act
Conscientious
Objection
SRH R&R
&
Consequences of
Unsafe abortion
Experimental
Tactile
•Singing CTOP Songs
•Touching MVA
•VCAT Exercises
Case
Studies:
Zanele’s
Story
Critical
Reflection
&
Small group discussion
Problem
Solving
&
Action Planning
Improved
KNOWLEDGE
Improved
ATTITUDES
New
ADVOCACY
BEHAVIOURS
Introduction
Community Engagement based on three objectives
1.
Develop skills and increase knowledge on Sexual and Reproductive Health Rights to:
increase contraceptive uptake avoid unwanted pregnancies seek safe abortions (including medical abortion) recognize abortion complications
2.
3.
Change social norms and practices that stigmatize abortion
Expand women's, including young women's, ability to obtain abortion including medical abortionrelated information and care
16
Some Highlights
Limpopo Program
Partnerships with CBO’s
Mphilonhle: 12 Schools, Mobile Clinics, SRH included in activities
(Rural KZN)
Mosaic: increased access to MVA & MA through opening 2 nd facility Mitchell’s Plain (Cape Town)
Masisukumeni: Men and Boys and SRH (Rural Mpumalanga)
Masimanyane: Rural Eastern Cape SRH awareness women and girls
University of Johannesburg SRH clinic (Urban Youth)
Linking the voices of the community with provincial services
Focus is on positioning TOP as part of comprehensive
Sexual and Reproductive Health.
Educate in and out of school of youth about their SRH rights and choices; lead workshops with their peers
Young Women and Abortion Study: Peri-Urban study
17
Previous Activities 2002 to 2011
Values Clarification workshops all 9 provinces for 1 st trimester access (throughout)
VC for 2 nd trimester access all 9 provinces 2008
Providers As Advocates training 2008/09
Strategic Plan for the Implementation of the CTOP
Act
Conscientious Objection Manual and Policy
Document
SRH Workshops all provinces, public and pvt sector, always include advocacy initiatives
2- year initiative (Ford Foundation) 9 CBOs in 3 Countries
Creating support for the Maputo Plan of Action :
Mozambique, South Africa and Zambia
19
Cont….
Values Clarification workshops with Communities, providers, management and provincial departments of health in Limpopo
Assisted Limpopo, Mpumalanga, Free State, North West,
Western Cape with updating of TOP policies to include MA
Continued to work with National DOH re adoption of policy
Provinces to adopt own policies from July 2010
Successfully defended the Amendment Act: Act #1 2008:
1 st quarter FY08 (National Project)
Defended the CTOP Act through submissions to Parliament
(June 2010)
Pvt Members Bill: C. Dudley – mandatory sonar, mandatory viewing of the sonar and mandatory counselling
Worked/working with SRH partners to include TOP in “National
AIDS Strategic Plan-2012-17”
20
Lessons Learned
Need to be vigorous in supporting and defending the law
Legal environment does not always translate into access
Implementation of strict selection criteria ensures that as far as possible - the correct person attends the training
Ensuring TOP is implemented through the system
(Limpopo) rather than by a person (Mpumalanga) leads to sustainability of the service
Working with CBO’s
Greater reach, larger audience, message spread
Greater knowledge = greater access
Linking CBO’s with Provincial Departments of Health
21
200
180
160
140
120
100
80
60
40
20
0
Training Totals per province
MVA Training FY08 - FY11 (Total = 482)
42
34
189
42
30
83
62
22
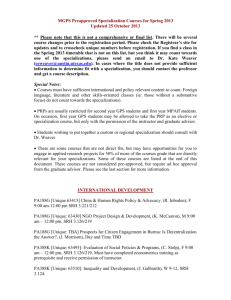
Provincial Clinical Orientations
Clinical Orientations FY08 - FY11 (Total = 511)
300
250
250
200
150
136
100
50
0
14
Eastern Cape
8
Gauteng kwaZulu Natal North West
95
8
Limpopo Western Cape
23
120
100
80
60
40
20
0
MA Refresher Training
Public Sector Private Providers
40
31
21
82
27
7
40
Pharmacists
46
45
48
24
Advocacy work limited to funding
26
Donors
Focus of Department of Health
Need to have a focused approach
Combine skills support each other
July to November 2011 VCAT
27
Questions?
28